
Abstract
With the escalating economic burden of tumors, there is an urgent imperative to develop novel therapies. Activation of complement to eliminate tumors proves to be an effective approach. ABO blood group antibodies, naturally present in the body, activate the immune system by recognizing blood group antigens, resulting in the lysis and demise of red blood cells. Similarly, ABO blood group antigens can activate the human immune response and exhibit anti-tumor effects. By leveraging the immune properties of blood group antibodies in tumor treatment, a mechanism akin to the destruction of red blood cells in blood group incompatibility can be employed to eradicate tumor cells. This approach holds promise as a fresh avenue for tumor treatment and prevention of resistance.
Keywords
- blood group antigen
- solid tumors
- antigen therapy
- cancer treatment
- cancer immunotherapy
1. Introduction
Due to the potential for deadly blood type compatibility problems during transfusions, ABO blood group antigens are both highly immunogenic and essential in transfusion therapy. ABO blood types vary across groups, which raises the possibility that they play a role in providing selecting benefits such as immunity to infectious illnesses [1]. Other blood cells pick up these antigens from the plasma, while red blood cells have roughly 2 million of them per cell. They may also be present in plasma proteins, some organs, platelets, white blood cells, and a variety of cell surface enzymes [2, 3, 4]. Except for cerebrospinal fluid, soluble ABO blood type antigens are present in secretors’ body fluids. Paraphrased: A, B, and O are the three primary variations of the ABO locus. The A and B antigens are created, respectively, by the glycosyltransferases that the A and B alleles generate. Specific single nucleotide polymorphisms (SNPs) in the ABO gene, which result in variants in the A and B transferases, are the cause of the A/B variances. The H antigen, the precursor to the ABO antigen, is unchanged by the O allele, which results in an inactive glycosyltransferase [1].
In 1953, the first evidence between the ABO blood group system and cancer was discovered. Their results point to a relationship between the ABO blood types and the prevalence of stomach cancer, suggesting that blood group A may have a negative impact on the chance of developing stomach cancer, whereas blood group 0 may have a positive impact [5]. Additionally, it has been shown that both primary breast cancers and their metastases show a decrease in blood group antigen expression, which may act as a possible invasion marker [6, 7]. In addition, colorectal cancer is significantly influenced by the ABO blood type antigens, with 50% of proximal colon cancers exhibiting a decrease in antigen expression. Incompatible expression of BG-A or B seems to be exclusive to cancer tissue, and these antigenic changes are seen in premalignant polyps, suggesting their participation in the early phases of neoplastic evolution [8]. The strongest link among all cancer types is the one between blood group A and an increased risk of stomach cancer. The finding that people with blood type A are more likely to get the recognized stomach cancer-causing pathogen
An innovative method for treating cancer is immunotherapy [10]. ABO blood type antigens have the ability to trigger the human immune system during solid tumor treatment and provide anti-tumor effects. By making use of this process, we suggest a novel approach to the treatment of malignancies and the prevention of resistance by causing erythrocyte-like lysis to destroy tumor cells and decrease tumor growth by activating the immune system with blood type antigens. This study illuminates intriguing prospects for enhanced tumor treatment.
2. ABO blood group antigens in cancer
The ABO gene, located on chromosome 9q34, encodes two glycosyltransferases, A and B, which link N-acetylgalactosamine or d-galactose to a shared precursor side chain (H determinant), resulting in the formation of the A or B antigens [11, 12]. The O variation of the gene produces a glycosyltransferase that lacks functionality, resulting in minor changes to the H antigen, in contrast to the A and B alleles. [12].
The phrase “histoblood group ABO” is used because ABO antigens are present in a large number of people. Growing evidence from recent scientific literature suggests that the clinical importance of the ABO system extends beyond immunohematology, transfusion, and transplantation medicine, as it plays a critical role in the emergence of cardiovascular, infectious, and neoplastic diseases as well as a number of other human disorders [13, 14, 15, 16, 17]. More specifically, some investigations have shown a relationship between ABO blood group antigens and various cancer types [18, 19].
