
Abstract
Esodeviations refer to misalignments where one or both eyes are turned toward the nose. Various factors contribute to this misalignment, such as disorders in horizontal rectus muscles, refractive errors, and accommodative convergence. The classification of esotropia is based on manifestations, accommodation issues, and consistency with gazes. Latent deviations, termed esophoria, arise due to weak fusional amplitudes and become apparent when fusion is disrupted. Intermittent esotropias manifest under stress or fatigue. Constant esotropias are categorized by comitance, with comitant esotropias involving constant deviation in all gaze directions, likely caused by refractive or accommodative problems. Incomitant esotropias, prevalent in lateral rectus paralysis or medial rectus entrapment, also occur in conditions such as Duane's retraction syndrome, Mobius syndrome, and heavy eye syndrome. Abducent Nerve Palsy arises from damage or dysfunction of the sixth cranial nerve, leading to weakness or paralysis of the lateral rectus muscle. Duane syndrome, a congenital eye movement disorder, restricts eye movement, especially outward, and Moebius syndrome, a rare congenital disorder affecting cranial nerves, results in difficulties with eye coordination. Treatment for esodeviations varies based on the underlying cause and severity, including options such as vision therapy, glasses, prisms, botulinum toxin injections, or surgery to correct muscle imbalances and enhance eye alignment.
Keywords
- esodeviation
- esophoria
- lateral rectus
- abducens nerve
- strabismus
- sixth cranial nerve
- esotropia
- squint
- recession
- resection
- transposition
- Duane
1. Introduction
Esodeviations are the misalignments, in which one or both eyes are positioned towards the nose. Esodeviations are the most common childhood strabismus and equally prevalent to the exodeviations in adults. A lot of factors are responsible for the misalignment of eyes, which include horizontal rectus muscles disorders [1], refractive errors, accommodative convergence etc. The risk factors include hyperopia, anisometropia, low birth weight, prematurity, neural developmental impairment [2].
Esotropia can be classified on the basis of manifestation, accommodation problems and consistency with gazes. The deviation may be manifest or latent. The latent deviations are known as the esophoria, while manifest deviations are known as esotropia, which are further classified as constant or intermittent, comitant or incomitant esotropias.
Esophorias are latent esodeviations, which are caused by weak fusional amplitudes and become prominent as fusion is break under cover. Intermittent esotropias, on the other hand, include the esodeviations which become manifest during stress or fatigue.
Constant esotropias are further grouped on the basis of comitance. In comitant esotropias both eyes remain constantly deviated to each other’s in all gaze directions, these are most likely due to refractive or accommodative problems. While incomitant esotropias are present mostly in lateral rectus paralysis or medial rectus entrapment in medial orbital wall fractures [3]. The other causes of incomitant esotropia include syndromes like, Duane’s retraction syndrome, Mobius syndrome, heavy eye syndrome etc.
Treatment of esotropia include refractive correction, convergence exercises and muscle surgery.
2. Esophoria
As fusion controls the alignment and keeps the eyes straight with binocular single vision. Sometimes the fusional amplitudes are not much strong to keep eye aligned as fusion breaks. Esophoria is the latent esodeviation that affects eye coordination. Due to insufficient fusional amplitudes, the covered eye tends to deviate nasally as fusion is broken by cover or both eyes focus on different objects.
2.1 Treatment
Refractive correction
Prisms; Temporary stick-on Fresnel prisms or spectacles incorporated, maximally 10∆–12∆ split between both eyes.
Surgery; occasionally for large esophorias.
3. Comitant esotropias
These are manifest esodeviations in which the angle of deviation remains constant in all directions of gaze. A variety of comitant esotropic deviations are known.
3.1 Essential infantile esotropia
Manifest by 6 months of age (Figure 1)
Large esodeviation >40Δ–50 Δ (Figure 2)
Equal at distance & near
Normal to age refractive error (hypermetropic)
Cross fixation is common.
Amblyopia is uncommon.
Prohibits fusion and binocular vision.
Inferior oblique overaction
Latent nystagmus
Dissociated vertical deviation may present.

Figure 1.
Infantile esotropia in a 4-month-old child.

Figure 2.
Infantile esotropia in a 2-year-old child, presented late in a screening clinic.
3.1.1 Management
Cycloplegic refraction to rule out refractive causes.
Early bilateral medial rectus recession
3.2 Acquired nonaccommodative esotropia
Develops after 6 months of age (Figure 3).
Esodeviation not corrected by convex lenses (Figure 4).
Starts as intermittent, became as constant.
Small esodeviation, 20Δ–35Δ
Diplopia may present.

Figure 3.
Acquired non-accommodative esotropia, patient dilated for cycloplegic refraction.

Figure 4.
Refractive correction not effective.
3.2.1 Management
Bilateral medial rectus recession
In children <6 years, MRI brain must be done to exclude posterior fossa pathology [4].
3.3 Accommodative esotropia
It is the esodeviation which is associated with the activation of near or accommodative reflex. In accommodation eyes focus on near objects by increasing the curvature of crystalline lens, known as accommodation power (A) and simultaneously converge to focus on object of interest, known as accommodation convergence (AC). Abnormalities in AC/A ratio causes accommodative type of esodeviation. It may present between 6 months and 6 years of age (mean 2½ years). It is further classified into;
3.3.1 Refractive accommodative esotropia
Mostly present between 1½ year and 3 years (Figures 5 and 6)
AC/A ratio is normal
Excessive hyperopia +2.0D - +10.0D, which cause
High accommodation convergence (beyond fusional amplitude)
Amblyopia may present

Figure 5.
Refractive accommodative esotropia.

