Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
This chapter deals with the first month of life of the newborns in India. Although it is a global issue, the chapter focuses on the issue giving the history, perspective, current situation, and the future of newborns in India. Being the second most populous country in the world, the lessons learnt from India on neonatal care can be adopted by other countries. The application of the neonatal care on a large scale in India has been slow and gradual as it needs a multidimensional strategy. The neonatal care is at two poles. One at the in-reach and the other at the level of out-reach. The former is at the institutional level and the later at the institutional level. Both the concepts are detailed out in the chapter. The chapter also factors in the multiheaded dependent indicator, such as neonatal mortality rate, that impacts poverty, and thus social development. The chapter discusses the child survival interventions through the reduction of child mortality in India and aspires that India achieve the sustainable development goal related to child mortality.
Public Health (Community Medicine) Program, Department of Social Work, Lucknow University, Lucknow, UP, India
Shankar Das
School of Health Systems Studies, Tata Institute of Social Sciences, Mumbai, India
Dharmendra Pratap Singh
Centre of Research Methodology, Tata Institute of Social Sciences, Mumbai, India
Sovesh Chandra Tripathy
IB Valley Coal Fields, Jharsuguda, Odisha, India
Anjali Tripathy
LLF, Lucknow, India
Sanskriti Tripathy
Bennet University, Greater Noida, Uttar Pradesh, India
Rakesh Dwivedi
Department of Social Work, Lucknow University, Lucknow, India
Mohini Gautam
Department of Social Work, Lucknow University, Lucknow, India
*Address all correspondence to: tridibeshtripathy@gmail.com
1. Introduction
As per the Hindu religious scripture, the Bhagwat Gita, Lord Krishna, a prominent Hindu god had an extremely turbulent life during his neonatal days[1]. The same struggle continues for all the current newborns or the birth cohort in India even today. The current neonatal mortality rate in India is 20 per 1000 live births as per SRS, 2020, and 24.9 as per NFHS 5[2, 3]. The high neonatal mortality is primarily through the early neonatal mortality rate (ENMR) that occurs in the first week of life. The current ENMR is 15 per 1000 live births. The late neonatal mortality rate that occurs in the rest 3 weeks is 5 per 1000 live births. This chapter focuses on aspects toward reducing this mortality rate. India has two approaches to reduce neonatal mortality, which is on the lines of the World Health Organization’s guidelines. These two approaches are home-based neonatal care (HBNC) practices and the facility-based neonatal care (FBNC) practices. The chapter focuses firstly on the HBNC approach[4].
Secondary data is the mainstay of the chapter. The chapter explores the gap between the current essential newborn care (EBNC) practices and HBNC practices. Through the gap exploration, the chapter finds out if there is a functional link between the two care approaches. Finally, the chapter suggests steps to be taken in future[4].
The current National Health Policy of India is viable till 2025, that is, 5 years before the SDG deadline. Therefore, it is envisaged that in next 2 years from now, the detail plans to introduce new and effective concepts in EBNC will be developed. The chapter also aspire that all the critical stakeholders of the sub national and national level will be involved to develop such detail plans. This will be a progressive step to fulfill the intricacies of the developed plan. Thereafter, India will be in a position to achieve the sustainable development goals (SDG) by 2030 and particularly those goals that are made toward reduction of neonatal, infant, and child mortality[5].
There are two aspects in the chapter. One is the community setting and the other is the hospital setting. The home-based newborn care (HBNC) is toward the community setting and the facility-based newborn care (FBNC) addresses the hospital setting. A child with a birth weight of less than 1800 grams has to be in the institutional care, whereas a child with birth weight more than 1800 grams can be saved through HBNC approaches[6].
The chapter is intended for people who are passionate about mother and child health (MCH). Among MCH, the chapter deals with the first month of life. It combines both the home-based newborn care (HBNC) and facility-based newborn care (FBNC) strategies in the most and densely populous country of the world, India. It deciphers out all the activities that can be done at home and facility levels to save the lives of all newborns. The chapter deals with the saving life or the need triad, especially for newborns. The three components of the triad are food, warmth, and security[6].
As all the HBNC-related activities are to be done at the grassroot level, the current chapter mentions the indicators through the work of the large network of outreach workers. These outreach workers are the Accredited Social Health Activists (ASHA) in India. These are daughters-in-law of the villages who work as volunteers. They are appointed by the local self-governance (LSG) to work on health-related issues in their own villages. They are attached to the public health system (PHS) by the LSGs. The PHS pays them honorariums for the various health services that they do at the grassroot level[6, 7].
As per the data of the Ministry of Health & Family Welfare (MOHFW) of Government of India, currently, there are 1 million ASHAs in India. They are spread over 18 Empowered Action Group (EAG) states or subnational levels. The National Health Mission was launched in 2005 in India in these 18 EAG states. As part of neonatal care package in India, home-based newborn care (HBNC) is one of the primary tasks of ASHAs. They are scheduled to visit homes of newborns to give need specific and time-based counseling at home level. Following such home visits, ASHAs are also supposed to refer the sick newborns, thus contributing to facility-based newborn care (FBNC) approaches. Among all the states in India, the most populous state in Northern India, the state of Uttar Pradesh has o.15 million ASHAs from among the total 1 million in India [6, 7].
