Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
This chapter aims to explore the clinical features and effective management strategies for diabetic foot ulcers (DFUs), which, if not appropriately treated, can lead to serious consequences and ultimately require amputation. It is crucial to adopt a comprehensive approach that encompasses accurate diagnosis and effective treatment plans. These ulcers have a multifactorial etiology and a wide range of clinical features that can be attributed to the ulcers themselves, the underlying causes contributing to their development, or their complications, particularly infections. However, timely and accurate diagnosis can be challenging due to a lack of sensation, making risk factor assessments and severity assessments through various classification systems necessary. Managing DFUs effectively requires a multidisciplinary approach that includes optimum glycemic control, performing wound debridement, relieving pressure from the affected area, controlling infections, and utilizing appropriate dressings.
*Address all correspondence to: ra1902557@qu.edu.qa
1. Introduction
The etiology of diabetic foot ulcers (DFUs) is multifactorial [1]. It often includes neuropathies, vasculopathies, immunopathies, foot deformities, biomechanical defects, suboptimal management of blood glucose as well as neglecting appropriate foot care, using inappropriate footwear, and foot skin dryness [1, 2, 3, 4].
Neuropathy is found in more than 80% of DFU patients [2, 3]. The sensory, motor, and autonomic nervous systems may be affected as a consequence of diabetic neuropathy [3].
Sensory neuropathy alters and reduces the perceptions of pain and pressure. The patient will normally present with altered sensations of the foot including paresthesia, hyper/hypoesthesia, and dysesthesia [1]. Due to loss of sensation, repetitive trauma and injury may occur with the patient none the wiser, preceding an ulcer; this might be due to footwear that is ill-fitted or small sprains and strains [3]. As a result, patients tend to seek care at a later, more severe stage. Since diabetic neuropathy can influence multiple body systems (autonomic neuropathy), it might also compromise the foot microcirculation, as well as result in skin changes, such as dry skin [2].
Motor neuropathy results in weakened intrinsic muscles and collapse of anatomical structures of the foot leading to deformities such as hammer toes, Charcot foot etc. [2]. These malformations can alter the distribution of pressure across the foot, deeming particular areas increasingly predisposed to injury and ulcer formation [3]. Pressure changes and loss of sensation also contribute to the formation of calluses [1].
Autonomic neuropathy will affect the integrity of the skin, since the autonomic nervous system acts on the blood vessel network as well as the physiological secretions. This will present as anhidrosis causing skin dryness, flaking, and increasing fragility. This renders the skin more vulnerable to dermal deterioration and fissure formation, increasing susceptibility to infection [3]. Changes in nail health (brittle nails) might be present [1].
2.1.1 Diabetic foot deformities
In conjunction with neuropathy and injury, foot deformity was asserted by the Task Force of the Foot Care Interest Group of the American Diabetes Association as the most prevalent trio of interconnected factors that will ultimately lead to the formation of ulcers [1, 5]. Some of the most prevalent anatomical deformities include deformities of the metatarsophalangeal joint, interphalangeal joint and prominent metatarsals. For instance, claw foot (pes cavus) manifests as flexed interphalangeal joints and hyperextended metatarsophalangeal joints while hyperextension of the metatarsophalangeal joint and distal interphalangeal joint along with flexion of the proximal interphalangeal joints indicate hammer toes [3, 6, 7]. In addition, other common deformities include pes equinus presenting with limited dorsiflexion of the foot due to tightness in the Achilles tendon and hallux valgus (bunions) characterized by the lateral deviation of the first metatarsal among others [6, 7]. These changes in the anatomical structure can limit joint movement and intensity pressure on the plantar surface [8].
The genesis of these deformities remains poorly established. A literature review conducted in 2016 discussed that there is no substantial evidence to uphold the widely held notion that foot deformities arise due to motor neuropathy leading to atrophy and imbalances of the muscles [6]. However, weak muscles and limited joint mobility were found to be linked with foot deformities and unsteady gait was linked with all the aforementioned [6].
Gait pattern can be altered in diabetic individuals [9]. A study in 2020 established gait analysis as a useful assessment for the identification of individuals at risk of ulceration [10]. They found that diabetes patients with no alteration of anatomical structures in the foot exhibited gait abnormalities like lateral shift of peak pressure when walking and elevated peak pressure at the medical heel region in those with diabetic neuropathy. Elevated peak plantar pressures and altered pressure distribution were found prior to the formation of foot deformities and deterioration of soft tissue on the underside of the foot that will lead to ulcer formation. Dynamic plantar pressure analysis is a valuable tool for diagnosis and proactive prevention of foot deformities [10].
2.1.2 Charcot neuropathic osteoarthropathy (CNO)
CNO is a chronic inflammatory condition affecting individuals with diabetic neuropathy and those with peripheral neuropathy [11, 12]. Osseous, joint, and soft tissue damage, usually in the foot and ankle, may or may not be associated with pain and might result in chronic alterations of the foot’s anatomical structure due to fractures, dislocations, and fracture-dislocations [11, 12]. Typically, clinical manifestations include a swollen and erythematous joint with a 2°C increase in temperature in comparison to the unaffected joint [13, 14]. CNO is distinguished by four stages similar to the active and inactive phases of disease including inflammation, fragmentation, coalescence, and consolidation. In the active phase, the foot becomes inflamed and often painless because of neuropathy [15]. In addition, transient osteopenia can lead to bone fragility resulting in fractures, joint destruction, and collapse of the foot’s longitudinal arch [16, 17]. Meanwhile in the inactive phase, the erythema will have subsided, but some swelling of the bone marrow and soft tissues might remain. Notable joint and bone damage precedes bone overgrowth that consequently leads to prominent osteophytes (bone spurs) and palpable loose fragments within the joint [16, 17].
The most used staging system is the Eichenholtz staging system assessed via clinical manifestations and radiology [18]. In stage 0, there is little inflammation, swelling of soft tissue, and insignificant x-ray findings. However, magnetic resonance imaging (MRI) findings demonstrate microfractures, bone marrow edema, and bone contusion [19]. Recognizing and managing the disease at this stage aids in the prevention of foot deformities [20, 21]. Stage 1 (fragmentation) is marked by soft tissue swelling and inflammation becomes severe. Macro-fractures are seen on x-ray and on MRI as well, which shows bone marrow swelling, in addition to bone resorption initiated with joint dislocations [19]. Bone remodeling commences as the fracture heals and the debris is resorbed marking the end of bone resorption characterizing stage 2 (coalescence). Stage 3 (consolidation) represents the last stage of bone remodeling and reconstruction. This stage marks the transition to the chronic CNO phase in which ulcers occur frequently and substantial structural alterations are undergone by the arch of the foot [19]. The final stage of CNO is known as rocker-bottom deformity [22].
2.2 Vasculopathy
Decreased tissue perfusion can, in addition to other factors like co-existing chronic conditions and infections, hinder the wound healing process, impair the body defense system, and increase the risk of ulcerations [3]. This peripheral ischemia of large and small vessels can also increase the risk of infection and might chronically lead to the foot becoming gangrenous and thus, amputated [23]. It may be classified into macro- or microvascular disease. Macrovascular refers to peripheral arterial disease (PAD) in which the arteries of the upper or lower limbs are narrowed or occluded. Etiologies of PAD include emboli, thrombi, or vasculitis and PAD is believed to be a contributor to lower limb complications [3, 24]. However, atherosclerosis is usually the primary etiology of which diabetes is considered a risk factor as discussed by [25].
Microvascular disease refers to the damage of small blood vessels caused by diabetes mellitus. These small vessels may show capillary wall thickening, sclerotic vessel walls, endothelial proliferation, and damage [3, 26]. It can affect various organs and tissues in the body and can impair the healing of the skin, especially in the lower extremities resulting in ulcers, infections, or gangrene.