Figure 6.
Refractive accommodative esotropia.
3.3.1.1 Fully accommodative esotropia
Can be fully aligned by hyperopic correction (Figure 7)
BSV is present

Figure 7.
Fully accommodative esotropia, orthophoric with refractive correction.
3.3.1.2 Partially accommodative esotropia
Deviation is reduced but not fully corrected by refraction (Figure 8)
Amblyopia is common as suppression of squinting eye
ARC may occur
Surgical correction is usually performed on squinting or amblyopic eye

Figure 8.
Partially accommodative esotropia, lessen with refractive correction.
3.3.2 Non-refractive accommodative esotropia
High AC/A ratio
Independent of refractive error (hyperopia and myopia) but hyperopia is frequent
Straight eyes for distance (with BSV)
Esotropia for near, suppression is usually present in squinted eye
3.3.2.1 Convergence excess
Increased accommodation convergence (AC) with normal accommodation (A)
Near point of accommodation is normal
Orthophoric with bifocals, executive type is preferred
Bilateral medial rectus is performed
3.3.2.2 Hypo-accommodative convergence excess
Normal accommodation convergence (AC) with decreased accommodation (A)
Near point of accommodation is remote
Executive type bifocals may be advised for near work
Surgical correction may be considered only when refractive correction is not sufficient.
3.4 Non-accommodative convergence excess/near esotropia
Presents in young adults and older children (Figure 9)
Esotropia for near
Orthophoric/small esophoria with BSV for distance
Non-significant refractive error (Figure 10)
Normal or low AC/A ratio
Near point of accommodation is normal

Figure 9.
Non-accommodative convergence excess esotropia.

Figure 10.
Non-significant refractive error, which is also not correcting esotropia.
3.4.1 Treatment
Bilateral medial rectus recessions.
3.5 Distance esotropia
Presents in myopic healthy young adults
Esotropia for distance, may be intermittent
Orthophoric for near
Normal bilateral abduction
Reduced fusional divergence amplitudes
No neurological deficit
3.5.1 Treatment
Prisms until spontaneous resolution
Surgery if persists
3.6 Acute esotropia/late-onset esotropia
Presents usually around 5 years–6 years of age but in young adults too
Sudden onset of esotropia and diplopia (Figure 11).
Non-significant refractive error
Normal ocular motility
Underlying neurological disorder may present

Figure 11.
Acute onset esotropia in 17-year-old male with history of sudden onset of diplopia 2 weeks ago. Fundus examination reveals bilateral disc swelling.
3.6.1 Management
Cranial nerve examination
Pupil reflexes
Fundus examination for optic disc pathology
Re-establishing BSV
Prevent suppression
3.6.2 Treatment
Prisms with glasses
Botulinum toxin in medial rectus
Strabismus correction surgery
3.7 Sensory-deprivation esotropia
In children younger than 4 years of age, many organic conditions cause impaired focusing to light to retina and perception by the visual cortex, thus hindring the fusion development. This causes the eye to deviate inwards nasally. In older children and adults these cause the sensory exotropia. These conditions may be uniocular or binocular as;
Uncorrected refractive errors
Anisometropic hypermetropia
Severe ptosis (Figure 12)
Buphthalmos
Corneal opacities
Congenital corneal dystrophies
Congenital cataracts
PHPV and persistent fetal vasculature
Retinopathy of prematurity
Retinal and optic disc colobomas
Retinal detachments
Macular dystrophies
Retinoblastoma
Coats disease
Optic nerve anomalies etc.