There is ongoing investigation into the precise mechanisms by which the ABO blood type or closely related genetic changes in the ABO locus affect cancer development and progression [16]. The enzymatic activity of ABO glycosyltransferases, which are essential for intercellular adhesion, cellular membrane communication, and the host’s immunological response, may be disturbed during this contact, according to one reasonable theory [20, 21]. Following a mechanism similar to the well-known role of ABO glycosyltransferases in regulating circulating plasma levels of von Willebrand factor, which ultimately results in an increased risk of venous thromboembolism [22, 23]. The modification of these surface molecules may potentially promote the development of cancer. This fascinating correlation is made even more convincing by recent research that indicates the von Willebrand factor plays a critical role in controlling angiogenesis and apoptosis, two procedures that are strongly related to carcinogenesis [24].
By altering the inflammatory state of the host, ABO type antigens may have an impact on the development and spread of cancer [25]. For instance, alterations in the ABO gene locus have been linked to the amounts of circulating molecules such as tumor necrosis factor-alpha [26], soluble intercellular adhesion molecule (ICAM)-1 [27, 28], E-selectin [29, 30], and P-selectin25. Because they directly link the ABO blood group with tumor start and spread, these results provide a biological justification for the hypothesized effect of ABO blood type on cancer prognosis [16]. The expression of soluble ICAM-1 is noticeably reduced in non-O blood group individuals, notably in blood group A individuals. By binding to ICAM ligands on circulating cells, this protein inhibits lymphocyte attachment to endothelial cells, suggesting a possible relationship between the ABO blood type and the degree of soluble ICAM-1 expression [31, 32]. The lower amounts of soluble ICAM in non-O blood group individuals may make it easier for malignancies to move to other areas of the body since certain cancer cells use similar adhesion processes to connect to endothelial cells and encourage metastasis [33].
A link between the illness and a locus on 9q34, denoted by the SNP rs505922, was found by a two-stage genome-wide association research on pancreatic cancer. It is remarkable that this SNP matches the ABO blood group gene’s first intron. According to past epidemiological research showing a decreased risk for those with blood group O compared to groups A or B, the results are consistent with the notion that the ABO blood group antigen may contribute to pancreatic cancer risk. This finding offers insightful information on the possible role of ABO antigen in pancreatic cancer and its implications for future study and therapy plans [34]. Later, the research was repeated by Rizzato and colleagues [35]. Based on research with 417 participants, Dandona and colleagues confirmed that individuals with blood types other than O had a higher chance of developing pancreatic cancer [36].
Various normal and malignant tissues, including renal cell carcinoma lines and kidneys, may be shown to have ABO antigens on their surfaces [37]. The lack of lymph node metastases and the occurrence of bilateral renal cell carcinoma (RCC) were both related to the ABO blood type, especially blood group O [38].
Blood type A or AB had a higher risk of developing nasopharyngeal carcinoma (NPC) than blood type O, according to research by Sheng et al. raising the possibility that the incidence of NPC and ABO blood types are related [39]. Blood type O was linked to a smaller percentage of poorly differentiated SCC, according to another research by Nozoe et al., but blood group AB was linked to greater tumor sizes and more advanced TNM stages. More malignancies with venous invasion were found to be associated with blood type A [40].
Large population-based studies have consistently shown a greater incidence of stomach cancer in those with blood type A. ABO blood type antigens have been linked to both stomach cancer and peptic ulcers, according to research by Edgren et al. Blood type A is connected to a greater risk of stomach cancer, while blood type O is linked to a higher risk of peptic ulcers. These relationships were verified by the research using a large population-based cohort [41]. In addition, individuals with blood types A, B, and all non-O blood groups together are at an increased risk of getting gastric cancer [42].
Based on a meta-analysis of 14 studies with 9665 breast cancer patients and 244,768 controls, it was hypothesized that blood type A Caucasians may be at higher risk of breast cancer than those with other blood types [43]. Patients with blood types B and AB had a significantly increased breast cancer incidence [44]. According to Mao et al.’s research, blood groups A and AB had a higher risk of developing gastric cancer than blood type O in a Chinese cohort and in a meta-analysis of other studies [45].