Symptoms that are indicative of PAD include intermittent claudication, which is pain reminiscent of cramps in the leg, usually upon physical activity, and is found in 10% of individuals with PAD, while pain during inactivity might signify critical limb ischemia [27, 28]. About half of individuals with PAD will not experience any symptoms [27]. Upon examination, skin alterations related to ischemia might be present in some patients; ischemia associated trophic changes can include alopecic skin changes and glossy and lustrous skin, in addition to cool feet [3, 27]. However, note that hairless skin is clinically of little value as an indicator of ischemia [28]. Furthermore, patients with PAD can also present with postural erythema due to reduced blood flow and postural pallor upon elevation of the leg. Peripheral pulses may also be abated, especially the femoral artery, popliteal artery, posterior tibial artery, and dorsalis pedis artery [27]. It is crucial to examine regions of pressure in the foot like the plantar region, the calcaneal area, the area posterior to the malleolus, and the metatarsal heads, in addition to the interdigital area. Important to note is that the presence of blisters in a foot with ischemia foretells ulceration [28].
2.3 Infections in DFU: Clinical presentation
Diabetic foot infections can present in about 58% of individuals with an acute foot ulcer [3]. It negatively affects the quality of life as reported by individuals with diabetic foot infections [29]. The infection is initiated by the invasion of microorganisms in the ulcerated area of broken-down skin. Later, the microorganism colonizes the region and triggers an inflammatory response that will induce a breakdown of tissue [3]. Due to the abnormal mechanism of the white blood cell immune response, patients might not present with the classic manifestations of infection, such as fever, fatigue, nausea, vomiting etc. [30]. Among the most preliminary presentations of a diabetic foot infection is elevated blood glucose of unknown etiology. Patients may present with manifestations of the “diabetic flu” as well, such as nausea, vomiting, anorexia, fever, and chills; the foot must be closely inspected for infections or ulcers in this case [31].
For identification of an infection, it is most important to look for a history of chills and fever and upon the examination of the foot, the existence of pus and a minimum of two manifestations of inflammation including pain, a rise in temperature, redness, and rigidity of tissue surrounding the ulceration area [1]. A probe to bone test is conducted with a sterile, blunt metal probe on the ulcer; if the bone can be palpated by the probe, it is indicative of osteomyelitis and is especially useful for patients with diabetes [32, 33, 34]. The risk factors that exhibit higher odds of diabetic foot infections comprise palpable bone in probe to bone test, ulcers lasting for more than 30 days, reoccurring ulcers, traumatic ulcers, and having PAD, in that order [35].
Diabetic foot infections are classified into no infection where the patient does not possess any of inflammatory signs discussed above [36]. Mild infection is characterized by there being pus, any two of the signs of inflammation, and any cellulitis or redness that is localized to 2 cm or less around the ulcer and does not go deeper than superficial subcutaneous tissue. Moderate infection includes the previous but might extend above 2 cm surrounding the ulceration and can extend to the bone and might involve gangrene as well. The severe stage of infection can involve all of the above in addition to being metabolically unstable and presenting with signs of systemic toxicity such as fevers, chills, low blood pressure, confusion, elevated blood glucose, and acidosis among others [36].
2.4 Classifications
Classifications of diabetic foot ulcers are systems that help to describe the characteristics and severity of the ulcers, as well as to predict the outcomes and guide the treatment. Although there are several classifications of diabetic foot ulcers, there is no universally agreed-on standard. Some of the common classifications are discussed below.
2.4.1 Meggitt-Wagner (MW) system
The Meggitt-Wagner (MW) system was initially established by Meggitt in 1976 and further adjusted and spread by Wagner in 1981. It is considered one of the most commonly used systems for the assessment of diabetic foot ulcers [1, 37, 38, 39]. It is deemed to be a practical and simple tool for utilization in clinical settings [37, 39]. It is composed of six grades, ranging from 0 to 5 based on the ulcer depth and the extent of skin necrosis (gangrene). Most patients in clinical settings have a grade of 2 or 3 [37].
However, among the limitations affecting the precision of this classification is that it does not recognize ischemia or infection in wounds of superficial depth [37]. Ischemia is only considered in grades 4 and 5 by the presence of gangrene. In addition, infection is identified only in Meggitt-Wagner grade 3. Despite the popularity of the Meggitt-Wagner classification, it has not been validated yet [37].
2.4.2 University of Texas classification (UT) system
This classification system developed more recently in the mid 1990s by the University of Texas assesses ulcer depth, in addition to ischemia and infection as opposed to the MW classification, but does not consider wound size as discussed by [37, 38]. It is also considered to be one of the most commonly used classification systems, along with the MW system [1]. The classification is composed of a 4 by 4 matrix, where wound depth is evaluated horizontally on a 4-grade scale of 0 to 3 and the ischemia and infection vertically indicating 4 stages from A to D, with stage A indicating no ischemia or infection and D, including both [39]. Some studies suggest that the UT classification system is useful for predicting amputation whereas the MW classification can only classify wound condition, while other studies suggest that both are helpful for predicting amputation, but the UT classification system can better predict the time it will take to heal [37, 38]. This is why it is one of the most widely used systems. The UT classification system is also a validated tool [37].
2.4.3 The size (area, depth), sepsis, arteriopathy, denervation [S(AD)SAD] system
The S(AD) SAD system is mainly used for clinical audit rather than in clinics as explained by [37, 39, 40]. This system evaluates five features that differentiate the lesions from each other and are given a score of 0, 1, 2, or 3 based on severity; the five features include the size (area and depth), sepsis if infected, arteriopathy if ischemic and denervation if neuropathic, with the latter two being assessed at each depth within the matrix [37, 40]. The S(AD)SAD system was validated prospectively in which four of the five clinical features correlated significantly and independently with wound healing and it has also been validated by looking at associations with outcome in internal and external settings as discussed in [37, 40].
2.4.4 The site, ischemia, neuropathy, bacterial infection, area, depth (SINBAD) system
The SINBAD system is a simple version of the S(AD)SAD classification, and it has gained validation in three separate continents for the reliable prediction of healing time [41]. It is also utilized by the UK National Diabetes Foot Care Audit [40]. It shares the same five characteristics of the S(AD)SAD system, with the additional factor of site distinguishing between the forefoot and hindfoot. The grades are calculated based on if a factor is found (1) or not (0); a maximum grade of 6 can be obtained [39, 40].
2.4.5 The perfusion (ischemia), extent (area), depth, infection, sensation (neuropathy) (PEDIS) system
The PEDIS system was first constructed by the International Working Group of Diabetic Foot (IWGDF) for utilization and classification in clinical research as stated by [37, 40, 42]. It consists of five features: perfusion (peripheral artery disease), extent (area), depth, infection, and sensation (neuropathy); the criteria are considered to be a bit complex with specific definitions and so the system is challenging to apply to all situations, as it was constructed mainly for research purposes [42].
2.4.6 The wound, ischemia, and foot infection (WIfI) system
The Society for Vascular Surgery Lower Extremity Guidelines Committee developed the wound, ischemia, and foot infection system to serve the increasing prevalence of ulcers with both neuropathy and ischemia. This system includes the three main features that are most likely to predict amputation risk at 1 year that will act as a guide to determine prognosis and select the most appropriate therapy and treatment options as discussed by [39, 42]. The components were graded on a scale of 0 to 3, including wound depth, extent of the ischemia, and if the foot is infected or not [42].