Figure 12.
Sensory-deprivation esotropia due to severe ptosis secondary to lid hemangioma in 8 months old child.
3.7.1 Treatment
Dilating fundus examination to establish the cause.
Treating the underlying cause first.
Amblyopia therapy
Cosmetic strabismus correction
3.8 Consecutive esotropia
Consecutive esotropia is said when an exotropic person becomes esotropic. It is usually caused by the surgical correction of exotropia, with incidence rate reported between 6 and 20%. The factors involve in the overcorrection of divergent squints;
Poor vision
Congenital retinal or optic nerve anomalies
Intermittent distance exotropia (IDEX)
3.8.1 Treatment
Comitant small deviation (10Δ–15Δ) should be observe for 2 weeks for spontaneous resolution.
Re-do strabismus correction by medial rectus recession or lateral rectus advancement in patients with good vision.
Repeated botulinum toxin injections in medial rectus muscle is preferred in patients with poor vision.
3.9 Divergence insufficiency
Common in elderly patients
Esotropia; distance fixation > near fixation
Diagnosis of exclusion
Caused by the weakening or rupturing of connective tissue between lateral rectus muscle and superior rectus muscle, causing sagging of lateral rectus muscle [5].
Associated with neurologic trauma, pontine tumors, raised intracranial pressure.
3.9.1 Management
Spontaneous resolution
Base out prisms in glasses.
3.10 Cyclic esotropia
It is a rare condition which is mostly characterized by esotropia lasting for 24 hours alternating with 24 hours of orthophoria. The incidence is 1 in every 3000–5000 patients. Cyclic esotropia may persist for months or years until it develops into a constant esotropia.
3.10.1 Treatment
Both eyes medial rectus recession has good results. Measurement is done on the basis of photographic evidence or the orthoptic assessment during the esotropic cycle, or until the esotropia becomes constant.
4. Incomitant esodeviations
In contrast to the comitant esodeviations, in which the degree of deviation remains constant in all directions of gazes, angle of deviation increases in lateral gaze while fixating distantly in incomitant esodeviation. Incomitant esodeviations are caused by;
4.1 Central nervous system pathologies
Increased intracranial pressure
Acquired sixth nerve palsy
4.2 Medial rectus restriction
Thyroid eye disease
Muscle entrapment in medial orbital wall fracture
4.3 Lateral rectus weakness
Isolated sixth nerve palsy
Slipped/detached lateral rectus muscle from trauma/surgery.
5. Abducens nerve palsy
Abducens Nerve is the Sixth Cranial nerve and responsible for the movement of the Lateral rectus nerve. The sixth nerve palsy is the most common extraocular muscle palsy in adults and second most common in children.
5.1 Presentation
Convergent squint due to unopposed action of antagonist Medial rectus
The esotropia is incomitant, greater in looking towards affected gaze and more at fixing distance than near.
Diplopia; binocular and horizontal, worsen for distant vision and in direction of paretic muscle.
5.2 Etiology
As the abducens nerve has the longest intracranial course among all cranial nerves, hence it is more prone to the damage.
Congenital [6]
Associated with birth trauma,
Hydrocephalus
Cerebral palsy,
Acquired [7]
Tumor,
Trauma,
Inflammation,
Infection
Idiopathic.
Common causes
Vasculopathies due to microvascular ischemia,
Trauma (Figure 13)
Idiopathic
Other causes include:
Stroke
Multiple sclerosis,
Raised intracranial pressure,
Cavernous sinus mass; aneurysm, meningioma, tumor metastasis
Sarcoidosis
Vasculitis
Lymes disease
Neurosyphilis

Figure 13.
Traumatic left sixth nerve palsy in 45-year-old female.
5.3 Differential diagnosis
The differentials of limited abduction involve:
5.3.1 Thyroid eye disease
Lid Retraction
Lid Lag
Injection over involved rectus
Positive FDT (Forced Duction Test)

Figure 14.
Esodeviation in thyroid eye disease. Right eye supro-nasal misalignment. Proptosis and lid retraction are also notable in both eyes.
5.3.2 Myasthenia gravis
Diplopia is fluctuating, variable and fatigable [8].
Ptosis is common.
Generalize fatigability may present.
Shortness of breath and hoarseness
Positive ice and rest tests
5.3.3 Duane retraction syndrome, type 1
Congenital
Narrowing of the palpebral fissure in adduction (Figure 15)
Retraction of globe