3. Anti-tumor mechanism
There are two routes through which immune-mediated processes might destroy red blood cells: immune cells use antibody-dependent cell-mediated cytotoxicity (ADCC) and complement lysis, which are often produced by antibodies [46, 47]. Specialized Natural Killer (NK) cells that can recognize complement and IgG/IgM molecules bound to red blood cells are the main drivers of ADCC. In ADCC mediated by antibodies, NK cells non-specifically destroy any target cells that have attached to the antibody, whereas antibodies precisely bind to particular epitopes on target cells [47]. In certain immunological or nonimmune hemolytic anemia instances [48], complement activation may play a role in the destruction of red blood cells, as is the case in systemic lupus erythematosus, when complement levels rise markedly [49]. Three main processes are involved in the destruction of tumor cells coated with IgG antibodies: receptor-mediated cytotoxicity, antibody-dependent cell-mediated cytotoxicity, and complement-mediated cytotoxicity, which happens when complement is triggered by clustered Fc regions resembling antibodies. The lysis of red blood cells is comparable to this mechanism [50]. As a result, the complement has become a very useful tool for eliminating tumor cells.
Perforin, granzyme, and other cytotoxic chemicals are released by activated NK cells, which successfully eliminate target tumor cells [51]. A growing body of research suggests that NK cells may directly kill tumor cells without the need for pre-sensitization and can boost adaptive immunity’s anti-tumor response by releasing cytokines [52]. The increase of tumor cell A antigen significantly increased the number of NK cells in tumor tissues, giving strong support for the pivotal anti-tumor function of NK cells [53].
Immunoediting, in which tumor cells are modified to become less immunogenic and avoid immune system detection, is the main method used to confer drug resistance on tumor cells [54]. Solid tumors may be induced to produce blood type antigens by local injection of lentiviral vectors, successfully reversing the problem of immunogenicity loss brought on by tumor immunoediting. With this method, immunological responses are specifically triggered.
In their study, Luo et al. used lentiviral vectors containing ABO blood type antigens to effectively limit the development of tumors in breast and colon cancer by inducing an immunological response in the body [53].
4. Challenges in solid tumor therapy
Solid tumor treatment has various obstacles in research and development. ABO blood type antigen treatment has shown promise in preclinical research. There are several barriers to overcome before this treatment may be extensively employed in clinical settings. Understand solid tumor therapy’s obstacles and limits to advance the field and improve patient outcomes.
The role of ABH blood groups in solid tumors is complex and varies depending on the type of carcinoma. In most types of carcinomas, the loss of A and B antigens is observed, with the H antigen being the only truly lost in pancreatic carcinomas. However, there are exceptions to this pattern in colorectal, hepatocarcinomas, and thyroid carcinomas, where ABH antigens are strongly expressed. The re-expression of A and B antigens is an early event in colorectal carcinogenesis but is lower in metastases. Anomaly in A and B antigenic expression, such as polyfucosylated structures, have been observed in various carcinoma types. The Lewis family of antigens, including sialyl-Lea, sialyl-Leb, and Ley antigens, also play a role in cancer, with their expression increasing or decreasing depending on the type of carcinoma. The molecular mechanisms responsible for the loss or re-expression of A and B antigens in tumors are still not fully understood [55]. ABH and Lewis blood types have the potential to treat solid cancers as disease indicators, allowing for early diagnosis and prognosis of various types of cancer. Serum indicators like sialyl-Lea and Leb have shown promise in colorectal, ovarian, and pancreatic cancers. However, their genetic variability limits their function as disease indicators. Monoclonal antibodies targeting cancer cells can slow or reverse tumor development, while bispecific antibodies recognizing both CD3 lymphocyte antigens and tumor antigens like sialyl-Lea activate T lymphocytes and direct their cytotoxicity to tumor cells. To halt metastatic spread, soluble sialyl-Lewis derivatives or selectin ligand mimetic peptides may inhibit selectin function. Therapeutic vaccinations targeting specific ABH and Lewis antigens, such as oligosaccharides and immunogenic proteins, have been used to immunize patients with high globo H and Ley antibody titers. The therapeutic value of these methods is being assessed [56, 57].