Subsequently, the chapter explores the history of newborn care in India and reaches to the current situation of the two elements of neonatal care, which are FBNC and HBNC. A comparison is done among the two elements in terms of modalities such as services, roll out and indicators of achievements through large-scale health surveys in India. These surveys include critical indicators on newborn care. Through this process, the importance of the triad of neonatal care, which is “warmth,”, “food,” and “security” in both the elements/approaches of newborn care are discussed. It is significant to note that the approach and criteria used to assess these two elements through the neonatal triad vary significantly [6, 7, 8].
The institutional care includes newborns whose birth weight is less than or equal to 1.8 kilograms as these kids should be under the purview of institutional care as per the prescribed guidelines of the Government of India (GoI). The guidelines are developed as per the World Health Organization guidelines on neonatal care. Under institutional care, besides the birth weight criteria, the sick newborns are also included in the FBNC approach. The institutional care has a three-tier approach in the public health system (PHS) in India. The first tier is the urban or rural primary health centers (UPHC/RPHC) that covers 30,000 to 40,000 population on an average. Here, the newborn care corners (NBCC) are established. Next tier is the community health center (CHC) that covers 0.1 million population on an average. In this tier, the newborn stabilization unit (NBSU) is set up. In the topmost tier, the new born care unit (NBCU) is established at the district-level hospitals or other health units, such as first referral units (FRU) that cover about 1.5 million populations. So, it is seen that the first two tiers operate at the sub-district level and the topmost tier is at the district level [6, 8].
The highest neonatal therapeutic unit is the medical college hospitals or the research institutions/higher medical centers that have neonatal intensive care units (NICU). These cater to the cases such as defects at birth or sick and premature babies that are born during the viability period of 180 to 210 days. These newborns need special care that is given by staffs trained on neonatal care. The current annual birth cohort of India is 250 million. Hence, the newborn care becomes critical as it is the ladder to reduce not only neonatal mortality rate (NMR) but also the infant mortality rate (IMR) and the under 5 mortality rate (U5MR) as well finally impacting the overall child mortality (CM). This is how it addresses the human development index (HDI) and other social development indicators (SDI) of the country. Further, it is seen that the all-important multidimensional poverty index (MDPI) used internationally also focuses on the child mortality rate (CMR) as a crucial indicator. Hence, it is a fact that any road to reduction in CMR has to navigate through a reduction in NMR and especially the ENMR [8, 9, 10, 11].
The historical perspective of FBNC and HBNC programs in India needs to be understood to comprehend the current situation of India in terms of neonatal care. The following box shows this historical progress through a time line. In short, it is the mirror of neonatal care of India (Box 1) [6, 7, 8, 9, 10, 11].
1980—National neonatology forum (NNF) launched. The next step was taken after 12 years.
1992—Essential newborn care (ENC) launched through Child Survival and Safe Motherhood (CSSM) program. First time, maternal and child health was seen as a single component.
1994—In 26 districts of India, newborn care program (NCP) launched through CSSM. First time, experiments or interventions were done at subnational level.
1994—National program on facility-based newborn care (FBNC) launched. Subsequent to the subnational efforts, the national-level effort was initiated.
2000—National Newborn Week (NNW) initiated and to be celebrated from fifteenth to twenty-first November each year. A dedicated time was ascribed to the newborn care on the lines of WHO.
2003—District-level newborn care unit (NBU) set up in Purulia district, West Bengal. The FBNC effort was demonstrated successfully at the subnational level.
2011—Home-based newborn care (HBNC) guidelines launched. The newborn care moved from the facility level to the community level.
2013—Integrated action plan for prevention and control of pneumonia and diarrhea (IAPPD) launched. This framework was developed subsequent to the integrated management of neonatal and childhood illnesses (IMNCI) framework. The community level framework was C-IMNCI, and the facility level framework was F-IMNCI.
2013—RMNCH+A launched in the month of February. First time, the focus shifted to adolescents and reproductive Health. The framework provides the care and services to be provided in a 5*5 framework.
2014—India Newborn Action Plan launched. This comprehensive document combines both the FBNC and HBNC strategies.
2015—Neonatal mortality rate became the first step toward reduction of infant mortality rate. India adopted the launch of goal #3 of sustainable development goals (SDG) by United Nations. At the national level, alignment of the national strategy was done with the SDG since 2015. This was followed after the roll out of millennium development goals (MDG) that was operational during the 2000–2015 period.
Box 1
This chapter focuses on both the FBNC and HBNC, which are part of child health intervention (CHI) in India. It is imperative to trace the history of the child survival programs in India as the neonatal care is its base. In the beginning, the focus of child survival intervention was on the operation of immunization programs in India. In India in 1978 through the expanded program on immunization (EPI), the child survival interventions saw the light of the day. The section below has the details related to the entire gamut of development of newborn care in India [12].
A district newborn care program was initiated as part of CSSM in 26 selected districts in India almost 30 years ago in 1994. It led to the development of the national program on FBNC in the same year. The percolation of these efforts led to creations of newborn care corners (NBCC) at every point of childbirth across the nation. Subsequent to that, newborn stabilization units (NBSU) at First Referral Units (FRU) and Special Newborn Care Units (SNCU) at district hospitals came up [13].
