Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
Diabetes is one of the most common diseases worldwide, with steady increase in its prevalence around the globe. One of the common and most devastating complication of such disease is diabetic foot ulcer. The prevalence of diabetic foot ulcers (DFU) among adults with diabetes globally has been estimated at 6.3%, while the annual incidence has been reported to range between 9.1 to 26.1 million cases. DFU is associated with several risk factors including a longer duration of diabetes, poorly controlled diabetes, diabetic neuropathy and foot deformities such as foot callus and flat foot. It can also result in many complications, among which infections are the leading cause of morbidity and mortality. Infections are estimated to occur in 60% of all diabetic ulcers. Moreover, the mortality rate is higher by 2.5-fold in patients with diabetes with foot ulcers compared to patients with diabetes without foot ulcers. In this chapter, we discuss the epidemiology of DFU, and review its prevalence in different parts of the world, along with risk factors, complication rates and overall impact on quality of life.
College of Medicine, Qatar University, Doha, Qatar
Amine Zaidi*
College of Medicine, Qatar University, Doha, Qatar
Basant Elsayed
College of Medicine, Qatar University, Doha, Qatar
Khaleed Jemmieh
College of Medicine, Qatar University, Doha, Qatar
Mohsen Eledrisi
Department of Medicine, Hamad Medical Corporation, Doha, Qatar
*Address all correspondence to: az1708239@student.qu.edu.qa
1. Introduction
Diabetes Mellitus is the most common metabolic disease with global prevalence of 9.3% (463 million) in 2019 and is expected to increase to 11% (700 million) by the year 2045 [1]. Patients with diabetes are prone to developing a range of complications, with the most disabling being lower extremity infections and amputations. The most common presentation of lower extremity complications is neuropathy, which is a key risk factor in developing one of the most feared and dreaded complications of diabetes, diabetic foot ulcers [2]. A trifactor of sensory, motor and autonomic neuropathy leading to loss of protective sensation, foot deformity and skin changes respectively leads to the formation of callus, which then ulcerates due to repetitive trauma and inflammation [3]. Approximately 18.6 million people with diabetes around the globe develop a foot ulcer each year [4] and 34% of all people with either type 1 or 2 diabetes will develop a foot ulcer within their lifetime [2].
Diabetic foot ulcers cause a considerable global disability burden. It is estimated that almost 20% of all diabetic foot ulcers (DFUs) eventually lead to amputations [5]. Diabetes-related lower-extremity complications account for up to 80% of all lower-extremity amputations and are a leading cause of hospitalization worldwide [6]. Furthermore, studies have shown DFU to be a cause of poorer quality of life [7] and therefore a major contributor to the global disability burden. In 2016, it was estimated that 2.1% of the global years lived with was directly caused by diabetes-related lower-extremity complications. Increased pain, poor physical function, poorer prognosis for other health conditions and lower quality of life overall are just some of the health impacts that can affect persons living with DFU [7].