According to some recent research, the efficiency of ABO blood type antigen treatment for cancer has been examined by turning on the killer cells of the complement system with the use of ABO blood type antibodies. Breast and colorectal cancer cells were injected into mice models with blood group A antibodies in various preclinical studies. Intratumor lentivirus injections with blood type antigens significantly reduced tumor volume in mice. After treatment, the tumors contain more NK cells and the C5b-9 complement membrane attack complex. Studies conducted in vitro showed that serum containing blood group A antibodies inhibited the development of tumor cells. These findings suggest that ABO blood type antigen therapy might be used to treat tumors. The article examines the impact of blood group A antibodies on the development of tumor cells as well as the blood group A antigen’s therapeutic potential in the management of cancers. According to studies done on mice, serum containing an anti-blood group A antibody dramatically slowed the development of tumors and decreased the number of cancer cells in both colon and breast cancer. Additionally, it was shown that the tumor volume and weight in mice were dramatically reduced by the lentiviral vector containing the blood type A antigen. As shown by an increase in the number of tumor cells attacked by the complement complex and an increase in the percentage of Natural Killer Cells (NK cells) in tumor tissue, the complement system was also shown to have a role in suppressing tumor development by the blood group antigen. [53].
One paper covers the difficulties and restrictions of ABO blood type antigen treatment for solid tumors. Researchers describe their experiences treating patients with relapsed or resistant acute myeloid leukemia (AML) using the humanized anti-CD47 monoclonal antibody Hu5F9-G4. It was discovered that Hu5F9-G4 therapy caused hemoglobin levels to drop and transfusion needs to rise. RBC agglutination, issues with ABO blood type, and compatibility tests were also noted. These results imply that facilities caring for Hu5F9-G4 patients should be aware of these possible problems [58].
5. Mechanisms and strategies for ABO blood group antigen therapy
The World Health Organization states that surgery, radiation therapy, and chemotherapy are the major cancer therapies, but cure rates are poor. New therapies are needed to treat a large proportion of untreated individuals. Immunotherapy, particularly CART, has made significant strides but has off-target consequences. The immune system targets and decreases tumor cells by reducing surface antigens. ABO blood type antigens are present in red blood cells, platelets, white blood cells, plasma proteins, tissues, and cell surface enzymes. The strongest relationship between blood type A and stomach cancer is any malignancy. The discovery that A blood type individuals are more sensitive to
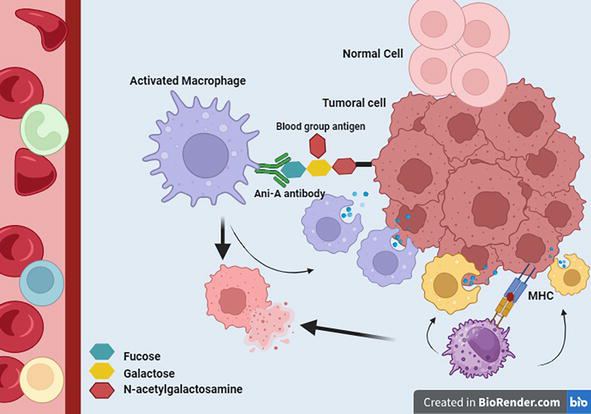
Figure 1.
Depicts the significance of ABO blood group antigens as potential therapeutic targets in solid tumor treatment. Notably, the expression of ABO blood group antigens on the surface of tumoral cells becomes a focal point for targeted antibody interventions.
Despite multiple research linking ABO phenotype to cancer risk, the mechanism of action and the relationship between histoblood group antigen expression and carcinogenesis were unknown for most tumor types. ABO blood type antibodies naturally stimulate the immune system by detecting blood group antigens to lyse and kill red blood cells. Similarly, ABO blood type antigens may boost immunity and fight cancer. The immunological impact of blood group antibodies may eliminate tumor cells in a manner similar to that of red blood cells after blood group incompatibility. Based on these discoveries, blood type antigens may be expressed on human tumor cell membranes. Blood group antigens attach to human serum antibodies to trigger the immune system to produce erythrocyte-like lysis to kill tumor cells and shrink the tumor. Patients with blood type A pick blood group B antigens, whereas those with type B choose A. To get mice to develop antibodies for the A blood group, the researchers employed vaccination techniques. To produce the A blood group antigen on tumor cells, they put the necessary genes into a lentiviral expression vector. The findings demonstrated that both colorectal and breast cancer cell numbers were decreased, and tumor development was suppressed in the presence of the A blood type antigen. The therapeutic result was independent of the mice’s immunological history. The complement system and natural killer cells were also discovered to be involved in the study’s findings that tumor development was slowed. Overall, the research showed that ABO blood type antigen therapy may be used to treat tumors. This study indicates that solid tumors expressing ABO blood type antigens may be treated in a novel way [53, 61].