The ulcer region is appraised qualitatively. The ischemia is evaluated on the foundation of ankle brachial pressure index (ABPI), transcutaneous oxygen tension, and toe systolic pressure. Furthermore, the grading for infection was assessed via the Infectious Diseases Society of America (IDSA)/International Working Group on Diabetic Foot (IWGDF) criteria [42]. The evaluation for ischemia requires a level of aptitude and specific equipment that might not be accessible or obtainable in certain regions, countries, or institutions. However, it is important to note that the primary aim of this classification system was to be able to objectively determine the requirement for revascularization therapy [42].
2.5 Vascular and neurological assessment and imaging studies
2.5.1 Vascular assessment
The peripheral pulses including the femoral, popliteal, posterior tibial, and dorsalis pedis pulses are palpated and a comparison is made between the two sides [28]. Note the presence (+), diminished/weak (+/−), or absence (−) of peripheral pulses. Record the existence of any thrills; however, thrills give limited indication as to the location and extent of the disease [28]. The chance of having PAD is 4.9 times more likely if the peripheral pulses are absent, but PAD cannot be excluded if peripheral pulses are present [43].
Patients will usually present with diabetic retinopathy, nephropathy, or neuropathy in case the small arteries are affected. However, in other cases where larger vessels like the deep femoral artery are affected, abnormal non-invasive vascular testing evaluating blood flow, velocity, and waveforms (triphasic, biphasic, or monophasic) is suggestive of macrovascular disease [3, 43].
A Doppler assessment should be carried out and the ankle brachial index (ABI) measured [44]. To measure the ABI, the systolic blood pressure is calculated at the ankles (dorsalis pedis artery or posterior tibial artery) and at the arm (brachial systolic pressure) via a manual sphygmomanometer with the aid of a Doppler probe [28, 45]. The higher of the ankle pulses is considered and divided by the highest brachial pressure of the two arms giving the ABI, measured for both limbs. The characteristic of the Doppler signal must be noted (waveform) [28].
In addition, usage of the ABI, toe-brachial index (TBI), and absolute toe pressures is considered the most common [43, 46]. An ABI >0.9 is considered normal, <0.9 is abnormal and may indicate claudication, <0.4 is often linked with tissue death and ischemia-related pain during rest, and > 1.2 might be suggestive of calcification in the arteries in patients with diabetes [28, 45].
PAD is indicated by a low ABI and TBI of below 0.91 and 0.7, respectively [43, 46]. The TBI supports the ABI. In cases of calcinosis, the arteries become less compliant and as a result, ABI might appear to be higher than expected with regard to PAD. As such, TBI is used as a supporting measure for the diagnosis of PAD, since the distal arteries (blood vessels of the digits) are not as influenced by calcifications than those proximal [43]. Transcutaneous oxygen pressures (TcPO2) can also shed light on alterations in the microvascular circulation and the capacity for wounds to heal [3].
2.5.2 Neurological assessments
The neurological tests are used to look for loss of protective sensation in patients with diabetes mellitus, in lieu of early neuropathy detection [45]. It is usually assessed via the Semmes-Weinstein 5.07 (10 g) monofilament, paired with one of the following: vibration testing, pinprick sensation, and ankle reflexes [2].
Semmes-Weinstein 10 g monofilaments evaluate cutaneous pressure in twelve different regions on the foot [2]. The monofilament is first tested on the proximal brachial area for patient demonstration. The patient is instructed to keep their eyes closed and indicate verbally (“yes” or “no”) whether they are able to sense the monofilament’s presence and the location in which the pressure was applied. Pressure perception must not be tested on callused areas [45]. When the ability to sense the pressure in any of the 12 regions is not present, this foretells an increased risk for ulcer formation [2]. It is also advised to perform this test on four anatomical regions of both feet, including the first, third, and fifth metatarsal heads and plantar surface of the distal hallux [45]. Failure to detect the nylon monofilament sensations in more than one of the plantar foot regions is suggestive of diminished large fiber nerve function [45].
Likewise, when a patient fails in the detection of pinprick sensations, it is linked with an increased risk of ulcer formation [47]. Failure to sense the pinprick just below the dorsal surface of the big toe on either foot is not normal [45].
Usually, vibration testing is carried out with a 128-Hz tuning fork placed on the bony prominence at the same location described above. The patient is asked to verbalize the initiation and cessation of vibration [2]. Loss of vibratory sensation is when the patient can no longer feel the vibration from the tuning fork, but the examiner still can [47, 48]. A biothesiometer, on the other hand, can quantitatively assess vibratory sensation by identifying the vibration-perception threshold (VPT), which is the minimum voltage required for sensing vibration on the pulp of the hallux [2]. A VPT greater than 25 is a strong predictor of sequential ulcer formation [49, 50].
The ankle jerk reflex is assessed over the Achilles tendon. If not present at first, the ankle reflex is reevaluated with reinforcement by locking the fingers together and pulling [45]. Abnormal reflexes are diminished with or without reinforcement and are linked with a high risk of ulcer formation [45, 47].
Another quick and simple technique is the Ipswich touch test, in which the clinical examiner gently and quickly touches their index finger to the patient’s first, third, and fifth toe in either foot [2]. A patient’s sensation is considered impaired when two or more areas (out of six in the 2 feet) lack sensation [2].
2.5.3 Imaging studies
Sometimes, it is difficult to evaluate the extent of the ulceration especially in the presence of exudates and slough [51]. So, medical imaging usually involves plain x-rays to detect potential undetectable osteomyelitis, there being air in subcutaneous tissue and any foreign bodies and any indications of concealed fractures [1]. Plain x-ray can also detect loss of bone density, CNO, and ulcer depth [51, 52]. In cases of CNO, x-rays may reveal eroded bones, fractures, manifestations of bone sclerosis, fractures, and subluxations or dislocations of more than one joint, especially of the Lis Franc joint that, though common, frequently go unnoticed by experienced radiologists unless a CNO is kept in mind (Figures 1 and 2) [14, 53].
Figure 1.
Ref. [22]: Weight bearing x-ray in dorsal plantar projection. Fractures, subchondral cysts, erosions and luxation of Lisfranc’s joint (white arrows) developed 5 months post baseline (b). Baseline (a).
Figure 2.
Ref. [22]: Eichenholtz stage 1 (fragmentation) of CNO showing gross cortical fractures of the second to fifth metatarsals (white arrows) on MRI (a) and x-ray (b).
MRI is considered a favorable test especially for detecting osteomyelitis and CNO (Figures 2 and 3) [1, 51]. It is utilized for the assessment of the magnitude of ulcer infection by evaluating its depth, the presence of edema, as well as localized edema in the soft tissues, joints, and tendon sheaths [51]. In addition, positron emission tomography is highly specific for osteomyelitis [54]. Computed tomography (CT) scans and MRIs are useful for diagnosing abscesses if physical examination is inconclusive; however experienced examiners would be able to detect abscesses without radiological means [52].
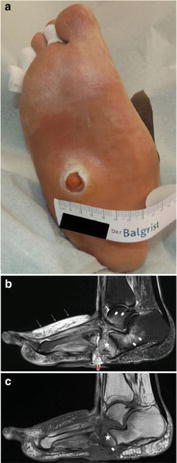
Figure 3.
Ref. [22]: (a) rocker-bottom deformity complicated by an ulcer on the plantar region of the foot, under the cuboid bone. (b) Shows spreading of infection to form a sinus tract to cuboid bone (asterisk) and bone marrow swelling as a result of active CNO (white arrows). (c) Shows osteomyelitis within the cuboid bone on a sagittal T1-weighted sequence.
Bone scans with technetium can be utilized for the diagnosis of underlying osteomyelitis, as well [1]. However, its utility is considered questionable as it often produces false negative and positive results [52].