Figure 15.
Duane retraction syndrome, right eye induced ptosis and left eye abduction deficit.
5.3.4 Mobius syndrome
Congenital
Bilateral facial paralysis
5.3.5 Convergence spasm
Intermittent, variable convergence
Miosis
Deficient Abduction in versions but with full ductions
5.3.6 Primary divergence insufficiency
Acquired
Esotropia
Diplopia at distance with binocular single vision (BSV) at near
5.3.7 Giant cell arteritis GCA
Extraocular muscle ischemia
Age > 55 years
5.4 Management & work up
5.4.1 Children
History:
Birth trauma,
Recent illness,
Neurological symptoms,
Ear infections
Complete Ophthalmic & Neurological Examination
MRI brain
5.4.2 Adults
History:
Onset & progression,
Systemic diseases; hypertension, diabetes, thyroid dysfunction,
Complete Ophthalmic & Neurological Examination:
Extraocular movements,
Corneal sensation,
Fundus examination for optic disc (swelling /papilledema)
Hess Chart (Figure 16)
Underation of ipsilateral lateral rectus muscle
Normal/overaction of contralateral medial rectus muscle
Systemic Examination; blood pressure,
Laboratory Examination:
Fasting blood sugar
HbA1c,
Serum lipid profile
ESR
CRP
CSF analysis
Lyme antibody titer
FTA-ABS or treponemal-specific assay, VDRL or RPR
MRI Brain
In all patients younger than 45 years,
Non-isolated sixth nerve lesion,
History of neoplasms,
Patients without microvascular diseases.
Papilledema
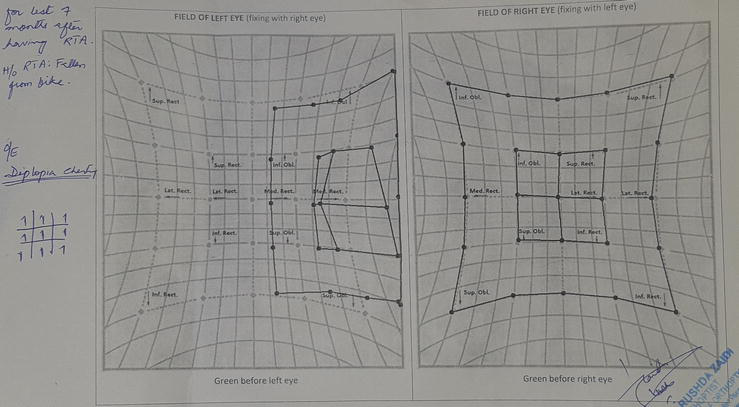
Figure 16.
Hess chart of 45-year-old patient, with history of road traffic accident 8 month ago, showing left lateral rectus under-action. Medial rectus muscles of both eyes showing no overaction. Due to compensatory head posture towards left the patient has no complaint of diplopia.
5.5 General treatment
Treat the underlying etiology.
Abducens nerve palsy due to microvascular causes are observed as they recover within 3 to 6 months.
Diplopia is managed by [9].
Occlusion; Bangerter filter, eye patch, central glass patch. It eliminates confusion and diplopia, prevents suppression and amblyopia, and minimizes contracture of ipsilateral medial rectus. In patients <10 years, patching is avoided due to high risks of amblyopia.
Base-out Fresnel or ground in prisms. Limited role in maintaining BSV as the deviation is incomitant.
Botulinum Toxin: it is injected into medial rectus to prevent secondary contracture and to weak medial rectus in transposition procedures.
Surgical intervention is advised only in patients having stable deviations for at least 6 months.
Follow up every 6 weeks until the resolution of palsy or stabilization of deviation.
5.6 Surgical management
5.6.1 Aim
Surgical correction is always planned for realignment of the globe in primary position [10].
5.6.2 Surgical protocols
Surgical management of the Lateral Rectus disorder in patients having stable orthoptic measurements for more than 6 months, depends upon [11];
Medial rectus fibrosis
Lateral rectus residual function
For medial rectus fibrosis, forced duction test is performed. If FDT is positive that shows tight medial rectus, recession of the medial rectus is done (Figure 17).
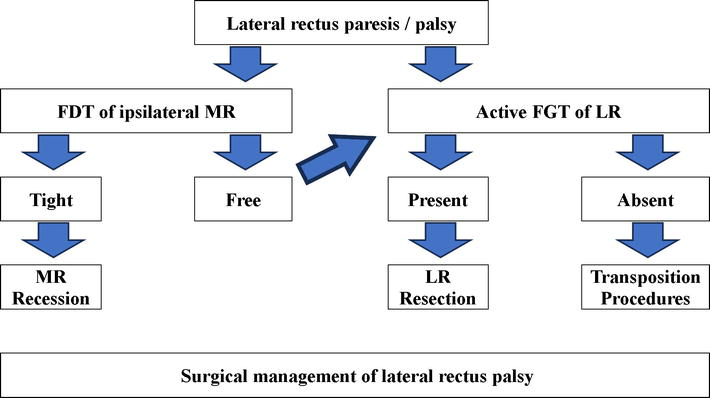
Figure 17.
Surgical management for lateral rectus palsy, based on the standard treatment protocol described by American Academy of ophthalmology.
For lateral rectus, active force generation test (FGT) is performed.
Active FGT present; Resection of LR
Active FGT absent; transposition procedures
If lateral rectus shows any residual function, then recession of ipsilateral MR along with supra-maximum (12–14 mm) resection of lateral rectus is performed.
5.7 Transposition surgeries for lateral rectus muscle palsy
When there is no LR function on active FGT, a variety of transposition surgeries can be planned for realigning the eyes in primary position, these include; (Figure 18).
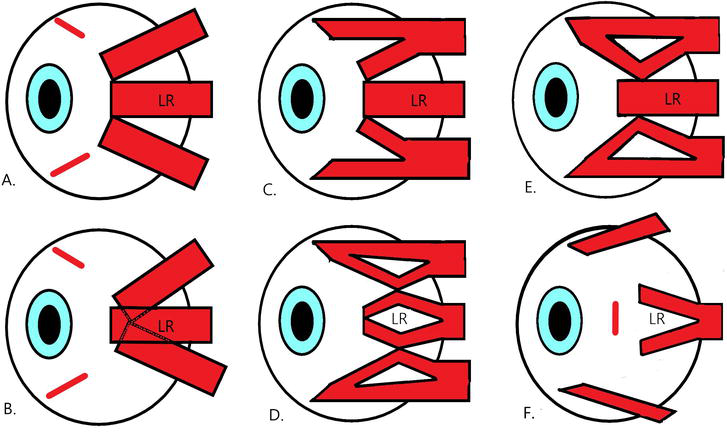
Figure 18.
Diagrammatic presentation of surgeries to treat lateral rectus palsy/disorders. A. Full tendon transposition; B. Full tendon transposition with cross-adjustable technique; C. Hummelsheim procedure; D. Jensen’s procedure; E. Nishida’s procedure; F. LR recession with possible Y-splitting for treating leash phenomenon in Duane’s retraction syndrome.
5.7.1 Full tendon transposition
Disinsertion of full width tendons of superior and inferior recti and transposing them towards lateral rectus insertion [12]. This procedure has risk of anterior segment ischemia which can be minimized by conserving muscular branches of anterior ciliary artery, and avoiding extensive dissection (Figure 18A).
5.7.2 Cross-adjustable technique
To increase the effectiveness of the full tendon transposition by increasing path length to avoid the resection of vertical rectus muscles, the tendons are passed beneath the LR tendon and attached at the opposite corners of LR Insertion [13]. This technique also decreases the need of ipsilateral MR recession in many cases (Figure 18B).
5.7.3 Hummelsheim