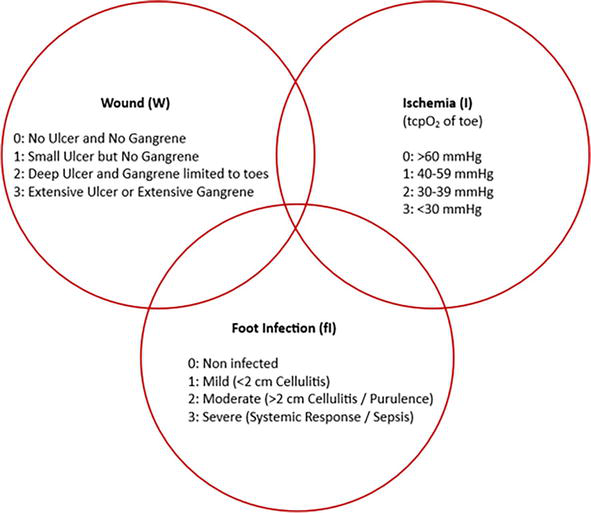
The Society for Vascular Surgery in 2013 proposed a classification system, that incorporates the three most important risk factors of amputation; wound, ischemia, and foot infection [8]. The wound, ischemia, and foot infection (WIfI) classification system gives a rating that ranges from 0 to 3 for each risk factor, in which 0 represents absent, 1 mild, 2 moderate and 3 severe (Figure 1). The individual scores are combined and then the total number is analyzed using two tables (Tables 1 and 2): one table estimates the risk of amputation at 1 year and the other table estimates the need for revascularization. The limb is classified in terms of both, risk of amputation and need for revascularization, into four categories: very low, low, moderate and high [9, 10]. It is proven that this classification system is an independent predictor of wound healing in patients with DFUs [10]. WIfI scores of 1,2,3 and 4 have been associated with 1-year amputation rates of 0, 8, 11, and 38% respectively [6]. These classification tools play a vital role in determining the patient’s prognosis as well as the modality of treatment offered. Currently, more research is being looked into for early and aggressive management of DFU due to its severe complications that have health impacts and financial impacts.
Figure 1.
The WIfI classification system. tcpO2 = transcutaneous oxygen pressure.
Ischemia 0
Ischemia 1
Ischemia 2
Ischemia 3
Wound 0
VL
VL
L
M
VL
L
M
H
L
L
M
H
L
M
M
H
Wound 1
VL
VL
L
M
VL
L
M
H
L
M
H
H
M
M
H
H
Wound 2
L
L
M
H
M
M
H
H
M
H
H
H
H
H
H
H
Wound 3
M
M
H
H
H
H
H
H
H
H
H
H
H
H
H
H
fI 0
fI 1
fI 2
fI 3
fI 0
fI 1
fI 2
fI 3
fI 0
fI 1
fI 2
fI 3
fI 0
fI 1
fI 2
fI 3
Table 1.
Estimation of risk of amputation at 1 year.
VL = very low; L = low; M = moderate; H = high; fI = foot infection.
Ischemia 0
Ischemia 1
Ischemia 2
Ischemia 3
Wound 0
VL
VL
VL
VL
VL
L
L
M
L
L
M
M
M
H
H
H
Wound 1
VL
VL
VL
VL
L
M
M
M
M
H
H
H
H
H
H
H
Wound 2
VL
VL
VL
VL
M
M
H
H
H
H
H
H
H
H
H
H
Wound 3
VL
VL
VL
VL
M
M
M
H
H
H
H
H
H
H
H
H
fI 0
fI 1
fI 2
fI 3
fI 0
fI 1
fI 2
fI 3
fI 0
fI 1
fI 2
fI 3
fI 0
fI 1
fI 2
fI 3
Table 2.
Estimation of the need for revascularization.
VL = very low; L = low; M = moderate; H = high; fI = foot infection.
2. Epidemiology and recurrence rate of diabetic foot ulcer
Diabetic foot ulcers are more common in men compared to women, and more prevalent in patients with type 2 diabetes compared to those with type 1 diabetes [11].
2.1 Global and regional prevalence rates of diabetic foot ulcer
Globally, the impact of DFU is staggering. According to the International Diabetes Foundation, between 40 to 60 million individuals are currently suffering from diabetic foot ulcers [11]. However, it is crucial to approach these prevalence figures with a discerning perspective, as they can be easily influenced through various methods, such as different surveillance approaches, and definitions of diabetic foot ulcer. In 2017, a meta-analysis carried out Zhang, P et al. reported that the global prevalence of DFU among adults with diabetes was 6.3% which translates to an estimated 33 million people [11]. The annual incidence of DFU has been reported to be between 9.1 to 26.1 million [2]. The occurrence rate of diabetic foot ulcers throughout a patient’s lifetime has been reported to range between 12–25% [11]. However, it has been reported that potential lifetime risk could be even greater due to the extended life expectancy [2]. Furthermore, the overall recurrence was estimated to be 22.1% per person-year [12].