Almost after 10 years of this event, in the year 2003, in Purulia district of the state of West Bengal in India, for the first time, it was demonstrated that institutional-level care of newborns is feasible at the district level. A triad level of care is detailed out in the FBNC guidelines of GOI. The first level is care at birth, the second level is care of normal newborn, and the third level is the care of sick newborn. The national-level experience of 11 years on newborn care led to the development of India Newborn Action Plan (INAP) in the year 2014. This GOI document details out the Standard Operating Procedures (SOP) of both the HBNC and FBNC components [8, 9, 12, 13, 14, 15, 16, 17].
As mentioned above, a child has to have a birth weight of at least 1800 grams to qualify for HBNC or stay at home. The HBNC approach is meaningless without the need and support of outreach health providers. Only places where the outreach worker visits the homes of pregnant women in their last trimester of pregnancy, those places can only ensure the benefit of the triad of warmth, food, and security [4, 6].
This paragraph details out the activities that need to be done to maintain the warmth of the child. The first activity is drying and wrapping the child immediately after birth. The second activity is to give skin-to-skin contact (STSC) by the mothers or any other caregiver. Here, the child gets the warmth of the mother or caregiver through the skin of the mother or caregiver. The point of caution is that the mother or caregiver should not have any cloth between the newborn and herself or himself. Both the child and the mother and caregiver should be covered from the top. The newborn should be kept in frog position between the breasts of the mother or caregiver with the mouth and nose sideways so that the child can respire or breathe freely. Humans learned the technique from the Kangaroos. The newborn of the Kangaroo lies in the pouch of the mother Kangaroo. The newborn derives warmth from the skin of the mother Kangaroo’s pouch. The newborn of the Kangaroo breastfeeds himself or herself while within the pouch [6, 7, 8].
This is how the newborn of the human or Kangaroo safely travels the first 28 days of life. It is rightly said and proved that the mother or the caregiver is the best warmer for the child leave aside the Radiant Warmer (RW) that are put up in institutions for neonatal care [8, 18].
The third activity to maintain warmth is through the delay of the bathing of the newborn at least for the ENMR period so that the Vernix Caseosa or the natural blanket that the newborn has on his or her skin is not removed. The ENMR period is for the first week of life. This process ensures that hypothermia in the newborn is prevented and taken care of [18].
The second component is the food component of newborn. The food component is attributed to the exclusive breastfeeding (EBF) practices of the child. The EBF period is during the 0–6 months of life. The EBF practice stipulates that only three things are allowed orally for the child in the first 6 months of life. These are oral rehydration solution (ORS) in case of neonatal diarrhea. The second thing is the oral vaccines (Polio and Rota), and the third thing is the prescribed medicines in case of a sickness in the newborn. The newborn should not be given anything orally till he or she attains 6 months of age other than these three things that are allowable orally. Water is also not allowed as the breast milk of the lactating mother has enough water for the child. The foremilk in both the breasts of the mother quenches the thirst of the newborn. Similarly, the hind milk in both the breasts of the mothers satiates the hunger of the newborn. So, the newborn drinks first and eats next unlike the adults [8, 18].
The third component addresses the security aspect of the child. Here, the activity is that the newborn should not be left alone in any case during the first month of life. The mother and the caregivers should be vigil and secure the newborn 24*7 [8, 18].
The KMC package bifurcates into STSC- and EBF-related activities. All the activities mentioned above can be done at household or home without any intervention or support from the skilled staff of the entire health system. That is why the package is called as HBNC package. In the first month of life that is highly sensitive, it should be ensured that there should not be a moving fan and no working air conditioner in the newborn’s room. All these activities further add to more loss of heat from the body of the newborn. The windows of the room are to be kept open to help the mother, caregiver, and the newborn to breathe freely. Every day as a routine, the newborn needs exposure to the morning sun for 15 minutes on an average. All such activities at home and institution lead to keeping the newborn warm, thus reducing the chances of mortality from hypothermia [6, 8, 18].
Next in line is the food component that addresses the indicators, such as early initiation of breastfeeding (EIBF) or Colostrum Feeding (CF). The former indicator holds good in the first 3 days of life, and the latter indicator holds good for the rest 27 days of life [8, 17].
4. Newborn care-related indicators in large-scale surveys in India
One of the large-scale surveys in India that captures newborn-related data is the National Family Health Survey (NFHS) that started in 1992–1993. It is done by the Ministry of Health & Family Welfare (MoHFW) of the Government of India (GOI), where the coordinating institution is the International Institute of Population Sciences located in Mumbai in the state of Maharashtra in India. It is an autonomous institution under the MoHFW of the GOI. Till the year 2023, there have been five rounds of this survey in India. Table 1 shows the newborn care-related indicators and their performance through the five rounds of these NFHS surveys [2, 3].