The work uses lentiviral vectors to transmit ABO blood group antigen genes in breast and colon cancer cells. Antigen expression causes an immune response that prevents tumor progression. The paper also examines lentiviral vectors’ efficiency in delivering solid tumor therapy genes. The researchers created a mouse model with blood type A antibodies and discovered that blood group antigens reduced cancer cell growth. The research reveals that this technique works better for colorectal cancer than breast cancer, probably owing to tissue-specific gene expression. Complement lysis and antibody-dependent cell-mediated cytotoxicity kill tumor cells. The research also shows how NK cells and complement may destroy tumor cells. The use of blood type antigens to induce immune responses may help overcome tumor immunoediting and treatment resistance. The study suggests improving intratumoral injection efficiency, treating AB blood group patients, combining this approach with other immune factors, studying the effect on other solid tumors, and comparing IgM and IgG antibodies in treatment efficacy. The study shows that blood type antigens heal tumors and urges additional investigation [51, 62, 63, 64].
6. Conclusion
In conclusion, the relationship between ABO blood type, cancer development, and immune-mediated processes holds remarkable potential for advancing cancer treatment. Disruptions in ABO glycosyltransferase activity and the intriguing connection to the von Willebrand factor suggest intricate mechanisms at play. Moreover, the parallels between immune-mediated destruction of red blood cells and tumor cells highlight the intricate nature of the immune response. While ABO blood type antigen treatment shows promise, navigating the challenges of solid tumor therapy is essential for translating research into clinical success. Understanding these complexities is crucial for pushing the boundaries of cancer treatment and improving patient outcomes.
Acknowledgments
The authors would like to express their gratitude to Professor Anil Tombak for their invaluable guidance and supervision throughout the process of writing this chapter. This chapter was not supported by any grant.
References
- 1.
Dean L. Blood Groups and Red Cell Antigens [Internet]. Bethesda, MD: National Center for Biotechnology Information (US); Chapter 5, The ABO blood group. 2005. Available from: https://www.ncbi.nlm.nih.gov/books/NBK2267/ - 2.
Ewald DR, Sumner SC. Blood type biochemistry and human disease. Wiley Interdisciplinary Reviews. Systems Biology and Medicine. 2016; 8 (6):517-535 - 3.
Zhang D, Tan M, Zhong W, Xia M, Huang P, Jiang X. Human intestinal organoids express histo-blood group antigens, bind norovirus VLPs, and support limited norovirus replication. Scientific Reports. 2017; 7 (1):12621 - 4.
Dotz V, Wuhrer M. Histo-blood group glycans in the context of personalized medicine. Biochimica et Biophysica Acta. 2016; 1860 (8):1596-1607 - 5.
Aird I, Bentall HH, Roberts JA. A relationship between cancer of stomach and the ABO blood groups. British Medical Journal. 1953; 1 (4814):799-801 - 6.
Idikio HA, Manickavel V. A, B, H, and Lewis-a and Lewis-b blood group antigens in human breast cancer: Correlation with steroid hormone receptor and disease status. Journal of Cancer Research and Clinical Oncology. 1993; 119 (8):486-492 - 7.
Lee AK, Rosen PP, DeLellis RA, Saigo PE, Gangi MD, Groshen S, et al. Tumor marker expression in breast carcinomas and relationship to prognosis. An immunohistochemical study. American Journal of Clinical Pathology. 1985; 84 (6):687-696 - 8.
Itzkowitz SH, Yuan M, Ferrell LD, Palekar A, Kim YS. Cancer-associated alterations of blood group antigen expression in human colorectal polyps. Cancer Research. 1986; 46 (11):5976-5984 - 9.
Wang Z, Liu L, Ji J, Zhang J, Yan M, Zhang J, et al. ABO blood group system and gastric cancer: A case-control study and meta-analysis. International Journal of Molecular Sciences. 2012; 13 (10):13308-13321 - 10.