Vertical recti are split half tendon width up to 14 mm approximately from the insertion. The temporal halves of superior and inferior recti are disinserted and transposed to the lateral rectus insertion [14]. Care must be taken to preserve the anterior ciliary vessels during procedure (Figure 18C).
5.7.4 Augmented/modified Hummelsheim
Transposed half tendons are further resected to increase the effectiveness of Hummelsheim procedure along with medial rectus recession. It is reported to correct deviation up to 40Δ ± 5Δ [15].
5.7.5 Jensen’s procedure
First described by Jensen et al. in 1964 [16], the bellies of superior and inferior recti are split half tendon width and tied to lateral rectus muscle without disinsertion, 12–14 mm behind from the insertion with non-absorbable suture (Figure 18D). To avoid anterior segment ischemia, at least one ciliary artery must be protected. In vessel sparing modification of Jensen’s procedure, the split muscles are stitched together by looping stitch underneath the vessels.
5.7.6 Nishida’s procedure
This procedure was described by Nishida et al. in 2003 [17]. In this technique the vertical rectus muscles are exposed by limbal based peritomy. After dissecting intermuscular septum along lateral margin of each muscle, vertical recti are split half tendon width up to 15 mm from the insertion. With 6–0 nylon sutures, lateral half of each muscle is secured at 8–10 mm from the insertion and anchored at 8 mm posterior to LR insertion to sclera (Figure 18E).
5.7.7 Superior rectus transposition
Jhonston et al. described transposition of the superior rectus muscle only to the lateral rectus insertion [18]. It was postulated to prevent anterior segment ischemia and to simplify the procedure. The procedure improves esotropia, abduction and head turn with minimal vertical misalignment.
5.7.8 Inferior rectus transposition
Alternative to superior rectus transposition, this procedure is helpful to improve esotropia, abduction limitation and head turn, along with the correction of hypertropia [19].
5.8 Follow up
Postoperatively, patients should be managed under close observation. Prisms should be prescribed for any residual diplopia. Since there are increased chances of anterior segment ischemia in the first 6 months of the primary surgery, hence the repeat surgery should always be planned after 6 months of primary surgery, providing the ample time for collaterals to develop.
5.9 Surgical complication
Anterior segment ischemia [20]
Under correction; of primary esotropia and head posture
Over correction; consecutive exotropia
Diplopia
Induced vertical deviations [21].
Conjunctival cyst
Conjunctival prolapse.
Corneal dellen
Tenon’s prolapse.
Scleral perforation
Lost/Slipped Muscle
Bradycardia
Secondary infections.
5.10 Prognosis
Rush JA reported an overall recovery rate of 49.6%, with 71% recovery in patients with systemic diseases (diabetes mellitus, hypertension, atherosclerosis etc.) [22].
6. Duane syndrome
It is also known as Stilling-Turk-Duane syndrome. Duane syndrome was first described in 1905 by Alexander Duane [23]. It is congenital, non-progressive syndrome [24] characterized by some or all of the following:
Abduction limitation, usually complete (Figure 19)
Globe retraction on attempted adduction
Induced Ptosis; narrowing of palpebral fissure on adduction (Figure 19).
Adduction limitation, usually partial [25]
Oblique movement on attempted adduction
Leash Phenomenon, Upshoot or downshoot of globe with adduction
Widening of palpebral aperture on abduction
Convergence insufficiency
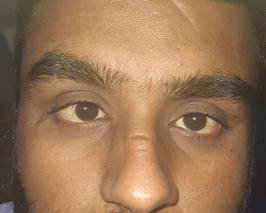
Figure 19.
Duane type 1, right small angle esotropia in primary gaze.
6.1 Types
Duane retraction syndrome is divided into three types with multiple subgroups; the difference in clinical features are;
6.1.1 Type 1
6.1.2 Type 2
5–10% of patients [26]
Exotropia in primary gaze
Compensatory head turn to the uninvolved side.
6.1.3 Type 3
10–20% of patients [26]
Present with either an esotropia or exotropia in primary gaze
Compensatory head turn to the involved side
The ability to adduct in this type is absent to restricted as compared to normal to mildly restricted in types 1 and 2.
6.2 Etiology
6.3 Pathophysiology
Duane syndrome results from aberrant lateral rectus innervation by third nerve as abducens motor neurons are absent or dysplastic.
6.3.1 Myogenic theory
It suggests that lateral rectus is fibrosed or inelastic and medial rectus has abnormal far posterior insertion [26].
6.3.2 Neurogenic theory
It was suggested by postmortem studies at John Hopkins University in 1980 [29]. At 4–8 weeks of gestation, a disturbance in embryologic development results in abducens nerve absent which causes aberrant lateral rectus innervation by third nerve [29]. Hence both MR & LR are innervated by oculomotor nerve, their simultaneous activation results in globe retraction [30].
6.4 Diagnosis
Duane syndrome is diagnosed primarily based on clinical features:
6.5 Management
6.5.1 Evaluation
History: onset, trauma, family history, other ocular or systemic diseases [27].
Complete ophthalmic examination; visual acuity, extraocular movements, aberrant movements and retractions, compensatory head position,