Survey Rounds & Year of survey
Newborn care-related indicators
Performance of the indicators in percentage
NFHS-I, 1992–1993
Children 0–1 month who are breastfeeding
Children under 3 years of age breastfed within 1 hour of birth
97.8
9.5
NFHS-2, 1998–1999
Children 0–3 months exclusively breastfed
Median duration of breast feeding in months
Children under 3 years of age breastfed within 1 hour of birth
55.2
25.4
16.0
NFHS-3, 2005–2006
Children under 3 years of age breastfed within 1 hour of birth
Children 0–5 months exclusively breastfed
Children born at home who were taken to a health facility for checkup within 24 hours of birth
23.4
46.4
0.3
NFHS-4, 2015–2016
Children born at home who were taken to a health facility for checkup within 24 hours of birth
Children who received a health check after birth from a doctor/nurse/LHV/ANM/Midwife/other health personnel within 2 days of birth
Children under 3 years of age breastfed within 1 hour of birth
Children under 6 months of age exclusively breastfed
2.5
27.2
41.6
54.9
NFHS-5, 2019–2021
Neonatal mortality rate
Children under 3 years breastfed within 1 hour of birth
Children under 6 months of age exclusively breastfed
24.9 (Per 1000 Live births). This number is an absolute number and not in percentage.
The other sources of data related to newborns, which are live births, stillbirths, and neonatal mortality, are given by the sample registration system (SRS) in India. The SRS was piloted in 1964–1965, and the system became fully operational in 1969–1970. Prior to SRS, the civil registration system (CRS) that included registration of births and deaths was operational on a voluntary basis after independence in 1947. The CRS was not uniform statistically as there were cases of under-registration and suboptimal coverage. In order to streamline the CRS-related activities, the registration of Births & Deaths Act, 1969 was enacted by the Indian parliament. To further strengthen and streamline the statistical data in India, the SRS was started as an alternative to the CRS. Currently, both the CRS and SRS co-exist [3, 9, 10, 11].
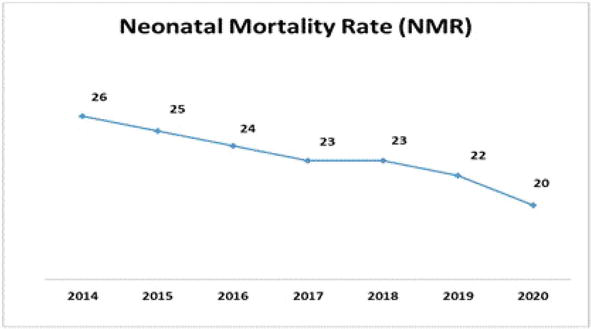
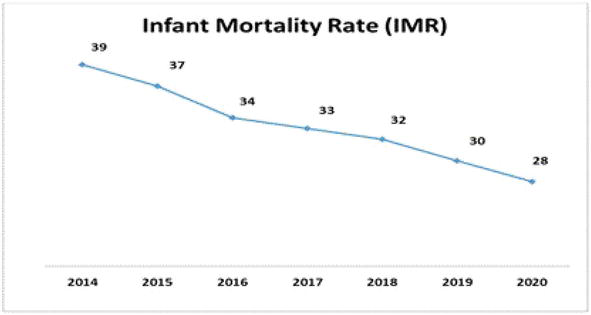
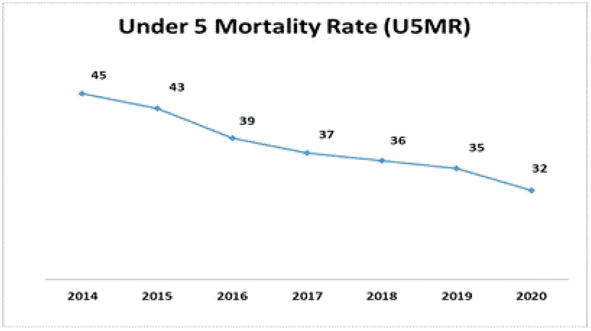
The following figures show SRS data related to child mortality, where it can be inferred that reduction in neonatal mortality rate (NMR) will eventually lead to reduction in infant mortality rate (IMR) and under 5 mortality rate (U5 MR). A slow reduction of NMR has led to slow reduction in both IMR and U5MR [3].
From the three figures, it can be seen that from 2014 to 2020, only a six-point reduction in NMR led to an 11-point reduction in IMR and 13-point reduction in U5 MR. This means a point reduction in NMR leads to almost two-point reduction in IMR and slightly more than double reduction in U5 MR. The inferred reduction ratio formula in the child mortality rates in India from 2014 to 2020 is NMR: IMR: U5MR is 6:11:13 or 1:1.8; 2.1 [3].
This is where the approach of FBNC and HBNC is critical as these approaches reduce the early neonatal mortality rate (ENMR), which takes into account the deaths in first week of life or in the 0–6 days of life. The period from 7 to 28 days falls under late neonatal mortality rate (LNMR). Currently, in India, the NMR is 20 per 1000 live births, the ENMR is 15 per 1000 live births, and the LNMR is 5 per 1000 live births. Hence, the complete focus should be on the first 7 days of life so that 15/20*100 = 75% of neonatal deaths are prevented. It is here that the neonatal triad along with the proven child survival interventions, such as immunizations, has a big role to play in reduction of NMR in India. The concept of deaths of newborns in India in the first 7 days of life has been discussed in the chapter in another section. Similarly, the current immunization for newborn is also discussed in the chapter in another section given below (Figures 1–3) [3].
Figure 1.
NMR in India [3]—Chart by the lead author.