Conventional angiography is used to evaluate the progression of vascular (atherosclerosis) disease and is important to carry out before vascular and endovascular surgery [52]. If patients are at increased risk or allergic to the injected substance, multidetector computed tomographic angiography (MRA) can be utilized instead. However, the MRA utilizes Gadolinium chelates as a contrast that can manifest three adverse events in those with renal insufficiency including pseudo hypokalemia, systemic nephrogenic fibrosis, and acute renal injury. Other options include multidetector computed tomographic angiography (MDCT), which evades arterial punctures and presents with the same adverse events as MRA. Those with renal impairment can opt for carbon dioxide angiography, but it requires iodine contrast material as well and so, is not that commonly used [52].
The management of diabetic foot ulcers is a complex and multidisciplinary process that aims to prevent complications, promote healing, and improve quality of life. Clinical evaluation includes patient and wound assessments. Patient assessment encompasses assessing the parameters that affect the prognosis of DFU, including glycemic control, CBC testing, and other comorbid conditions like renal disease and heart failure that would worsen the prognosis. This requires a thorough history and physical examination, as well as laboratory tests, imaging studies, and vascular studies.
Wound assessment begins with debridement cleaning, and applying appropriate dressings, moisturizers, and topical agents. The wound care should be tailored to the characteristics of the ulcer, such as its size, depth, exudate, and infection. The ulcer should be classified according to its depth, infection, and ischemia. Antibiotic therapy is required for nearly all infected diabetic lesions; the use of antibiotics should be deferred for wounds that are not clinically infected. It depends on the classification of wound infections to mild-moderate and severe infections. The initial antibiotic medication must usually be decided empirically; it could be adjusted subsequently based on the availability of additional clinical and microbiological results. Antibiotics may be prescribed, either orally or intravenously, depending on the type and extent of the infection. Microbial analysis is crucial to identify the specific pathogens behind the infection; it includes obtaining pus discharge sample from the wound and processing it. The infection should be monitored regularly, and the antibiotic therapy adjusted accordingly.
Offloading is necessary to reduce the pressure and friction on the ulcer, which can impair healing and worsen the wound. This can be achieved by using various devices, such as casts, braces, crutches, wheelchairs, or special shoes.
Revascularization should be considered to improve the blood supply to the ulcer and the affected limb, enhance healing, and reduce pain especially if there is evidence of peripheral artery disease or critical limb ischemia. This can be done by using medical, endovascular, or surgical interventions, depending on the severity and location of the vascular lesions.
3.1 Debridement
Debridement is a word borrowed from the French word “débrider,” which means “to unbridle, unharness.” It is the removal of non-viable or dead tissue from the site of the wound in order to promote the development of granulation tissue and re-epithelialization, two processes that aid in the healing process [38]. Eradication of the local infection will minimize the bacterial load and lower the risk of antibiotic treatment resistance. Debridement can be divided into mechanical and non-mechanical. Mechanical includes surgery, wet-to dry dressings, ultrasound debridement, biosurgery, and hydro-surgery. Non-mechanical includes enzymatic agents and autolytic debridement [55].
Mechanical debridement is relatively quicker than non-mechanical debridement; however, depending on which method is utilized, it might be selective or nonselective. It is also associated with more discomfort and pain relative to non-mechanical debridement, and more expensive. On the contrary, non-mechanical debridement tends to be more specific for non-viable tissue, simpler application with minor discomfort but it tends to be a slower process [56].
3.1.1 Surgical debridement
Surgical debridement is considered the most widely used method; it involves cutting away necrotic tissue with sharp instruments such as a scalpel or scissors [55]. It could be performed in inpatient or outpatient settings. The decision on where to carry out the debridement is determined by the patient’s level of comfort, the level of anesthetic necessary, and the extent of the debridement process required [56].
It is the most appropriate choice for removing large areas of necrotic tissue and is indicated in cases of sepsis. The surgical removal of superficial necrotic and hyperkeratotic tissue caused by repeated pressure on the foot is essential for wound healing, and it is necessary for deep wounds with bone and soft tissue involvement. Potential adverse effects from this type of treatment include bleeding from the debridement itself, and anesthesia complications [57].
Conservative surgery for DFUs in patients with chronic forefoot OM is a safe and effective approach that improves recovery and minimizes the risk of limb loss and mortality when compared to radical amputation operations. The aim of the surgeon is to avoid amputation and keep it as a last but necessary action. The indications for limb amputation are life-threatening sepsis, wet gangrene, extensive muscle necrosis, and bed-ridden patients with impossible revascularization. This decision was taken by vascular surgeons. DM-related lower limb amputation can be classified into minor and major amputations; minor involves minimal removal of tissue, typically at the level of the ankle or below including digits amputation, and partial foot amputation. Major amputation involves below and above the knee amputation and is indicated after a minor amputation if the wound is unlikely to recover, or if the necrosis has progressed to the legs [58].
3.1.2 Wet-to-dry debridement
Wet-to-dry debridement is a form of mechanical debridement that involves removing necrotic tissue from the wound. During this procedure, saline wound gauze is placed in the wound and allowed to dry completely, then it is removed from the wound bed without moistening it first, so it removes the dead tissue [59]. As saline evaporates, it becomes hypertonic, and fluid from the wound is sucked into the dressing, causing tissue desiccation [58].
This form of debridement is one of the most used dressing methods. However, in the literature, some would argue against it concluding that it does not constitute advanced wound care [58]. It increases the likelihood of external contamination compared to other debridement techniques and requires multiple dressing changes. As well as being often a painful experience for the patient, and in addition to removing dead tissue, it often removes viable tissue as well [57].
3.1.3 Ultrasound debridement
Ultrasound debridement is a technique that uses sound energy to mechanically debride wounds by contact or noncontact use of low-frequency ultrasound energy. The procedure employs a cavitation approach to generate sound energy from a handheld tool, which mechanically destroys devitalized tissue [56]. This method of debridement removes dead tissue, stimulating necrotic tissue, lessening bacterial colonies formation [60].
3.1.4 Bio-surgery (maggot-larvae)
Maggots are the larvae of the fly Lucilia sericata that are placed on necrotic wounds to consume dead and necrotic tissue. They are placed on the wound as their secretions have antibacterial features that have a bacteriostatic impact, as well as proteolytic enzymes including collagenase that break down collagen matrix [61]. It possesses features of debridement, antimicrobial, and healing stimulation. It is a selective process, which makes it advantageous.
3.1.5 Hydro-surgery
Hydro-surgery is a high-pressure process that can be performed using a syringe or a saline jet stream. It is used for disposing of foreign bodies and debris from the wound; it is a nonselective method of debridement that can remove granulation tissue and may endanger the health care practitioner. The mist produced by high-pressure watering may contaminate the provider. It does not take much time and it is suitable for large wounds [56].
The ability to integrate this technology with antiseptic remedies is an intriguing part of it. This has the potential to increase antibacterial activity, which is an important aspect of debridement operation [61].
3.1.6 Enzymatic debridement
Enzymatic debridement is applying proteolytic enzymatic substances to the wound. Many agents are used, for example, collagenase, bromelain, and papain. The most used enzyme is collagenase—sourced from strain of Clostridium histolyticum—which breaks down the collagen in the necrotic tissue to debride Clostridium bacteria. It’s advantageous since it is highly selective for collagen, and it is pain-free [62].
However, a study discussed the possibility of collagenase acting as a stimulant to keratinocyte and endothelial cell migration, increasing epithelization rather than acting as a stringent debridement agent [62]. It remains a good option in patients who require debridement but are not surgical candidates.