Systemic examination, cranial nerves evaluation
Forced duction and active force generation tests to evaluate tight muscles.
Genetic evaluation and counseling when familial pattern is noted [26].
MRI brain and orbit, for visualization of anatomy.
6.5.2 Non-surgical management
Refractive correction by glasses or contact lens [26]
Corrective prisms for abnormal head posture [26]
Amblyopia prevention & treatment; new cases must be evaluated 3–6 monthly [26].
Botulinum Toxin: to minimize leash phenomenon [31].
Children >7 years with good vision and binocularity can be evaluated annually [26].
6.6 Surgical management
6.6.1 Limitations
Cannot fully cure the disease.
Only correct tropias in primary gaze
Improve head posture.
Improve leash phenomenon [26]
Either recessions only or transpositions are done; muscle resections can never be planned.
6.6.2 Indications
6.6.4 Surgical procedures
A variety of surgeries have been advised depending upon the type and clinical features of the disease.
DRS type 1 & 3 + face turn
Based on FDT; MR recession only or Transposition of vertical rectus muscles to lateral rectus [35].
Full tendon transposition of vertical recti (Figure 18A).
Full tendon transposition with cross-adjustable technique
Jensen’s procedure (Figure 18D).
Nishida’s procedure (Figure 18E).
Superior rectus transposition
Inferior Rectus transposition
DRS type 1 & 3 + Leash phenomenon/severe globe retraction
Recession of both MR & LR with possible Y-splitting of LR [26] (Figure 18F).
DRS type 2 + face turn (fixation with uninvolved eye)
Ipsilateral LR recession [26]
DRS type 2 + face turn (fixation with involved eye)
Contralateral LR recession [26]
DRS type 2 + Leash phenomenon
Ipsilateral LR recession with possible Y-splitting (Figure 18F) [26].
7. High myopia esotropia
In patients with high myopia and large axial lengths, tenon muscle pulleys of superior rectus and lateral rectus muscles may become instable. This causes the bulging of globe through the defect of muscle pulleys resulting in inferior displacement of the lateral rectus muscle and nasal displacement of the superior rectus muscle.
7.1 Management
Magnetic resonance imaging (MRI) should be done in every high myope with acquired esotropia to diagnose the condition. The esotropia is treated by repairing muscle pulleys by plication of the superior rectus muscle and lateral rectus muscle with a non-absorbable suture.
8. Moebius syndrome
It is a rare congenital, non-progressive syndrome involving both abducens and facial nerve palsies.
8.1 Clinical features
It is characterized by;
Lagophthalmos
Esotropia
Limitation in abduction and/or adduction
Intact vertical movements & bell’s phenomenon, saving cornea intact.
Unilateral/bilateral, partial/complete facial nerve palsy
Mask like face appearance
Cranial nerves V, VIII, X & XII may be affected too.
Tongue atrophy, limbs and chest deformities may occur.
8.2 Management
No definitive treatment
Behavioral management; suction aids
Rehabilitation; Orthopedics surgeons
Temporary tarsorrhaphy to prevent dry eye.
Medial rectus recession for esotropia
Transposition surgeries; inconsistent results
9. Idiopathic orbital inflammatory syndrome
Idiopathic orbital myositis is relatively less common, non-infective, non-granulomatous, non-neoplastic inflammation of isolated or multiple extraocular muscles. Lateral rectus is usually less involved than medial rectus.
9.1 Features
Tendon involving muscle enlargement.
Pain, more on eye movements
Proptosis
Periorbital edema
Diplopia
9.2 Management
Systemic evaluation
Autoimmune profile (CBC, ESR, ACE, ANA, cANCA, pANCA, LDH)
Imaging: Orbital MRI with DWI protocol
Corticosteroids (1 mg/kg/day)
Low dose radiation
Steroid sparing agents (methotrexate, cyclophosphamide)
10. Conclusion
Esodeviations involve a variety of disorders which cause eyes to move nasally inwards, the management depends upon addressing these disorders. In general, the management protocol involves;
10.1 Observation and systemic evaluation
Acute onset esodeviations are usually lateral rectus palsies secondary to systemic hypertension, diabetes mellitus, atherosclerosis and benign intracranial hypertension, which are usually self-resolving, subject to the treatment of underlying etiology and any life-threatening condition, if present. Systemic evaluation for the above-mentioned diseases along with the laboratory profiles and radiological imaging are key steps in observing these acute lesions.
In case of trauma involving the sixth nerve, only the emergency traumatic repairs must be performed first. The esotropia associated with traumatic sixth nerve palsy is left observed for at least 6 months before offering any surgical intervention. Non-surgical treatment options must be offered to all patients during the observation to relive diplopia and asthenopia.
10.2 Non-surgical treatment