Figure 2.
IMR in India (source-SRS, 2020)[3]—Chart by the lead author.
Figure 3.
U5 MR in India (SRS, 2020) [3]—Chart by the lead author.
In India, currently, the campaign regarding immunization is “5 years, 7 times and not to drop a single time.” This means till 5 years of age, the child has to attend the vaccination centers seven times, where the vaccinator will vaccinate the child as per prescribed immunization schedule. Table 2 gives the details of the current immunization schedule in India. The current article focuses on the immunization of newborns that addresses the prevention aspects of newborns [12].
MR-B, JE-B, DPT-1, vitamin-A-2nd to 6th dose at every 6-month interval
At 5–6 years (seventh time)
DPT-2
For Pregnant Women
Td-1 and Td-2 at an interval of 3 months between the two doses. Td-B one dose given to the mother if there is a gap of less than 3 years between two pregnancies.
Table 2.
Routine immunization schedule of India, 2023 [12, 14].
Pentavalent stands for a combination of five vaccines such as Diphtheria, Pertussis, Tetanus, Hepatitis B, and Haemophilus Influenzae type B (Hib).
OPV stands for Oral Polio Vaccine.
The acronym “fipv” stands for fractional inactivated polio vaccine.
Rota vaccine is given for diarrhea.
PCV stands for Pneumococcal Conjugate Vaccine.
MR stands for Measles & Rubella.
JE stands for Japanese Encephalitis that is given to children in selected states of Uttar Pradesh, Andhra Pradesh, Bihar, and Telangana.
DPT stands for Diphtheria, Pertussis and Tetanus.
Td stands for Tetanus and a small diphtheria component.
B stands for booster dose.
As seen from the above table, at birth, the child is vaccinated with BCG to prevent from tuberculosis, hepatitis B to prevent from serum hepatitis, and the zero dose for prevention from poliomyelitis. With this, the neonatal stage of the vaccination schedule finishes for the child. Hence, it is inferred that the newborn is prevented from tuberculosis, serum hepatitis, and poliomyelitis through three different vaccinations in the first month of life [12, 14, 17].
The protection, prevention, and treatment (PPT) model is adopted to deal with neonatal care. The following table details out the model. It is to be noted that protection component comes only once in a lifetime for the newborn. These are the Early Initiation of Breast Feeding (EIBF), which is commonly known as colostrum feeding that lasts for only 3 days after birth followed by the exclusive breast feeding (EBF) that lasts for 4–28 days for the newborn. This is the “food” component of the newborn [17].
Besides immunization, the other prevention-related activities of the newborn are drying, wiping, and wrapping the newborn after birth so that the warmth is maintained. The other activities, such as not bathing the newborn for 7 days, providing Skin to Skin Care (STSC) as a part of the Kangaroo Mother Care (KMC), not using air conditioner or fans in the newborn’s room and showing the morning sun to the newborn for 15 minutes also maintains the warmth of the baby. These activities are preventive activities for the newborn to prevent him/her from hypothermia [18].
Keeping a constant vigil on the newborn addresses the security component of the newborn triad. This is also a preventive activity for the newborn [8].
In case of any danger signs in the newborn, the newborn should be referred for treatment to a center, where sick newborn care unit exists or to a higher level of health care, where neonatal intensive care unit is functional. This addresses the treatment part of the newborn. Table 3 relates to the PPT framework [8].
Protection
Prevention
Treatment
The first protective activity is “Colostrum Feeding” which is technically known as Initiation of Breast Feeding that should be given ideally within 1 hour of birth.
The second protective activity is Exclusive Breastfeeding that should be done from 0 to 6 months of age for every child. The orally allowed substances for the newborn during this period are oral vaccines such as Polio & Rota, Oral Rehydration Solution (ORS) if the newborn suffers from diarrhea or dehydration and prescribed medicines if the newborn falls sick.
Hand washing with soap before 7 critical action points. These are before preparing food for the child, after cleaning the child’s toilet, after household chores, before eating, before serving food and before feeding the child.
Clean and potable drinking water for the mother, child, and clean air to breathe in both indoor &and outdoor.
Use of functional and clean toilets by all the household members, masks for members of the household having respiratory issues, vaccines such as OPV-Zero dose, Hepatitis B and BCG,
Therapeutic measures such as Cotrimoxazole prophylaxis for HIV infected and exposed newborns
Improved & timely care seeking & referral of sick newborns.
Case management of sick newborns at health facility/institutions & community/grassroot level
Cotrimoxazole for not severe Acute Respiratory Infection (ARI) cases, amoxicillin for severe ARI cases
Oxygen for ARI in newborn in health facilities
ORS but no Zinc supplement for newborn having diarrhea as Zinc is not given to 0–2-month-old child.
Continued feeding including breastfeeding for Young Children & only EBF for newborns.
The following section deals with the major killers of children under 5 years of age, where the neonatal deaths contribute to 57.9% of all deaths and the rest is for the postnatal stage. Among the three diseases, such as tetanus, diarrhea, and pneumonia, there are two major killers, which continue in the postnatal period as well. These two are diarrhea and pneumonia that are a threat for children till 5 years of age. That leaves us only with tetanus that is a potential threat to the newborn. Among newborns, diarrhea contributes to 0.4% of all deaths and pneumonia contributes to 3%. The rest all are conditions that are a danger to the newborn. The contexts of these two major killers are mentioned in the above PPT framework through the mention of treatment of pneumonia and diarrhea. The causes of U5 deaths in global level apply to India, as well as these cohort studies are done on a large scale and over a period of time [17, 19].