In African nations (excluding North Africa), the prevalence of DFU has been observed to range between 10 and 30% [13]. This situation is expected to further escalate as the International Diabetes Foundation is anticipating a rise in the number of patients with diabetes in Africa. In Tanzania, Abbas et al. (n.d.), have documented a 17.5% prevalence of neuro-ischemic ulcer lesions among patients with diabetes [13]. Similarly, in Ethiopia, Tolosa et al. reported an overall magnitude of foot ulcers of 12.98% in patients with diabetes [14]. A separate study further conducted in Tanzania revealed that around 15% of patients with diabetes who were admitted to inpatient services had foot ulcers, with 80% of these cases being individuals with no previous history of ulcers. A similar rate has also been reported in Mogadishu, and Somalia [15]. Moreover, in Kenya, the rate was estimated to be 9.04% [16]. The elevated prevalence of DFU can be attributed to the common practice of walking barefoot, which is practiced in rural communities in Africa. Furthermore, the limited income in these regions makes it difficult for individuals with diabetes to procure appropriate footwear, further contributing to the issue [17]. The recurrence rate of diabetic foot ulcers in African nations was found to be relatively low, reaching 16.9% [12].
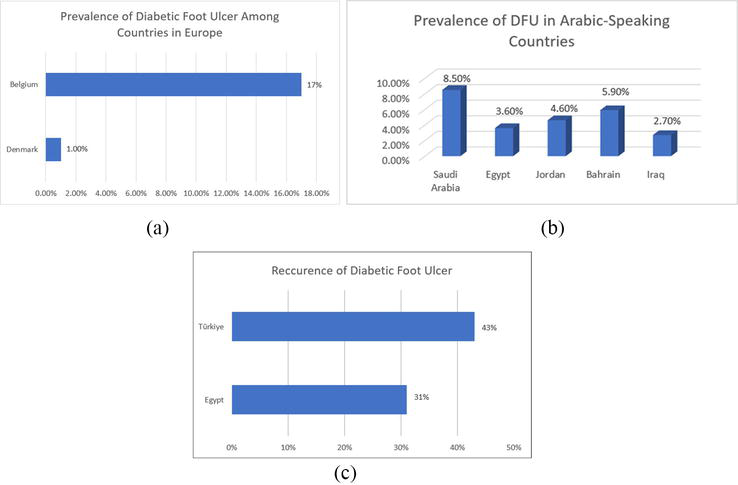
In Europe, 1 in 11 adults has diabetes, mounting to – 61 million individuals [18]. This region also bears the highest number of children and adolescents with type 1 diabetes, reaching around 295,000 individuals [18]. The prevalence of DFU varies significantly, ranging from 1% in Denmark to a remarkable 17% in Belgium (Figure 2a). Likewise, the recurrence rate has also demonstrated wide variation as well. This is evident by the fact that it stood at 7% in Germany and Italy in 2012, but then surged to 42% in Italy by 2017. In a recent study conducted in Belgium, it was concluded that diabetic foot ulcers were more prevalent in men compared to women and were presented in a more severe form [19]. Furthermore, according to Grand View Research (n.d.), the European diabetic foot ulcer treatment market size was valued at 1.45 billion USD in 2021 and it is expected to increase at a compound annual growth rate of 5.4% between 2022 and 2030 [20].
Figure 2.
a. Displays the prevalence of diabetic fot ulcer among countries in Europe. b. Displays the prevalence of DFU in countries in which Arabic is the official language. c. Displays the rate of recurrence of diabetic foot ulcer in Egypt and Türkiye.
In North America & Caribbean, approximately 1 in 7 adults have diabetes, totaling 51 million individuals [21]. This region also accounts for the highest diabetes-related expenditure, reaching 415 billion USD, which constitutes around 43% of global expenditure [21]. The prevalence of DFU in North America was around 13% [13]. The frequency of DFU recurrence ranged from 9% in 2013 to 52% in 2018 [22].