Ribas A, Wolchok JD. Cancer immunotherapy using checkpoint blockade. Science. 2018; 359 (6382):1350-1355 - 11.
Yamamoto F, Clausen H, White T, Marken J, Hakomori S. Molecular genetic basis of the histo-blood group ABO system. Nature. 1990; 345 (6272):229-233 - 12.
Lowe JB. The blood group-specific human glycosyltransferases. Baillière's Clinical Haematology. 1993; 6 (2):465-492 - 13.
Anstee DJ. The relationship between blood groups and disease. Blood. 2010; 115 (23):4635-4643 - 14.
Liumbruno GM, Franchini M. Beyond immunohaematology: The role of the ABO blood group in human diseases. Blood Transfusion. 2013; 11 (4):491-499 - 15.
Franchini M, Mannucci PM. ABO blood group and thrombotic vascular disease. Thrombosis and Haemostasis. 2014; 112 (6):1103-1109 - 16.
Franchini M, Favaloro EJ, Targher G, Lippi G. ABO blood group, hypercoagulability, and cardiovascular and cancer risk. Critical Reviews in Clinical Laboratory Sciences. 2012; 49 (4):137-149 - 17.
Dentali F, Sironi AP, Ageno W, Turato S, Bonfanti C, Frattini F, et al. Non-O blood type is the commonest genetic risk factor for VTE: Results from a meta-analysis of the literature. Seminars in Thrombosis and Hemostasis. 2012; 38 (5):535-548 - 18.
Liumbruno GM, Franchini M. Hemostasis, cancer, and ABO blood group: The most recent evidence of association. Journal of Thrombosis and Thrombolysis. 2014; 38 (2):160-166 - 19.
Franchini M, Lippi G. The intriguing relationship between the ABO blood group, cardiovascular disease, and cancer. BMC Medicine. 2015; 13 :7 - 20.
Zhang S, Zhang HS, Cordon- Cardo C, Reuter VE, Singhal AK, Lloyd KO, et al. Selection of tumor antigens as targets for immune attack using immunohistochemistry: II. Blood group-related antigens. International Journal of Cancer. 1997; 73 (1):50-56 - 21.
Hakomori S. Tumor-associated carbohydrate antigens defining tumor malignancy: Basis for development of anti-cancer vaccines. Advances in Experimental Medicine and Biology. 2001; 491 :369-402 - 22.
Jenkins PV, O'Donnell JS. ABO blood group determines plasma von Willebrand factor levels: A biologic function after all? Transfusion. 2006; 46 (10):1836-1844 - 23.
Franchini M, Crestani S, Frattini F, Sissa C, Bonfanti C. ABO blood group and von Willebrand factor: Biological implications. Clinical Chemistry and Laboratory Medicine. 2014; 52 (9):1273-1276 - 24.
Franchini M, Frattini F, Crestani S, Bonfanti C, Lippi G. von Willebrand factor and cancer: A renewed interest. Thrombosis Research. 2013; 131 (4):290-292 - 25.
Grivennikov SI, Greten FR, Karin M. Immunity, inflammation, and cancer. Cell. 2010; 140 (6):883-899 - 26.
Melzer D, Perry JR, Hernandez D, Corsi AM, Stevens K, Rafferty I, et al. A genome-wide association study identifies protein quantitative trait loci (pQTLs). PLoS Genetics. 2008; 4 (5):e1000072 - 27.
Paré G, Chasman DI, Kellogg M, Zee RY, Rifai N, Badola S, et al. Novel association of ABO histo-blood group antigen with soluble ICAM-1: Results of a genome-wide association study of 6,578 women. PLoS Genetics. 2008; 4 (7):e1000118 - 28.
Barbalic M, Dupuis J, Dehghan A, Bis JC, Hoogeveen RC, Schnabel RB, et al. Large-scale genomic studies reveal central role of ABO in sP-selectin and sICAM-1 levels. Human Molecular Genetics. 2010; 19 (9):1863-1872 - 29.
Paterson AD, Lopes-Virella MF, Waggott D, Boright AP, Hosseini SM, Carter RE, et al. Genome-wide association identifies the ABO blood group as a major locus associated with serum levels of soluble E-selectin. Arteriosclerosis, Thrombosis, and Vascular Biology. 2009; 29 (11):1958-1967 - 30.