3.1.7 Autolytic debridement
The most conservative debridement method, phagocytic cells and proteolytic enzymes break down the necrotic tissue during this natural debridement process. Only necrotic tissue will be impacted by the debridement, making it a very selective process. It is indicated for non-infected wounds. Infected wounds may potentially benefit from its usage as an additional treatment. When treating infected wounds, it could be used with other debridement methods, such as mechanical debridement [63]. Below is a table summarizing the types of debridement mentioned in this chapter (Table 1).
Mechanical debridement
Non-mechanical debridement
Surgery
Enzymatic agents (collagenase)
Wet-to-dry (saline wound gauze)
Autolytic (proteolytic enzymes)
Ultrasound (sound energy)
Bio-surgery (maggot larvae)
Hydro-surgery (syringe/saline jet stream)
Table 1.
Types of debridement.
3.2 Infection control
The likelihood of delayed wound healing and amputation is known to increase with wound infection. To improve outcomes, it is crucial to diagnose an infection in a diabetic foot infection and treat it with antibiotics [64]. Following the proper management of debridement of necrotic tissue, infection, and ischemia, there are a variety of adjuvant treatments that may be useful to accelerate wound healing.
Antibiotics are not indicated for diabetic ulcers unless there are signs of infection. Patients with mild infections are treated with oral antibiotics that target gram-positive cocci like streptococci and Staphylococcus aureus and can be treated in outpatient settings. Effective options include medications like cephalexin, dicloxacillin, amoxicillin-clavulanate, or clindamycin [65].
Patients must be admitted for parenteral antibiotic treatment when they have moderate-to-severe infections. Gram-positive cocci, obligate anaerobes, and aggressive gram-negative aerobes should all be included in the empiric options. Vancomycin, linezolid, or daptomycin is effective against MRSA [65].
3.3 Topical antimicrobial therapy
3.3.1 Iodine-based
Cadexomer iodine (e.g., Iodosorb) is an antibacterial that promotes healing by maintaining a moist wound environment. Cadexomer iodine kills all gram-positive and gram-negative microorganisms. There is some indication that cadexomer iodine produces greater healing rates than normal treatment in topical formulations, although it should most likely only be considered for short-term use [57].
3.3.2 Silver-based
Silver dressings can be utilized as the primary or secondary dressings to treat mild, moderate, or heavy discharge in both acute and chronic wounds such as DFU, pressure ulcers, and ulcers of the legs.
The findings of a meta-analysis revealed that silver dressings improve DFU healing rate, decrease time required for full healing, reduce in-hospital length, and increase the infection clearance rate, while having no significant impact on ulcer area reduction [66].
3.3.3 Honey-based
Honey has broad-spectrum antibacterial activity due to its high osmolarity and hydrogen peroxide content. According to a meta-analysis, honey dressing effectively promoted wound healing and bacterial clearance time within the first 1 to 2 weeks of application.
According to the findings of systematic reviews evaluating honey’s ability to aid healing in a variety of wounds, there are insufficient data to make recommendations for the routine use of honey for all wound types; specific wound types, such as burns, may benefit, while others, such as chronic venous ulcers, may not [57].
3.4 Wound dressings
3.4.1 Alginate
Alginate dressings are made of natural polysaccharides derived from several types of algae. They’re available in a variety of forms, including beads, and pads. These dressings form a gel that is characteristically highly absorbent, which makes it better suited for wounds that are moderately to extensively exudative, while keeping the skin moist [64].
3.4.2 Vacuum-assisted closure
Negative pressure wound therapy (NPWT), also known as vacuum-assisted closure, is an adjuvant therapy that is utilized in the treatment of open wounds that imparts sub atmospheric pressure to the wound surface. The wound care system comprises an open-cell foam dressing, a semi occlusive adhesive cover, a fluid collection device, and a suction pump. NPWT promotes wound healing [67].
3.5 Oxygen therapy
3.5.1 Hyperbaric oxygen therapy
Hyperbaric oxygen therapy entails inhaling 100% pure oxygen in a hyperbaric chamber. Many individuals with DFUs have poor oxygenation to injured areas, especially if they have vascular disease. It promotes angiogenesis by increasing local tissue oxygen perfusion of the wound. HBOT may be particularly effective in people with diabetes who have undergone wound care for more than 4 weeks and have had a poor or no response to wound care treatment [56].
3.5.2 Topical oxygen
Topical oxygen therapy entails providing oxygen over the site of the ulcer rather than through the circulatory system as in hyperbaric oxygen therapy. Patients who are not eligible for HBOT may find this approach more appealing. The impact of topical oxygen therapy on the healing process is difficult to notably explain, but it provides an option with some marginal potential advantages and relatively minor risks [56].
This is administered by a high-flow oxygen concentrator machine and applied through a bag or container enclosed around the wound. Sustained topical oxygen therapy is administrated directly to the wound and uses pure (>99%) humidified oxygen supplied by a tiny, electrochemical oxygen generator [68].
Another way of administering topical oxygen is by applying hemoglobin containing spray to the wound. It functions by binding oxygen from the atmosphere and diffusing it into a wound to speed up the wound-healing process [69]. After adequate debridement, the spray is applied for 1–2 seconds, and the wound is covered with a dressing. In a 2018 study that observed the healing effect of various wound types, it concluded significant improvements that were detected very early following the introduction of hemoglobin spray, with statistically significant benefits identified within 1 week of the first application across wound types [70].
3.6 Offloading techniques
According to evidence-based guidelines, offloading is an essential step in aiding recovery and limiting foot ulcers and is a key aspect of DFU treatment. Mechanical offloading proves helpful for ulcers that undergo prolonged or frequent pressure and stress or recurrent mild pressure. To reduce the incidence of foot ulcers and infection, they disperse pressure on plantar surfaces, decreasing pressure on the ulcers [71]. For healing to be maintained, the offloading system must reach a threshold peak pressure of 200 KPa. The patient needs shoes for indoor and outdoor use, which the orthopedic specialist must provide [72]. Offloading devices include total contact casts, cast walkers, shoe modifications, and other devices to assist in ambulation [57].
3.6.1 Total contact cast
Total contact casting is considered the gold standard treatment for offloading DFU [71]. A total contact cast is a non-removable semi-rigid molded cast wrapped around and in contact with the foot and a portion of the leg using the TCC technique. To have complete access to the foot’s sole, the cast is frequently placed on a patient who is lying on his or her back with the knee flexed and the ankles in a neutral posture. Indications of this type of cast include plantar non-infected neuropathic ulcers of forefoot and midfoot (Meggitt-Wagner grade I and II) and early stages of Charcot arthropathy. The principle behind it is raising the weight-bearing surface area and distributing pressure over a broader region, reducing pressure. It is important to note that fracture stabilization in Charcot arthropathy -main goal rather than unloading- results in less localized tissue inflammation and swelling. The duration of the TTC is until the swelling subsides and stage III consolidation of Charcot arthropathy is achieved and until the ulcer heals.
3.6.2 Cast walkers
Cast walkers relieve pressure on the forefoot. Removable cast walkers keep the ankle at a 90-degree angle, reducing pressure on the forefoot. They can be removed by the patient, allowing for frequent ulcer inspection and dressing changes. For this reason, they can be used for infected ulcers [57].
3.6.3 Therapeutic shoes
Following ulcer healing, therapeutic shoes with orthotic insoles are recommended as a safeguard against recurrent ulcers.
A study demonstrated findings show the use of offloading therapeutic footwear minimizes the occurrence of DFU significantly. However, the positive impact may gradually subside with time [73].