In South and Central America, 1 in 11 adults have diabetes, totaling 33 million individuals [23]. Carro, G et al. (2018), concluded in their transversal study the prevalence of DFU across 9 Latin American countries was 14.8% [24]. while the prevalence in Brazil was 21%.
In the Middle East and North Africa (MENA) region, 1 in 6 adults currently live with diabetes — an estimated 73 million individuals. It is predicted that the prevalence of diabetes will increase by 86%, reaching 136 million by the year 2045 [25]. The prevalence of diabetic foot ulcers in this region has been estimated to range between 5 and 20% [26]. Furthermore, in a systemic review conducted in Arabic-speaking countries, the prevalence of DFUs was found to be as follows: Saudi Arabia (8.5%), Egypt (3.6%), Jordan (4.6%), Bahrain (5.9%), and Iraq (2.7%) (Figure 2b) [27]. Recurrence of DFU varied widely; as an example, it was 31% in Egypt and 43% in Türkiye (Figure 2c) [25].
In the Southeast Asian region, approximately 1 in 11 adults are affected by diabetes, approximated to be around 90 million individuals. This number is expected to increase by 69%, reaching 152 million by the year 2045. The prevalence of DFU in this region was 15%, with a recurrence rate of less than 14% [28]. A recent meta-analysis concluded that the prevalence of diabetic foot ulcers in Pakistan was 12.16% [29].
The data shows not only the staggering prevalence of diabetes and DFU that currently exists but also points to a further increase in the future.
A plethora of risk factors associated with DFU has been studied. The common underlying risk factors are poor glycemic control, improper foot care, underlying peripheral neuropathy and poor circulation. In addition, foot deformities such as calluses, dry poorly perfused and flat foot were considered important risk factors for DFU. A study in Sudan described the duration of diabetes for >10 years as the only statistically significant risk factor associated with diabetic foot ulcers [30]. Other factors such as hypertension, HbA1c, lipid levels, albuminuria, retinopathy, age and BMI were not associated with the development of DFU [30]. A nationwide systemic review in Ethiopia described that diabetic foot ulcers were significantly associated with the following risk factors: having callus on the foot, high BMI, poor self-care practice, type 2 diabetes and living in urban areas, while younger patients (<45 years) and those who have diabetes for <10 years were found to have decreased odds of diabetic foot ulcers [14]. Although DFUs are more common among male patients along with a tendency to progress to amputation [31], no significant association was found in this study between gender and DFU [14].
3.2 Risk factors for recurrent DFU
Demographic factors like male gender and smoking were associated with an increased incidence of DFU recurrence while age and BMI were not predictors of DFU recurrence. Also, patients having a long duration of diabetes were at a significant risk of DFU recurrence. Among different forms of DFU, patients with previous plantar ulcers were at a higher risk of DFU recurrence. No association was found between the recurrence of DFU and any of the following: age, BMI, long duration of past DFUs, hypertension, high cholesterol, nephropathy and retinopathy [32]. Patients with peripheral artery disease, diabetic neuropathy and impaired proprioception were at a significant risk of DFU recurrence [32, 33].
3.3 Financial cost of diabetic foot ulcers
The annual expenditure for any medical performance per person with diabetic foot complications was 3 times higher than that for diabetic patients without DFUs [34]. In 2017, it was estimated that the complications of diabetes in the United States carried a direct cost of $237 billion; historically approximately 33% of this cost has been accepted as attributable to DFUs [31]. Costs have been demonstrated to correlate with wound severity. The cost of individual hospitalizations for DFUs has also increased significantly independent of amputation rate and length of stay, demonstrating the importance of avoiding inpatient admissions in this patient population when possible [31].
Moreover, due to the nature of DFU, several teams are consulted for adequate management of DFU during hospitalization. This ranges from internists, endocrinologists, and surgeons to specialized services such as podiatrists and physiotherapists. Henceforth, hospital admission for patients with DFU represents one of the largest direct expenditures. Moreover, high recurrence rates for DFU, (up to 22.1% per person-year) [12], lead to recurrent hospital admissions, impaired quality of life and low productivity, which further increase the expenses.