8. Neonatal mortality & multidimensional poverty index (MPI)
The global MPI includes education, health, and standard of living as the three dimensions to measure poverty. Unlike the previous methods that included income and consumption as the indicators. In the MPI, there are three dimensions and 10 indicators. Each of the dimensions has one-third weightage. The details of the dimension and the related indicators are given below as per the weightage [10].
The first is the education dimension. Under this dimension, there are two indicators. These are “Years of Schooling” and “Child Enrollment.” Each of these indicators has 1/6 weightage. When we sum up 1/6 + 1/6, we get 1/3 [10].
The second is the health dimension. The indicators under this dimension are “child mortality” and “nutrition.” Each of the two indicators has 1/6 weightage. Thus, on adding them, we get 2/6 or 1/3 [10].
Under the third dimension comes the standard of living. In this dimension, there are six indicators. These indicators are “electricity,” “flooring,” “drinking water,” “sanitation,” “cooking Fuel,” and “assets.” Each of these indicators has 1/18 weightage. On adding the weightage of each of these indicators, we get 6/18 or 1/3 [10].
Hence, each dimension through their related indicators contributes to one third of the poverty measure scale. The total poverty is represented as 1 adding 1/3 + 1/3 + 1/3 = 3/3 = 1 [10].
The index cites that a person/household will be categorized as multi-dimensionally poor when deprived in one third or more or 33% or more of the weighted all the 10 indicators of the three dimensions [10].
In case, the deprivation is half or more of the weighted indicators, these households are clubbed under extreme multidimensional poverty. It should be noted that the MPI ranges from “0” to “1,” where higher values mean higher level of poverty [10].
Here, we can see that one third of the weightage revolves around child mortality. The poor households need support from the public health system through the outreach and in-reach platforms so that they can save their newborns, which, in turn, will help reduce infant mortality and finally impact U5 mortality. Through reduction in these three stages of neonant, infant, and U5, we can reduce child mortality. Hence, poverty is rightly seen as a state of health in epidemiology and child mortality as an indicator of social development [9, 10, 11, 14].
The term “growth” means increase in the physical size of the body that we measure in terms of system international (SI) units, such as kilograms and centimeters. “Development” means increase in skill and function. These two are termed together as the child grows and develops as a whole. These two terms not only talk about physical aspects but also include intellectual, emotional, and social aspects of newborns. Data related to growth and development includes a comprehensive and sensitive indicator specific to child health that starts with the newborn health before and after birth [20, 21].
The growth chart tracks the growth and development through weight as the numerator and age as the denominator. Here, weight is the dependent variable, and age is the independent variable. A newborn usually doubles its birth weight by 5 months and trebles it by the end of the first year. For example, a newborn with 2.5 kilograms at birth will be 5 kilograms by 5 months of age, thus gaining 500 grams per month. Among these 5 months, the first month is the most critical as the newborn has to gain 500 grams by the end of neonatal stage. This is only possible if the triad of warmth, food, and security are adhered with as per standards [20, 21].
Similarly, the height/length of newborn is 50 cm, and it should be 75 cm by the end of the first year of life. So every month, the newborn is expected to gain 2 cm. Here again, the gain of 2 cm in the first month is most critical. If these two indicators are taken care of, the crossing over of chest and head circumferences takes place in the infancy stage. All these growths and development-related indicators are achievable only if the food component of the newborn is taken care of. The following section deals with the care protocol component of newborns [20, 21, 22].
Government of India’s Ministry of Health & Family Welfare developed a document titled “National Patient Safety Implementation framework for the period of 2018–2025 aligning the document with the end line of the current National Health Policy (NHP).” The patient safety is a fundamental element of public health care. The document defines the concept “as the freedom for a patient from unnecessary harm or potential harm associated with provision of health care” [23].
For the safety of the newborns, there are provisions and checks against issues such as inadvertent mix-up of babies at birth and abduction. The health care system aims to prevent, detect, and manage human and operational errors. To minimize these errors, the health care staff is trained accordingly so that they can counsel parents. Simultaneously, they will be able to provide emotional support to parents. Both the counseling and emotional support approaches lead to the safety and development of neonates. The trained staffs can ably and closely monitor each newborn baby’s condition and respond swiftly to any concerns or emerging issues [23].
Studies observed that the professional midwives trained on Midwife Led Continuity of Care (MLCC) as per the care guidelines that are regulated to international standards can provide better care. Studies show that when the MLCC trained staff supports mothers of newborns, there are 16% less likely chances that the mothers will lose their babies. In addition, the women supported by the MLCC trained staff experience 24% less likely chance to have preterm birth [24].
The section below discusses the importance of food component of the article, which is early initiation of breastfeeding (EIBF) and exclusive breastfeeding (EBF). These two indicators hold good during the first month of life [25].