Wedge shoes are a type of therapeutic footwear to offload the forefoot and heel. These shoes could be beneficial in some conditions. Plantar heel ulcers, for example, tend to be more challenging to heal due to an inability to effectively offload this area of the foot, but the heel wedge shoe may be helpful in achieving this goal. The downside of wedge shoes is that most individuals, particularly older adults, or those with proprioception disorders, may find it difficult, if not impossible, to keep their balance while wearing them [57].
3.7 Multidisciplinary approach to diabetic foot care
The MDT approach requires an integrated and shared effort among health care experts from several disciplines. According to a meta-analysis [70], lower extremity amputations (LEAs) and diabetic foot ulcerations (DFUs) have been demonstrated to decrease with the use of MDTs.
MDT includes medical professions, including Endocrinology, General Medicine, Infectious Disease, and Physical Medicine & Rehabilitation. Surgical disciplines like General Surgery, Orthopedics, Vascular, Surgery, Plastic Surgery, and Podiatry, in addition to nurses. It has been proposed that podiatrists serve as “gatekeepers” for the management and prevention of DFUs [74]. Physicians are required to assure optimal metabolic regulation and to assess long-term consequences such as infections, renal insufficiency, and nutrition. Surgeons can execute urgent debridement or limb amputation for control of infection. Vascular surgeons assess the extent of ischemia associated with wounds, develop a treatment plan, perform open or endovascular surgery, and manage peripheral arterial disease. Rehabilitation staff will screen and categorize risk, select footwear and orthotics, educate the patient, and provide psychological support.
3.8 Preventive strategies and patient education
Prevention of DFU requires lifestyle adjustment, lipid control, blood pressure management, and glucose regulation [75]. Once a year, complete foot exams should be performed on all diabetic patients. The purpose of this evaluation is to identify the risk factors that could lead to a foot ulcer and, ultimately, limb amputation. The physical examination includes vascular and neurologic assessment [75].
Patient education is crucial to avoid developing DFU and detect them early on. Some of the important recommendations for foot care include [2] avoiding activities that can cause foot injury, like walking barefoot. Both feet should be checked regularly for any deformities, blisters, or swelling and be careful while trimming the nails to prevent them from digging into the skin causing irritation. Smoking can aggravate heart and circulation issues, as well as limit blood flow to the feet, and should be stopped.
3.9 Emerging technologies
Various mobile phone applications are being developed with the aim of providing an easy means of monitoring DFU. Cassidy [76] created the first smartphone app capable of accurate DFU detection. This system was evaluated in a 6-month clinical trial at two NHS hospital sites in the UK (Lancashire Teaching Hospitals and Salford Royal Hospital) and is now being improved in terms of functionality and accuracy [58]. Additional app features include automated DFU wound pathology classification.
Medical conditions like renal diseases, and immunocompromised states as well as variables such as anemia and hyperglycemia may influence DFU development and healing. The incorporation of these parameters into machine learning algorithms should aid in the advancement of AI-based prediction models [77].
DFUs have a multifactorial etiology that most commonly includes neuropathies, vasculopathies, foot deformities, and inappropriate footwear. Patients may exhibit a variety of clinical manifestations including erythema, edema, painfulness or painlessness, loss of sensation, foot deformities, and skin changes among others. If DFUs are not managed properly, infections can arise. This is why appropriate physical examination, imaging, vascular and neurological studies completed as indicated, and classification of ulcers are important for guiding the clinician towards the best management plan for each individual patient. Management of DFU is very broad; the ones included in this chapter include debridement (mechanical and non-mechanical), infection control depending on the severity and type of wounds, topical therapy, wound dressings, oxygen therapy, and offloading techniques. To put it simply, DFU has complex etiology and diverse presentations and is optimally managed by a multidisciplinary team.
References
1.Oliver TI, Mutluoglu M. Diabetic foot ulcer. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 8 Aug 2023. pp. 2-15. PMID: 30726013
2.Wexler DJ. Evaluation of the diabetic foot. In: UptoDate. 2023
3.Del Core MA, Ahn J, Lewis RB, Raspovic KM, Lalli TA, Wukich DK. The evaluation and treatment of diabetic foot ulcers and diabetic foot infections. Foot and Ankle Orthopaedics. 2018;3(3):247301141878886. DOI: 10.1177/2473011418788864
4.Reiber GE, Vileikyte L, Boyko EJ, del Aguila M, Smith DG, Lavery LA, et al. Causal pathways for incident lower-extremity ulcers in patients with diabetes from two settings. Diabetes Care. 1999;22:157-162
5.Cheuy VA, Hastings MK, Mueller MJ. Metatarsophalangeal hyperextension movement pattern related to diabetic forefoot deformity. Physical Therapy. 2016;96:1143-1151
6.Allan J, Munro W, Figgins E. Foot deformities within the diabetic foot and their influence on biomechanics: A review of the literature. Prosthetics and Orthotics International. 2016;40:182-192
7.van Schie CH, Vermigli C, Carrington AL, Boulton A. Muscle weakness and foot deformities in diabetes: Relationship to neuropathy and foot ulceration in caucasian diabetic men. Diabetes Care. 2004;27:1668-1673
8.Liao F, An R, Pu F, Burns S, Shen S, Jan Y-K. Effect of exercise on risk factors of diabetic foot ulcers. American Journal of Physical Medicine & Rehabilitation. 2019;98(2):103-116. DOI: 10.1097/phm.0000000000001002
9.Gonzalez-Martin C, Pertega-Diaz S, Seoane-Pillado T, Balboa-Barreiro V, Soto-Gonzalez A, Veiga-Seijo R. Structural, dermal and ungual characteristics of the foot in patients with type II diabetes. Medicina. 2019;55(10):639. DOI: 10.3390/medicina55100639
10.Gnanasundaram S, Ramalingam P, Das BN, Viswanathan V. Gait changes in persons with diabetes: Early risk marker for diabetic foot ulcer. Foot and Ankle Surgery. 2020;26(2):163-168. DOI: 10.1016/j.fas.2019.01.005
11.Edmonds ME. Progress in care of the diabetic foot. The Lancet. 1999;354(9175):270-272. DOI: 10.1016/s0140-6736(99)90012-0