Although the costs of DFU treatment were higher in developed and high-income countries such as the US ($10.9 billion/year), the UK ($4 billion/year) and Denmark ($150 million/year) [35], the condition has also a profound impact on the economy of middle- and low-income countries. As an example, in India, an average salary of 5.7 years will be needed to completely treat a patient with DFU [36]. Annual admission costs related to DFU were at $264 million in Brazil [37], and in Turkey, 3% of annual health expenditure was spent on DFU management alone [38].
The huge financial impact of DFUs calls for the importance of early identification and proper aggressive treatment of patients with diabetes and DFU to prevent its progression and reduce its economic burden. According to the Markov model for cost-effectiveness, targeted preventative strategies have the scope of reducing amputations and DFU incidence by almost 25%, and if these measures are applied, the likelihood of cost savings is more than 90% when dealing with DFU [39].
Studies show that although the cost is great, low cost, early implemented measures can go a great way in helping us to decrease those costs [40].
Diabetic foot ulcers may result in several complications, some of which can be life-threatening. In this section of this chapter, we will focus on the epidemiology of these complications and their associated morbidity.
4.1 Infection
Foot infection is a leading cause of morbidity in patients with diabetes, occurring in 60% of diabetic foot ulcers [41]. Hence, such infections are a common cause of emergency department visits and hospital admissions. Foot ulcers usually precede the development of infection and infection rates are observed to be higher in patients with recurrent wounds, chronic non-healing wounds, wounds with a positive probe-to-bone test, and recent infections not related to the foot [42]. Infections associated with diabetic foot ulcers can range from superficial ones such as cellulitis to life-threatening conditions such as necrotizing fasciitis and sepsis [43]. In just more than 65% of patients with diabetic foot ulcers, infections are the leading cause of major lower extremity amputation and about 20% of moderate to severe infections lead to amputations [3, 44]. Osteomyelitis occurs in 15–20% of diabetic foot ulcers and is considered one of the most common manifestations of diabetic foot infections. It is estimated to occur in >20% of moderate infections and just more than half of severe infections [44, 45, 46]. Osteomyelitis most commonly affects the forefoot (90%), followed by the midfoot (5%) and least commonly the hindfoot (5%). Forefoot osteomyelitis appears to have the best prognosis as the risk of major amputation for such cases is less than 1% whereas that of hindfoot osteomyelitis is estimated to be at 50% [44].
4.2 Amputation
In a multicentric study based in Europe, it was found that 5% and 17% of patients with diabetic foot ulcers require major (above the ankle) and minor (below the ankle) amputation respectively, within 1 year of ulcer development [41]. Foot ulcers appear to be very prevalent in diabetic patients who require amputation as 85% of all amputations in patients with diabetes were preceded by foot ulcers [46]. A meta-analysis involving 16 studies revealed that the prevalence of lower limb amputation in patients with diabetic foot ulcers is around 19% [47].
4.3 Mortality
Mortality rates associated with the development of a DFU are estimated to be 5% in the first 12 months. Whereas the 5-year-mortality rate is 30–42% and exceeds 70% for those with major amputations [3, 48]. The 3-year survival rate is 72% for diabetic patients with foot ulcers compared to 87% for diabetic patients without foot ulcers [49]. One study that compares death in the presence or absence of ulcers revealed that the mortality rate for people with diabetic foot ulcers is 231 deaths per 1000 person-years, compared with 182 deaths per 1000 person-years in people with diabetes without foot ulcers [3]. In a study conducted in the UK involving 20,737 patients with diabetes who newly developed foot ulcers, it was found that 5% of patients died within 1 year of their first foot ulcer visit and just more than 40% died within 5 years [50]. The study also found that death is 2.5 times more likely in diabetic patients with foot ulcers compared to those without foot ulcers. Surprisingly, the 5-year mortality rate of patients with diabetic foot ulcers seems to be comparable to that of pooled 5-year survival of all cancers and even greater in some studies [51].