Qi L, Cornelis MC, Kraft P, Jensen M, van Dam RM, Sun Q , et al. Genetic variants in ABO blood group region, plasma soluble E-selectin levels and risk of type 2 diabetes. Human Molecular Genetics. 2010; 19 (9):1856-1862 - 31.
Witkowska AM, Borawska MH. Soluble intercellular adhesion molecule-1 (sICAM-1): An overview. European Cytokine Network. 2004; 15 (2):91-98 - 32.
Rieckmann P, Michel U, Albrecht M, Brück W, Wöckel L, Felgenhauer K. Soluble forms of intercellular adhesion molecule-1 (ICAM-1) block lymphocyte attachment to cerebral endothelial cells. Journal of Neuroimmunology. 1995; 60 (1-2):9-15 - 33.
Kobayashi H, Boelte KC, Lin PC. Endothelial cell adhesion molecules and cancer progression. Current Medicinal Chemistry. 2007; 14 (4):377-386 - 34.
Amundadottir L, Kraft P, Stolzenberg-Solomon RZ, Fuchs CS, Petersen GM, Arslan AA, et al. Genome-wide association study identifies variants in the ABO locus associated with susceptibility to pancreatic cancer. Nature Genetics. 2009; 41 (9):986-990 - 35.
Rizzato C, Campa D, Giese N, Werner J, Rachakonda PS, Kumar R, et al. Pancreatic cancer susceptibility loci and their role in survival. PLoS One. 2011; 6 (11):e27921 - 36.
Dandona M, Gao F, Linehan DC, Wang-Gillam A. Re: ABO blood group and the risk of pancreatic cancer. Journal of the National Cancer Institute. 2010; 102 (2):135-137; author reply 7 - 37.
Breimer ME, Mölne J, Nordén G, Rydberg L, Thiel G, Svalander CT. Blood group a and B antigen expression in human kidneys correlated to A1/A2/B, Lewis, and secretor status. Transplantation. 2006; 82 (4):479-485 - 38.
de Martino M, Waldert M, Haitel A, Schatzl G, Shariat SF, Klatte T. Evaluation of ABO blood group as a prognostic marker in renal cell carcinoma (RCC). BJU International. 2014; 113 (5b):E62-E66 - 39.
Sheng L, Sun X, Zhang L, Su D. ABO blood group and nasopharyngeal carcinoma risk in a population of Southeast China. International Journal of Cancer. 2013; 133 (4):893-897 - 40.
Nozoe T, Ezaki T, Baba H, Kakeji Y, Maehara Y. Correlation of ABO blood group with clinicopathologic characteristics of patients with esophageal squamous cell carcinoma. Diseases of the Esophagus. 2004; 17 (2):146-149 - 41.
Edgren G, Hjalgrim H, Rostgaard K, Norda R, Wikman A, Melbye M, et al. Risk of gastric cancer and peptic ulcers in relation to ABO blood type: A cohort study. American Journal of Epidemiology. 2010; 172 (11):1280-1285 - 42.
Etemadi A, Kamangar F, Islami F, Poustchi H, Pourshams A, Brennan P, et al. Mortality and cancer in relation to ABO blood group phenotypes in the Golestan cohort study. BMC Medicine. 2015; 13 :8 - 43.
Miao SY, Zhou W, Chen L, Wang S, Liu XA. Influence of ABO blood group and rhesus factor on breast cancer risk: A meta-analysis of 9665 breast cancer patients and 244,768 controls. Asia-Pacific Journal of Clinical Oncology. 2014; 10 (2):101-108 - 44.
Costantini M, Fassio T, Canobbio L, Landucci M, Resasco M, Boccardo F. Role of blood groups as prognostic factors in primary breast cancer. Oncology. 1990; 47 (4):308-312 - 45.
Mao Y, Yang W, Qi Q , Yu F, Wang T, Zhang H, et al. Blood groups a and AB are associated with increased gastric cancer risk: Evidence from a large genetic study and systematic review. BMC Cancer. 2019; 19 (1):164 - 46.
Kolb WP, Müller-Eberhard HJ. The membrane attack mechanism of complement. Verification of a stable C5-9 complex in free solution. The Journal of Experimental Medicine. 1973; 138 (2):438-451 - 47.