12.Wukich DK, Schaper NC, Gooday C, Bal A, Bem R, Chhabra A, et al. Guidelines on the diagnosis and treatment of active Charcot neuro-osteoarthropathy in persons with diabetes mellitus (IWGDF 2023). Diabetes/Metabolism Research and Reviews. 23 May 2023:e3646. DOI: 10.1002/dmrr.3646. Epub ahead of print. PMID: 37218537
13.Petrova N, Edmonds M. Acute Charcot neuro-osteoarthropathy. Diabetes/Metabolism Research and Reviews. 2016;32(S1):281-286. DOI: 10.1002/dmrr.2734
14.Rogers LC, Frykberg RG, Uccioli L, Wukich DK, Sanders L, Pitocco D, et al. The Charcot foot in diabetes. Diabetes Care. 2011;34(9):2123-2129. DOI: 10.2337/dc11-0844
15.La Fontaine J, Lavery L, Jude E. Current concepts of Charcot foot in diabetic patients. The Foot. 2016;26:7-14. DOI: 10.1016/j.foot.2015.11.001
16.Ergen FB, Sanverdi SE, Oznur A. Charcot foot in diabetes and an update on imaging. Diabetic Foot Ankle. 20 Nov 2013;4. DOI: 10.3402/dfa.v4i0.21884. PMID: 24273635; PMCID: PMC3837304
17.Frykberg RG, Zgonis T, Armstrong DG, Driver VR, Giurini JM, Kravitz SR, et al. Diabetic foot disorders: A clinical practice guideline (2006 revision). The Journal of Foot and Ankle Surgery. Sep-Oct 2006;45(5):S1-S66. DOI: 10.1016/s1067-2516(07)60001-5. PMID: 17280936
18.Chantelau E, Grützner G. Is the Eichenholtz classification still valid for the diabetic Charcot foot? Swiss Medical Weekly [Internet]. 20 Apr 2014;144(1718):w13948. DOI: 10.4414/smw.2014.13948. Available from: https://smw.ch/index.php/smw/article/view/1862 [Cited 10 Jan, 2024]
19.Dardari D. An overview of Charcot’s neuroarthropathy. Journal of Clinical and Translational Endocrinology. 2020;22:100239. DOI: 10.1016/j.jcte.2020.100239
20.Chantelau E. The perils of procrastination: Effects of early vs. delayed detection and treatment of incipient Charcot fracture. Diabetic Medicine. 2005;22(12):1707-1712. DOI: 10.1111/j.1464-5491.2005.01677.x
21.Wukich DK, Sung W, Wipf SA, Armstrong DG. The consequences of complacency: Managing the effects of unrecognized Charcot feet. Diabetic Medicine. 2011;28(2):195-198. DOI: 10.1111/j.1464-5491.2010.03141.x
22.Rosskopf AB, Loupatatzis C, Pfirrmann CWA, Böni T, Berli MC. The Charcot foot: A pictorial review. Insights into Imaging. 2019;10(1):77. DOI: 10.1186/s13244-019-0768-9
23.Palumbo PJ, Melton LJ. Peripheral vascular disease and diabetes. In: Harris MI, Hamman RF, editors. Diabetes in America. Washington DC: U.S. Govt. Printing Office; 1985. pp. 1-21 [p. XV]
24.Kullo IJ, Rooke TW. Peripheral artery disease. New England Journal of Medicine. 2016;374(9):861-871. DOI: 10.1056/nejmcp1507631
25.Tresierra-Ayala MÁ, García RA. Association between peripheral arterial disease and diabetic foot ulcers in patients with diabetes mellitus type 2. Medicina Universitaria. 2017;19(76):123-126. DOI: 10.1016/j.rmu.2017.07.002
26.National Diabetes Advisory Board. The prevention and treatment of five complications of diabetes: A guide for primary care physicians. Metabolism. 1984;33:15-17
27.Hennion DR, Siano KA. Diagnosis and treatment of peripheral arterial disease. American Family Physician. 2013;88:306-310
28.Bailey M, Griffin K, Scott D. Clinical assessment of patients with peripheral arterial disease. Seminars in Interventional Radiology. 2014;31(04):292-299. DOI: 10.1055/s-0034-1393964
29.Raspovic KM, Wukich DK. Self-reported quality of life and diabetic foot infections. The Journal of Foot and Ankle Surgery. 2014;53(6):716-719. DOI: 10.1053/j.jfas.2014.06.011
30.Bagdade JD, Root RK, Bulger RJ. Impaired leukocyte function in patients with poorly controlled diabetes. Diabetes. 1974;23(1):9-15. DOI: 10.2337/diab.23.1.9
31.Wukich DK, Hobizal KB, Raspovic KM, Rosario BL. SIRS is valid in discriminating between severe and moderate diabetic foot infections. Diabetes Care. 2013;36(11):3706-3711. DOI: 10.2337/dc13-1083
32.Grayson ML. Probing to bone in infected pedal ulcers. Journal of the American Medical Association. 1995;273(9):721. DOI: 10.1001/jama.1995.03520330051036
33.Malhotra R, Chan CS-Y, Nather A. Osteomyelitis in the diabetic foot. Diabetic Foot Ankle. 2014;5(1):24445. DOI: 10.3402/dfa.v5.24445
34.Mutluoğlu M, Uzun G, İpcioğlu OM, Sildiroglu O, Özcan Ö, Turhan V, et al. Can procalcitonin predict bone infection in people with diabetes with infected foot ulcers? A pilot study. Diabetes Research and Clinical Practice. 2011;94(1):53-56. DOI: 10.1016/j.diabres.2011.05.023
35.Lavery LA, Armstrong DG, Wunderlich RP, Mohler MJ, Wendel CS, Lipsky BA. Risk factors for foot infections in individuals with diabetes. Diabetes Care. 2006;29(6):1288-1293. DOI: 10.2337/dc05-2425
36.Bader MS. Diabetic foot infection. The Diabetic Foot. 2008;78(1):71-79
37.Karthikesalingam A, Holt PJ, Moxey P, Jones KG, Thompson MM, Hinchliffe RJ. A systematic review of scoring systems for diabetic foot ulcers. Diabetic Medicine. 2010;27(5):544-549. DOI: 10.1111/j.1464-5491.2010.02989.x
38.Santema TB, Lenselink EA, Balm R, Ubbink DT. Comparing the Meggitt-Wagner and the University of Texas wound classification systems for diabetic foot ulcers: Inter-observer analyses. International Wound Journal. 2015;13(6):1137-1141. DOI: 10.1111/iwj.12429
39.Wang X, Yuan C-X, Xu B, Yu Z. Diabetic foot ulcers: Classification, risk factors and management. World Journal of Diabetes. 2022;13(12):1049-1065. DOI: 10.4239/wjd.v13.i12.1049
40.Game F. Classification of diabetic foot ulcers. Diabetes/Metabolism Research and Reviews. 2016;32(S1):186-194. DOI: 10.1002/dmrr.2746
41.Ince P, Abbas ZG, Lutale JK, et al. Use of the SINBAD classification system and score in comparing outcome of foot ulcer management on three continents. Diabetes Care. 2008;31:964-967
42.Monteiro-Soares M, Boyko EJ, Jeffcoate W, Mills JL, Russell D, Morbach S, et al. Diabetic foot ulcer classifications: A critical review. Diabetes/Metabolism Research and Reviews. Mar 2020;36(Suppl 1):e3272. DOI: 10.1002/dmrr.3272. PMID: 32176449
43.Wukich DK, Shen W, Raspovic KM, Suder NC, Baril DT, Avgerinos E. Noninvasive arterial testing in patients with diabetes: A guide for foot and ankle surgeons. Foot & Ankle International. 2015;36(12):1391-1399. DOI: 10.1177/1071100715593888
44.Lange SF, Trampisch H-J, Pittrow D, Darius H, Mahn M, Allenberg JR, et al. Profound influence of different methods for determination of the ankle brachial index on the prevalence estimate of peripheral arterial disease. BMC Public Health. 2007;7:147. DOI: 10.1186/1471-2458-7-147. PMID: 18293542; PMCID: PMC1950873
45.Boulton AJ, Armstrong DG, Albert SF, Frykberg RG, Hellman R, Kirkman MS, et al. Comprehensive foot examination and risk assessment: A report of the task force of the foot care interest group of the American diabetes association, with endorsement by the American association of clinical endocrinologists. Diabetes Care. 2008;31(8):1679-1685. DOI: 10.2337/dc08-9021