4.4 Disability and low quality of life
Diabetic foot ulcers have a significant impact on the quality of life and well-being of individuals regardless of the presence of other diabetes-related complications that influence the quality of life [50]. This low quality of life is reflected by questionnaires, such as SF-36, which shows that the most significantly impacted domains are physical functioning, productivity, general health, and depressive symptoms [7]. The healing status of ulcers also seems to have an impact on welfare as patients with unhealed ulcers are more anxious and frustrated than those with healed ones [50]. Anxiety and depression seem to be fairly prevalent in patients with diabetic foot ulcers, with reported prevalence rates of 13.8 and 20%, respectively [52]. In terms of Years Lived with Disability (YLD), it is estimated that 2.5 million YLDs result from foot ulcers [46].
Diabetes is the most common metabolic disease worldwide and its prevalence and complications are on the rise. Diabetic foot ulcers are common complications of diabetes that can affect a wide range of patients around the globe, have shown increasing trends over the last decades and are associated with increased morbidity and mortality. Diabetic foot ulcers can result in significant medical, psychological, and financial consequences to patients, their families and society. Diabetic foot ulcers are a major cause of infections, lower limb amputations, disability, reduced quality of life, higher mortality and increased economic burden.
1.Saeedi P et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the international diabetes federation diabetes atlas, 9(th) edition. Diabetes Research and Clinical Practice. 2019;157:107843
2.Armstrong DG, Boulton AJM, Bus SA. Diabetic foot ulcers and their recurrence. The New England Journal of Medicine. 2017;376(24):2367-2375
3.Armstrong DG et al. Diabetic foot ulcers: A review. JAMA. 2023;330(1):62-75
4.Zhang Y et al. Global disability burdens of diabetes-related lower-extremity complications in 1990 and 2016. Diabetes Care. 2020;43(5):964-974
5.Pickwell K et al. Predictors of lower-extremity amputation in patients with an infected diabetic foot ulcer. Diabetes Care. 2015;38(5):852-857
6.Kerr M et al. The cost of diabetic foot ulcers and amputations to the National Health Service in England. Diabetic Medicine. 2019;36(8):995-1002
7.Khunkaew S, Fernandez R, Sim J. Health-related quality of life among adults living with diabetic foot ulcers: A meta-analysis. Quality of Life Research. 2019;28(6):1413-1427
8.Mills JL Sr et al. The Society for Vascular Surgery Lower Extremity Threatened Limb Classification System: Risk stratification based on wound, ischemia, and foot infection (WIfI). Journal of Vascular Surgery. 2014;59(1):220-34.e1-2
9.Cerqueira LO et al. WIfI classification: The Society for Vascular Surgery lower extremity threatened limb classification system, a literature review. Jornal Vascular Brasileiro. 2020;19:e20190070
10.Hicks CW et al. The Society for Vascular Surgery Wound, ischemia, and foot infection (WIfI) classification independently predicts wound healing in diabetic foot ulcers. Journal of Vascular Surgery. 2018;68(4):1096-1103
11.Zhang P et al. Global epidemiology of diabetic foot ulceration: A systematic review and meta-analysis (†). Annals of Medicine. 2017;49(2):106-116
12.Fu XL et al. Global recurrence rates in diabetic foot ulcers: A systematic review and meta-analysis. Diabetes/Metabolism Research and Reviews. 2019;35(6):e3160
13.Abbas ZG, Boulton AJM. Diabetic foot ulcer disease in African continent: 'From clinical care to implementation'—review of diabetic foot in last 60 years—1960 to 2020. Diabetes Research and Clinical Practice. 2022;183:109155