11. About human Milk
According to the Lancet “human breast milk is a perfectly adapted nutritional supply for the infant. It is probably the most specific personalized medicine that the infant receives at a time when gene expression is being fine-tuned for life” [25].
The importance of EBF can be gauged by the fact that the levels of myo-inositol are high in the first 2 weeks of breastfeeding, and this helps in the wiring of the brain that lays foundation for cognitive development [26].
In order to ensure quality and quantity (Q&Q) of the breast milk, the study advises lactating mothers to have whole grain cereals and seeds as the bran of these foods contains a precursor of inositol called as phytic acid. Almonds, peas, and cantaloupes are foods to be consumed by lactating mothers as these foods are rich sources of inositol [26].
Another study points out that the human milk has an essential nutrient called Docosa Hexanoic Acid (DHA), and Omega-3 fatty acid helps in brain development. The study adds that a severe and fatal gastrointestinal condition called necrotizing enterocolitis (NEC) is prevented by breast milk and probiotics. The intestines of premature babies do not produce enough interleukin (IL) number 22 that protects from microbial infections [27].
12. Literature review
As already discussed above, lower-level health units are the first point of contact for the newborns. A meta-analysis of studies across 44 countries suggests strengthening of these lower-level health units as the main strategy toward reducing neonatal mortality. These units have high caseloads as these are the first point of contacts for the families of newborns. The study concludes on the note that strengthening of such units can yield reduction in mortality rate of newborns [13].
The institutionalized approach comes under the domain of facility-based newborn care (FBNC) that refers to 24*7 services provided by skilled and trained personnel at health facilities. In India at the national level, FBNC started in 1960s in few teaching hospitals or medical colleges. After 40 years, during 1990–2000, Essential Newborn Care (EBNC) that includes activities such as breastfeeding, warmth, and hygiene) was initiated as a strategy. Following this strategy, at the institutional levels newborn care-related equipment such as radiant warmers, resuscitation equipment, weighing scale, and phototherapy units were procured and used. Automatically, training to use these equipment became a regular activity of the FBNC strategy [28, 29, 30, 31].
From the national level, efforts were also seen at the subnational levels. In this context, a study in the state of Karnataka showed that research tools, such as supervisory and monitoring checklists, improve the quality of HBNC services. This is a critical area that the current article deals with [32].
Moving further, another study found that FBNC has a component duo called as essential newborn care (EBNC) and sick newborn care (SBNC). The Government of India (GOI) has devised the FBNC guidelines that mention about three levels of newborn care. The first level is at birth, the second level is at the care of normal newborns, and the third level is at the care of sick newborns. These three levels were to be dealt and made operational at the district-level institutional facilities [33].
Like the state of Karnataka, the state of Uttar Pradesh also had a study that elicited the key differences between the FBNC and HBNC. The study explored that use of Ante Natal Care (ANC) and skilled attendance (SA) at the delivery points were strongly associated with Clean Cord Care (CCC) & early initiation of breastfeeding (EIBF). However, the study deduced that the association was not strong with thermal care. Further, the study mentions that in order to maintain thermal care, a symbiotic relationship between HBNC & FBNC is essential [11, 29, 30, 31, 34, 35].
As mentioned above, during the 1990–2000 period in India, essential newborn care activities such as breastfeeding, warmth, and hygiene were initiated, conceptualized and put in place at a regular basis. Following this sustained effort, the triad of warmth, food, and security became the triangle of HBNC [36].
A second study in the state of Uttar Pradesh, which is the most populous state of India on HBNC in 2014, brought out the fact that none of the mothers of newborns had adequate knowledge, as well as awareness on the provisions of HBNC. These provisions were for home visits by the ASHAs, and it was observed that the number of home visits by ASHAs to the homes of newborns decreases as the age of the newborn child increases [34].
A study done in 2020 focuses on the dedication of the front line workers (FLWs). The study cites that HBNC is effective in reducing NMR and IMR when delivered by dedicated front line worker (FLW). These are seen not only in community settings but also in institutional settings or newborn care facilities with high rates of facility/institutional births per month/year [29].
Another study threw a perspective on HBNC that deciphers that upscaling of Home-based newborn care (HBNC) needs the support through identification of various limiting factors and effective upscaling in order to enable HBNC for reduction of neonatal mortality (NM) [30].
A 2009 study, which is the third study for the state of Uttar Pradesh in this chapter, reflected that in the parts of Western UP factors, such as awareness and demand for HBNC, were low not only among the mothers but also the community-based service providers, such as ASHAs. The study also mentioned about existing gaps in implementation and roll out of the HBNC strategy [11, 31, 34, 35, 37].
A study also mentions about the obstacles in newborn care, especially the HBNC. The elucidated obstacle was the practice of prelacteal feeding in newborn child. The time limit for prelacteals is the 0–6 days of life. It is to be reinforced that prelacteal feeding (PLF) of the newborns should not be practiced at any cost, and especially it is applicable for the low birth weight (LBW) babies. These LBW babies have birth weight less than 2.5 kilograms. The poor practice of prelacteals feeding (PLF) leads to hypothermia or loss of temperature in the newborn child. The condition of hypothermia leads or aids in infections [18, 31, 34].