46.Wukich DK, Raspovic KM, Suder NC. Prevalence of peripheral arterial disease in patients with diabetic Charcot neuroarthropathy. The Journal of Foot and Ankle Surgery. 2016;55(4):727-731. DOI: 10.1053/j.jfas.2016.01.051
47.Abbott CA, Carrington AL, Ashe H, Bath S, Every LC, Griffiths J, et al. The north-west diabetes foot care study: Incidence of, and risk factors for, new diabetic foot ulceration in a community-based patient cohort. Diabetic Medicine. 2002;19(5):377-384. DOI: 10.1046/j.1464-5491.2002.00698.x
48.Singh N. Preventing foot ulcers in patients with diabetes. Journal of the American Medical Association. 2005;293(2):217. DOI: 10.1001/jama.293.2.217
49.Young MJ, Breddy JL, Veves A, Boulton AJ. The prediction of diabetic neuropathic foot ulceration using vibration perception thresholds: A prospective study. Diabetes Care. 1994;17(6):557-560. DOI: 10.2337/diacare.17.6.557
50.Armstrong DG, Lavery LA, Vela SA, Quebedeaux TL, Fleischli JG. Choosing a practical screening instrument to identify patients at risk for diabetic foot ulceration. Archives of Internal Medicine. 1998;158(3):289. DOI: 10.1001/archinte.158.3.289
51.Singh S, Pai DR, Yuhhui C. Diabetic foot ulcer – Diagnosis and management. Clinical Research on Foot and Ankle. 2013;01(03). DOI: 10.4172/2329-910x.1000120
52.Rosyid FN. Etiology, pathophysiology, diagnosis and management of diabetics’ foot ulcer. International Journal of Research in Medical Sciences. 2017;5(10):4206. DOI: 10.18203/2320-6012.ijrms20174548
53.Konarzewska A, Korzon-Burakowska A, Rzepecka-Wejs L, Sudoł-Szopińska I, Szurowska E, Studniarek M. Diabetic foot syndrome: Charcot arthropathy or osteomyelitis? Part I: Clinical picture and radiography. Journal of Ultrasonography. 2018;18(72):42-49. DOI: 10.15557/JoU.2018.0007
54.Madan SS, Pai DR. Charcot neuroarthropathy of the foot and ankle. Orthopaedic Surgery. 2013;5(2):86-93. DOI: 10.1111/os.12032
55.Armstrong DG, de Asla RJ. Management of Diabetic Foot Ulcers. In: Connor RF, editor. UpToDate. Wolters Kluwer; 2022
56.Dayya D, O’Neill OJ, Huedo-Medina TB, Habib N, Moore J, Iyer K. Debridement of diabetic foot ulcers. Advances in Wound Care. 2022;11(12):666-686. DOI: 10.1089/wound.2021.0016
57.Armstrong DG, Meyr AJ. Basic principles of wound management. In: Connor RF, editor. UpToDate. Wolters Kluwer; 2022
58.Liao X, Li S-H, El Akkawi MM, Fu X, Liu H, Huang Y. Surgical amputation for patients with diabetic foot ulcers: A Chinese expert panel consensus treatment guide. Frontiers in Surgery. 8 Nov 2022;9:1003339. DOI: 10.3389/fsurg.2022.1003339. PMID: 36425891; PMCID: PMC9679004
59.Fleck CA. Why “Wet to Dry”? The Journal of the American College of Clinical Wound Specialists. 6 Oct 2009;1(4):109-113. DOI: 10.1016/j.jcws.2009.09.003. PMID: 24527129; PMCID: PMC3601877
60.Campitiello F, Mancone M, Corte AD, Guerniero R, Canonico S. An evaluation of an ultrasonic debridement system in patients with diabetic foot ulcers: A case series. Journal of Wound Care. 2018;27(4):222-228. DOI: 10.12968/jowc.2018.27.4.222
61.Strohal R, Dissemond J, Jordan O’Brien J, Piaggesi A, Rimdeika R, Young T, et al. EWMA document: Debridement: An updated overview and clarification of the principle role of debridement. Journal of Wound Care. Jan 2013;22(1):5. DOI: 10.12968/jowc.2013.22.sup1.s1. PMID: 23299351
62.Demidova-Rice TN, Geevarghese A, Herman IM. Bioactive peptides derived from vascular endothelial cell extracellular matrices promote microvascular morphogenesis and wound healing in vitro. Wound Repair and Regeneration. 2010;19(1):59-70. DOI: 10.1111/j.1524-475x.2010.00642.x
63.Manna B, Nahirniak P, Morrison CA. Wound Debridement. In: StatPearls. Treasure Island (FL): StatPearls Publishing; Jan 2024. [Updated 2023 Apr 19]
64.Everett E, Mathioudakis N. Update on Management of Diabetic Foot Ulcers. Annals of the New York Academy of Sciences; Jan 2018:1411(1):153
65.Noor S, Khan RU, Ahmad J. Understanding diabetic foot infection and its management. Diabetology and Metabolic Syndrome. Apr-Jun 2017;11(2):149-156. DOI: 10.1016/j.dsx.2016.06.023. Epub 2016 Jun 18. PMID: 27377687
66.Luo Y, Li L, Zhao P, Yang C, Zhang J. Effectiveness of silver dressings in the treatment of diabetic foot ulcers: A systematic review and meta-analysis. Journal of Wound Care. 2022;31(11):979-986. DOI: 10.12968/jowc.2022.31.11.979
68.Oropallo A, Andersen CA. Topical oxygen. In: Statpearls [Internet]. Treasure Island (FL): StatPearls Publishing; Jan 2024
69.Hunt SD, Elg F. Clinical effectiveness of hemoglobin spray (granulox®) as adjunctive therapy in the treatment of chronic diabetic foot ulcers. Diabetic Foot and Ankle. 2016;7(1):33101. DOI: 10.3402/dfa.v7.33101
70.Elg F, Hunt S. Hemoglobin spray as adjunct therapy in complex wounds: Meta-analysis versus standard care alone in pooled data by wound type across three retrospective cohort controlled evaluations. SAGE Open Medicine. 2018;6:205031211878431. DOI: 10.1177/2050312118784313
71.Majid U, Argáez C. Off-Loading Devices for People with Diabetic Neuropathic Foot Ulcers: A Rapid Qualitative Review. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 17 Jun 2020. PMID: 33296155
72.Apelqvist J. Diagnostics and treatment of the diabetic foot. Endocrine. 2012;41(3):384-397. DOI: 10.1007/s12020-012-9619-x
73.Luo B, Cai Y, Chen D, Wang C, Huang H, Chen L, et al. Effects of special therapeutic footwear on the prevention of diabetic foot ulcers: A systematic review and meta-analysis of randomized controlled trials. Journal of Diabetes Research. 2022;2022:1-10. DOI: 10.1155/2022/9742665
74.Musuuza J, Sutherland BL, Kurter S, Balasubramanian P, Bartels CM, Brennan MB. A systematic review of multidisciplinary teams to reduce major amputations for patients with diabetic foot ulcers. Journal of Vascular Surgery. Apr 2020;71(4):1433-1446.e3. DOI: 10.1016/j.jvs.2019.08.244. Epub 2019 Oct 30. PMID: 31676181; PMCID: PMC7096268
75.Iraj B, Khorvash F, Ebneshahidi A, Askari G. Prevention of Diabetic Foot Ulcer. International Journal of Preventive Medicine; Mar 2013;4(3):373-376. PMID: 23626896; PMCID: PMC3634178
76.Cassidy B, Reeves ND, Pappachan JM, Ahmad N, Haycocks S, Gillespie D, et al. A cloud-based deep learning framework for remote detection of diabetic foot ulcers. IEEE Pervasive Computing. 2022;21(2):78-86. DOI: 10.1109/mprv.2021.3135686
77.Pappachan JM, Cassidy B, Fernandez CJ, Chandrabalan V, Yap MH. The role of artificial intelligence technology in the care of diabetic foot ulcers: the past, the present, and the future. World Journal of Diabetes. 15 Dec 2022;13(12):1131-1139. DOI: 10.4239/wjd.v13.i12.1131. PMID: 36578875; PMCID: PMC9791570
Written By
Reem Al-Subai, Reema M. Al-Emadi, Hesham Aljohary and Musab Murad
Submitted: 01 October 2023Reviewed: 18 October 2023Published: 11 March 2024