14.Tolossa T et al. Prevalence and associated factors of foot ulcer among diabetic patients in Ethiopia: A systematic review and meta-analysis. BMC Public Health. 2020;20(1):41
15.Salad AM et al. Prevalence of diabetes foot ulcers and associated factors among adult diabetic patients in three referral hospitals in Mogadishu, Somalia. Frontiers in Public Health. 2023;11:1195483
16.Wincate Maingi GK, Matheri J. Prevalence and factors associated with diabetic foot ulcer among adult patients attending diabetic clinic at Nyeri level 5 hospital. African Journal of Health Sciences. 2020;33:44-52
17.Boateng D et al. Contribution of diabetes to amputations in sub-Sahara Africa: A systematic review and meta-analysis. Primary Care Diabetes. 2022;16(3):341-349
18.Diabetes in Europe in 2021 [Internet]. Diabetes Atlas. Belgium: International Diabetes Foundation; 2021 [cited 2023]. Available from: https://diabetesatlas.org/regional-factsheets/
19.Vanherwegen AS et al. Sex differences in diabetic foot ulcer severity and outcome in Belgium. PLoS One. 2023;18(2):e0281886
20.GVR Report Cover, Europe Diabetic Foot Ulcer Treatment Market Size, Share & Trends Report Europe Diabetic Foot Ulcer Treatment Market Size, Share & Trends Analysis Report by Treatment (Biologics, Wound Care Dressings), by Ulcer Type (Neuro-Ischemic, Ischemic, Neuropathic), and Segment Forecasts. [Internet]. www.grandviewresearch.com. Grand View Research. San Francisco, Cal; [cited 2023]. Available from: https://www.grandviewresearch.com/industry-analysis/europe-diabetic-foot-ulcer-treatment-market-report
21.Diabetes in North America and Caribbean in 2021 [Internet]. Diabetes Atlas. Belgium: International Diabetes Foundation; 2021 [cited 2023]. Available from: https://diabetesatlas.org/regional-factsheets/
22.Gamboa-Antiñolo F-M. Diabetic foot ulcers: A growing global health emergency in the COVID-19 era. Internal and Emergency Medicine. 2023;18(5):1259-1261
23.Diabetes in South and Central America in 2021 [Internet]. Diabetes Atlas. Belgium: International Diabetes Foundation; 2021 [cited 2023]. Available from: https://diabetesatlas.org/regional-factsheets/
24.Carro GV et al. Diabetic foot among hospitalized patients in Latin America. Medicina (B Aires). 2018;78(4):243-251
25.Diabetes in Middle East and North Africa in 2021 [Internet]. Diabetes Atlas. Belgium: International Diabetes Foundation; 2021 [cited 2023]. Available from: https://diabetesatlas.org/regional-factsheets/
26.Monteiro-Soares M, Santos JV. Diabetes foot-related complications [Internet]. In: Magliano D, Boyko E, Genitsaridi I, Piemonte L, Riley P, Salpea P, editors. Diabetes Atlas. Belgium: International Diabetes Foundation; 2022 [cited 2023]. Available from: https://diabetesatlas.org/atlas/diabetic-foot-2022/
27.Mairghani M et al. The prevalence and incidence of diabetic foot ulcers among five countries in the Arab world: A systematic review. Journal of Wound Care. 2017;26(Suppl. 9):S27-S34
28.Diabetes in South East Asia in 2021 [Internet]. Diabetes Atlas. Belgium: International Diabetes Foundation; 2021 [cited 2023]. Available from: https://diabetesatlas.org/regional-factsheets/
29.Akhtar S et al. The prevalence of foot ulcers in diabetic patients in Pakistan: A systematic review and meta-analysis. Frontiers in Public Health. 2022;10:1017201
30.Almobarak AO et al. Prevalence of diabetic foot ulceration and associated risk factors: An old and still major public health problem in Khartoum, Sudan? Annals of Translational Medicine. 2017;5(17):340
31.Sorber R, Abularrage CJ. Diabetic foot ulcers: Epidemiology and the role of multidisciplinary care teams. Seminars in Vascular Surgery. 2021;34(1):47-53