Lintner KE, Wu YL, Yang Y, Spencer CH, Hauptmann G, Hebert LA, et al. Early components of the complement classical activation pathway in human systemic autoimmune diseases. Frontiers in Immunology. 2016; 7 :36 - 48.
Berentsen S, Hill A, Hill QA, Tvedt THA, Michel M. Novel insights into the treatment of complement-mediated hemolytic anemias. Therapeutic Advances in Hematology. 2019; 10 :2040620719873321 - 49.
Seidel UJ, Schlegel P, Lang P. Natural killer cell mediated antibody-dependent cellular cytotoxicity in tumor immunotherapy with therapeutic antibodies. Frontiers in Immunology. 2013; 4 :76 - 50.
Sanchez-Martinez D, Allende-Vega N, Orecchioni S, Talarico G, Cornillon A, Vo DN, et al. Expansion of allogeneic NK cells with efficient antibody-dependent cell cytotoxicity against multiple tumors. Theranostics. 2018; 8 (14):3856-3869 - 51.
Shimasaki N, Jain A, Campana D. NK cells for cancer immunotherapy. Nature Reviews. Drug Discovery. 2020; 19 (3):200-218 - 52.
Myers JA, Miller JS. Exploring the NK cell platform for cancer immunotherapy. Nature Reviews. Clinical Oncology. 2021; 18 (2):85-100 - 53.
Luo Q , Pan M, Feng H, Wang L. ABO blood group antigen therapy: A potential new strategy against solid tumors. Scientific Reports. 2021; 11 (1):16241 - 54.
O'Donnell JS, Teng MWL, Smyth MJ. Cancer immunoediting and resistance to T cell-based immunotherapy. Nature Reviews. Clinical Oncology. 2019; 16 (3):151-167 - 55.
Le Pendu J, Marionneau S, Cailleau-Thomas A, Rocher J, Le Moullac-Vaidye B, Clément M. ABH and Lewis histo-blood group antigens in cancer. APMIS. 2001; 109 (1):9-26 - 56.
Ørntoft TF, Bech E. Circulating blood group related carbohydrate antigens as tumour markers. Glycoconjugate Journal. 1995; 12 :200-205 - 57.
Langkilde NC, Wolf H, ØRntoft TF. Lewis antigen expression in benign and malignant tissues from RBC Le (a—b—) cancer patients. British Journal of Haematology. 1991; 79 (3):493-499 - 58.
Brierley C, Staves J, Roberts C, Johnson H, Vyas P, Goodnough L, et al. The effects of monoclonal anti-CD47 on RBCs, compatibility testing, and transfusion requirements in refractory acute myeloid leukemia. Transfusion. 2019; 59 (7):2248-2254 - 59.
Whiteside TL, Demaria S, Rodriguez-Ruiz ME, Zarour HM, Melero I. Emerging opportunities and challenges in cancer immunotherapy. Clinical Cancer Research. 2016; 22 (8):1845-1855 - 60.
Zonneveld R, van der Meer- Kapelle L, Sylva M, Brand A, Zijlstra M, Schonewille H. Severe fetal hemolysis and cholestasis due to high-titer maternal IgG anti-A antibodies. Pediatrics. 2019; 143 (4):e20182859 - 61.
Fan X, Lang H, Zhou X, Zhang L, Yin R, Maciejko J, et al. Induction of human blood group A antigen expression on mouse cells, using lentiviral gene transduction. Human Gene Therapy. 2010; 21 (7):877-890 - 62.
O’Donnell JS, Teng MW, Smyth MJ. Cancer immunoediting and resistance to T cell-based immunotherapy. Nature Reviews Clinical Oncology. 2019; 16 (3):151-167 - 63.
Boisgerault F, Mingozzi F. The skeletal muscle environment and its role in immunity and tolerance to AAV vector-mediated gene transfer. Current Gene Therapy. 2015; 15 (4):381-394 - 64.
Miller A, Nace R, Steele M, Bailey K, Peng KW, Russell SJ. Perfusion pressure is a critical determinant of the intratumoral extravasation of oncolytic viruses. Molecular Therapy. 2016; 24 (2):306-317