Non-surgical treatments are aimed to restore vision, relive diplopia and asthenopia. Patching can help to treat amblyopia and minimize diplopia. In children and young adults with esotropias associated with underlying amblyopia, the healthy eye is completely patched to enhance the sensory perception of the lazy eye. While, in elder adults with lateral rectus palsy, patching the center part of glasses helps in minimizing the diplopia in primary gaze with keeping side vision intact. Full refractive correction by hyperopic convex lenses and bifocals helps in treating the accommodative esotropias and convergence excess esotropias respectively. In divergence insufficiency, divergence orthoptic exercises are advised with or without prisms. Prescribing prisms may relieve diplopia well. Prism glasses and Fresnel prisms are tolerated well in patients who are kept under observation before planning any surgical procedure. Medical management is necessary for the esotropia associated with systemic diseases. In addition to the systemic medicines, some of the drugs used are vitamin B12, corticosteroids and disease modifying agents. Corticosteroids by their anti-inflammatory effects are prescribed in thyroid eye disease, myositis and traumatic brain and orbital injuries. Botulinum toxin has gained much popularity for non-surgical chemo-denervation of the medial rectus muscle in treating infantile and acute esotropias. It also helps to prevent medial rectus fibrosis in lateral rectus palsy and also help to prevent anterior chamber ischemia by sparing medial rectus recession in transposition procedures.
10.3 Surgical treatment
The main aim of surgical treatment is to attempt in developing a good binocular single vision by restoring the regular alignment of both eyes and addressing any pathology causing sensory deprivation. Treating ptosis, cataract and other causes are sometimes more important than to treat the esotropia alone. In medial rectus muscle entrapments, medial orbital wall is repaired as early as possible to avoid the development of muscle fibrosis and ischemia. in treating abnormal head posture and diplopia, surgical options must be considered to offer, only when there are more than 6 months passed with static orthoptic measurements. It is advised to treat amblyopia prior to surgery but sometimes surgery, itself, is the only option to treat the amblyopia as early as possible, before development of any degeneration at the level of lateral geniculate nucleus. Intermittent esotropias have good surgical prognosis over constant and alternating ones. The typical surgical approach for comitant esotropia is bilateral medial rectus recession or unilateral medial rectus recession and lateral rectus resection (recess-resect procedure). In incomitant esotropias surgical approaches vary with the type of esotropia, as transposition of vertical recti. Different transposition procedures of vertical rectus muscles are done to compensate for the limited abduction. These procedures include full tendon transposition, partial tendon vertical transposition, split muscle transpositions etc. The main complication of these surgeries is the anterior segment ischemia, which can be avoided by preserving muscular arteries during surgery. Other complications include under corrections and induced vertical deviations. Loop myopexy is considered for myopic esotropia /heavy eye syndrome.
Acknowledgments
I would like to acknowledge the motivation given by Dr. Muna Malik, and her help in typing, proofreading and reviewing this manuscript.
The project is not funded by any sponsor and all the expenses were borne by the author himself.
Conflict of interest
The author declares no conflict of interest.
Notes/thanks/other declarations
Thanks to my colleagues and patients who gave me strength to write this chapter.
All pictures are taken with the consent of patients, subjected not to disclose their particulars and full-face identity. The diagrams are made by the author.
References
- 1.
Cabrera AF, Suárez-Quintanilla J. Anatomy, Head and Neck, Eye Lateral Rectus Muscle. Treasure Island (FL): StatPearls Publishing [Internet]; 2022 - 2.
Bohnsack BL, Gallina D, Thompson H, Kasprick DS, Lucarelli MJ, Dootz G, et al. Development of extraocular muscles requires early signals from periocular neural crest and the developing eye. Archives of Ophthalmology. 2011; 129 (8):1030-1041 - 3.
Shumway CL, Motlagh M, Wade M. Anatomy, Head and Neck, Eye Extraocular Muscles. Treasure Island (FL): StatPearls Publishing [Internet]; 2021 - 4.
Liu JK. Combined petrosal approach for resection of a large trigeminal Schwannoma with Meckel's cave involvement-part II: Microsurgical approach and tumor resection: 2-dimensional operative video. Operative Neurosurgery (Hagerstown, Md.). 2021; 20 (3):E226 - 5.
Chaudhuri Z, Demer JL. Sagging eye syndrome: Connective tissue involution as a cause of horizontal and vertical strabismus in older patients. JAMA Ophthalmology. 2013; 131 (5):619-625 - 6.
McKay VH, Touil LL, Jenkins D, Fattah AY. Managing the child with a diagnosis of Moebius syndrome: More than meets the eye. Archives of Disease in Childhood. 2016; 101 (9):843-846 - 7.