32.Huang Z-H et al. Risk factors for the recurrence of diabetic foot ulcers among diabetic patients: A meta-analysis. International Wound Journal. 2019;16(6):1373-1382
33.Hicks CW et al. Incidence and risk factors associated with ulcer recurrence among patients with diabetic foot ulcers treated in a multidisciplinary setting. The Journal of Surgical Research. 2020;246:243-250
34.Lin CW et al. Nationwide trends in the epidemiology of diabetic foot complications and lower-extremity amputation over an 8-year period. BMJ Open Diabetes Research & Care. 2019;7(1):e000795
35.Jodheea-Jutton A, Hindocha S, Bhaw-Luximon A. Health economics of diabetic foot ulcer and recent trends to accelerate treatment. The Foot. 2022;52:101909
36.Karri VVSR. Current perspective in the management of diabetic foot ulcers—an overview on the Indian scenario. International Journal of Pharmacy and Pharmaceutical Sciences. 2014;6
37.Rezende KF et al. Predicted annual costs for inpatients with diabetes and foot ulcers in a developing country-a simulation of the current situation in Brazil. Diabetic Medicine. 2010;27(1):109-112
38.Oksuz E et al. Cost of illness among patients with diabetic foot ulcer in Turkey. World Journal of Diabetes. 2016;7(18):462-469
39.Barshes NR et al. A model to estimate cost-savings in diabetic foot ulcer prevention efforts. Journal of Diabetes and its Complications. 2017;31(4):700-707
40.Rankin TM et al. Illustration of cost saving implications of lower extremity nerve decompression to prevent recurrence of diabetic foot ulceration. Journal of Diabetes Science and Technology. 2015;9(4):873-880
41.Prompers L et al. Prediction of outcome in individuals with diabetic foot ulcers: Focus on the differences between individuals with and without peripheral arterial disease. The EURODIALE Study. Diabetologia. 2008;51(5):747-755
42.McDermott K et al. Etiology, epidemiology, and disparities in the burden of diabetic foot ulcers. Diabetes Care. 2022;46(1):209-221
43.Armstrong DG, Lipsky BA. Diabetic foot infections: Stepwise medical and surgical management. International Wound Journal. 2004;1(2):123-132
44.Giurato L et al. Osteomyelitis in diabetic foot: A comprehensive overview. World Journal of Diabetes. 2017;8(4):135-142
45.Lázaro Martínez JL et al. Optimal management of diabetic foot osteomyelitis: Challenges and solutions. Diabetes, Metabolic Syndrome and Obesity. 2019;12:947-959
46.Edmonds M, Manu C, Vas P. The current burden of diabetic foot disease. Journal of Clinical Orthopaedics and Trauma. 2021;17:88-93
47.Rodrigues BT et al. Prevalence and risk factors of lower limb amputations in patients with diabetic foot ulcers: A systematic review and meta-analysis. Diabetes & Metabolic Syndrome: Clinical Research & Reviews. 2022;16(2):102397
48.Walsh JW et al. Association of diabetic foot ulcer and death in a population-based cohort from the United Kingdom. Diabetic Medicine. 2016;33(11):1493-1498
49.Ramsey SD et al. Incidence, outcomes, and cost of foot ulcers in patients with diabetes. Diabetes Care. 1999;22(3):382-387
50.Goodridge D et al. Quality of life of adults with unhealed and healed diabetic foot ulcers. Foot & Ankle International. 2006;27(4):274-280
51.Armstrong DG et al. Five year mortality and direct costs of care for people with diabetic foot complications are comparable to cancer. Journal of Foot and Ankle Research. 2020;13(1):16
52.Polikandrioti M et al. Quality of life in diabetic foot ulcer: Associated factors and the impact of anxiety/depression and adherence to self-care. The International Journal of Lower Extremity Wounds. 2020;19(2):165-179
Written By
Ahmed Daniyal Nawaz, Amine Zaidi, Basant Elsayed, Khaleed Jemmieh and Mohsen Eledrisi
Submitted: 16 September 2023Reviewed: 03 November 2023Published: 08 February 2024