Teksam O, Keser AG, Konuskan B, Haliloglu G, Oguz KK, Yalnizoglu D. Acute abducens nerve paralysis in the pediatric emergency department: Analysis of 14 patients. Pediatric Emergency Care. 2016; 32 (5):307-311 - 8.
Kung NH, Van Stavern GP. Isolated ocular motor nerve palsies. In: Seminars in Neurology. Vol. 35, No. 5. New York, NY, USA: Thieme Medical Publishers; 2015. pp. 539-548 - 9.
Heckmann JG, Vachalova I, Lang CJ, Pitz S. Neuro-ophthalmology at the bedside: A clinical guide. Journal of Neurosciences in Rural Practice. 2018; 9 (4):561-573 - 10.
Rosenbaum AL. The efficacy of rectus muscle transposition surgery in esotropic Duane syndrome and VI nerve palsy. Journal of American Association for Pediatric Ophthalmology and Strabismus. 2004; 8 (5):409-419 - 11.
von Noorden GK. A reassessment of infantile esotropia XLIV Edward Jackson memorial lecture. American Journal of Ophthalmology. 1988; 105 (1):1 - 12.
Schillinger RJ. A new type of tendon transplant operation for abducens paralysis. The Journal of the International College of Surgeons. 1959; 31 (5):593-600 - 13.
Phamonvaechavan P, Anwar D, Guyton DL. Adjustable suture technique for enhanced transposition surgery for extraocular muscles. Journal of American Association for Pediatric Ophthalmology and Strabismus. 2010; 14 (5):399-405 - 14.
Hummelsheim E. Weitere Erfahrungen mit partieller Sehnenuberpflanzung an den Augenmuskeln. Arch Augenheilkd. 1908; 62 :71-74 - 15.
Couser NL, Lenhart PD, Hutchinson AK. Augmented Hummelsheim procedure to treat complete abducens nerve palsy. Journal of American Association for Pediatric Ophthalmology and Strabismus. 2012; 16 (4):331-335 - 16.
Jensen CD. Rectus muscle union: A new operation for paralysis of the rectus muscle. Transactions of the Pacific Oto-Ophthalmological Society. 1964; 45 :359-387 - 17.
Nishida Y, Inatomi A, Aoki Y, Hayashi O, Iwami T, Oda S, et al. A muscle transposition procedure for abducens palsy, in which the halves of the vertical rectus muscle bellies are sutured onto the sclera. Japanese Journal of Ophthalmology. 2003; 47 (3):281-286 - 18.
Johnston SC et al. ARVO abstract. IOVS. 2006; 47 :2475:ARVO E-Abstract - 19.
Velez FG, Chang MY, Pineles SL. Inferior rectus transposition: A novel procedure for abducens palsy. American Journal of Ophthalmology. 2017; 177 :126-130 - 20.
von Noorden GK. Anterior segment ischemia following the Jensen procedure. Archives of Ophthalmology. 1976; 94 (5):845-847 - 21.
Ruth AL, Velez FG, Rosenbaum AL. Management of vertical deviations after vertical rectus transposition surgery. Journal of American Association for Pediatric Ophthalmology and Strabismus. 2009; 13 (1):16-19 - 22.
Rush JA, Younge BR. Paralysis of cranial nerves III, IV, and VI: Cause and prognosis in 1,000 cases. Archives of Ophthalmology. 1981; 99 (1):76-79 - 23.
Kirkham TH. Inheritance of Duane's syndrome. The British Journal of Ophthalmology. 1970; 54 (5):323 - 24.
McKusick VA, O’Neill MJ. Duane Retraction Syndrome 1. Hereditary Ocular Disease. USA: University of Arizona, Department of Ophthalmology and Vision Science; 2016. Available from: http://disorders.eyes.arizona.edu/disorders/duane-retraction-syndrome-1 [Accessed: February 4, 2024] - 25.
Elliot AJ. Duane's retraction syndrome. Proceedings of the Royal Society of Medicine. 1945; XXXVIII :463-465 - 26.
Barry BJ, Whitman MC, Hunter DG, et al. Duane Syndrome. 2007 May 25 [Updated 2019 Aug 29]. In: Adam MP, Feldman J, Mirzaa GM, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2024. Available from: https://www.ncbi.nlm.nih.gov/books/NBK1190/ [Accessed: February 4, 2024] - 27.
Murillo-Correa CE, Kon-Jara V, Engle EC, Zenteno JC. Clinical features associated with an I126M α2-chimaerin mutation in a family with autosomal-dominant Duane retraction syndrome. Journal of American Association for Pediatric Ophthalmology and Strabismus. 2009; 13 (3):245-248 - 28.
Miyake N, Andrews C, Fan W, He W, Chan WM, Engle EC. CHN1 mutations are not a common cause of sporadic Duane’s retraction syndrome. American Journal of Medical Genetics. Part A. 2010; 152 (1):215 - 29.
Hotchkiss MG, Miller NR, Clark AW, Green WR. Bilateral Duane's retraction syndrome: A clinical-pathologic case report. Archives of Ophthalmology. 1980; 98 (5):870-874 - 30.
Duane TD. Clinical ophthalmology. In: Pediatric Ophthalmic Surgery. Vol. 6. Philadelphia, PA: Lippincott Williams & Wilkins; 1994 - 31.
Talebnejad MR, Sahraian N, Eghtedari M. Management of Duane’s syndrome with botulinum toxin injection. Iranian Journal of Ophthalmology. 2008; 20 (3):10-14 - 32.
Barbe ME, Scott WE, Kutschke PJ. A simplified approach to the treatment of Duane’s syndrome. British Journal of Ophthalmology. 2004; 88 (1):131-138 - 33.
Duane TD. Clinical ophthalmology. In: Strabismus, Refraction, the Lens. Vol. 1. Philadelphia, PA: Lippincott Williams & Wilkins; 1993 - 34.
Jampolsky A. Duane syndrome. In: Rosenbaum AL, Santiago AP, editors. Clinical Strabismus Management. Philadelphia: W.B. Saunders & Co; 1999. p. 331 - 35.
Doyle JJ, Hunter DG. Transposition procedures in Duane retraction syndrome. Journal of American Association for Pediatric Ophthalmology and Strabismus. 2019; 23 (1):5-14