The chapter is well served if it mentions studies that deal about causes/determinants of deaths in newborn child out of which infection category leads among all the causes. The section below deals with the fact that occurs if the poor practices, such as pre (0–6 days of life) and post (after 6th day of life) lacteals are not done during the first 28 days of life [11, 35, 37, 38, 39].
The current neonatal mortality rate (NMR) in India is 20 per 1000 live births. Similarly, there are multiple benefits of EIBF as well. It reduces the maternal mortality through easing the placental delivery, and thereby the chances of postpartum hemorrhage (PPH) are reduced. Poor practices, such as prelacteal feeding (PLF), happen when unfortunately, maternal mortality (MM) takes place [3, 8].
Another poor practice is the discarding of first breast milk by the lactating mothers. This practice occurs when there is less secretion of breast milk. The less or no secretion of breast milk happens as the newborn child is not put to the breast of the mother, or the EIBF indicator is not adhered to. Communities fall in the trap of these poor religious and cultural practices, while falsely assuming that such practices will help in enhancing the milk secretion in the lactating mothers. The criticality of Colostrum Feeding (CF) or the EIBF indicator is felt when the Maternal Mortality Rate and Ratio (MMR) of India is examined, analyzed and contextualized in the current circumstances at the national and subnational level. Here, it is significant to note that the MM rate in India is 6.0, and the MM ratio is 97 as per the SRS of India. Further, the SRS also mentions that the life time risk (LTR) of a mother in India is 0.3%, which means in probability, out 100 chances, there are 30 chances that the pregnant lady might have a maternal death, assuming that the risk is uniformly distributed along the entire reproductive life of a woman in the reproductive age group of 15–49 years. This high mortality, risk factors, and high death probability can be drastically reduced with the proven and time-tested strategies, such as promotion of EIBF in India and global level. The adoption of EIBF strategy also ensures removal of the two barriers in newborn care [31, 39].
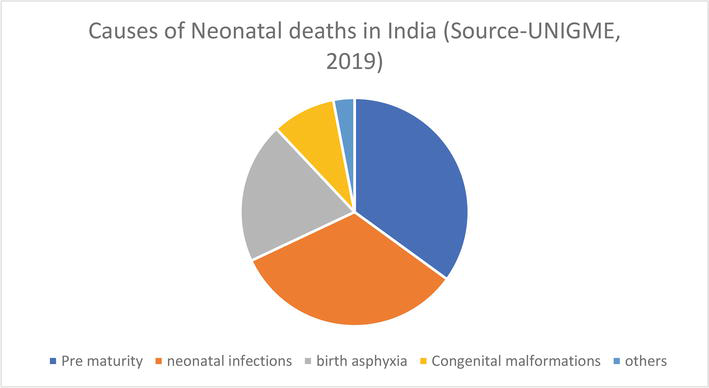
The figure given below is regarding the causes of these neonatal deaths. The figure shows that prematurity is the leading cause among all the categories. In this category, the low birth weight (LBW) babies are included, and the current chapter details out the two barriers/obstacles of the newborns where such LBW babies do not have the strength to suck the breast milk of the lactating mother. The second in line is the neonatal infection (NI) and here the infection prevails because of poor thermal care that leads to hypothermia. It is also critical to note that EIBF is an active component of thermal care as it comes under the domain of Kangaroo Mother Care (KMC). It is proved beyond doubt that timely referrals by FLWs, or family members will definitely help in processes to reduce other causes of neonatal deaths, such as infections and asphyxia. Both FBNC and HBNC roll out have substantiated that hypothermia is a significant contributing factor for such causes that are attributed to neonatal deaths. Hence, the relevance, importance, and timely contextualization of the contents of the current book chapter is clearly in focus in India (Figure 4) [39, 41].
Figure 4.
Causes of neonatal deaths in India [40]—Pie chart by the Lead author.
A newborn is a boy or girl in the first 4 weeks of life or in the 0–28 days category. India introduced the National Rural Health Mission in 2005. Since the initiation of NRHM across 18 Empowered Action Group (EAG) states, the newborn child care took a paradigm shift. This was because the focus of newborn child care had moved from FBNC to a healthy mix of HBNC and FBNC strategies. The WHO bulletin published in the year 2012 states that India’s home-based newborn care (HBNC) model launched in 2011 can be touted as a global policy, and it has percolated to many nations as we can see in 2023 or 12 years after its introduction. The efforts on HBNC were initiated in India in Gadchiroli region of the state of Maharashtra. Here, an effort of 20 years has demonstrated and proved that there was 62% reduction in neonatal mortality through the simple strategy of multiple home visits by community level workers (CLW) [6, 38].
These efforts by the CLWs led to the conceptualization of the NRHM on a large scale at the national level in India in the year 2005. In the strategy of NRHM for newborn care, the FLWs, such as ASHAs, are required to do six home visits to the homes of the new mothers and newborns in case of an institutional delivery and seven home visits in case of a home delivery. Taking the birthday as the “0” day, the visit days for the institutional delivery are on the 3rd, 7th, 14th, 21st,28th, and 42nd days after the delivery. Similarly, the visit days for the home delivery are on the 1st, 3rd, 7th, 14th, 21st, 28th, and 42nd days after birth [6, 8].
When we analyze the pattern of mortality of the newborns, the data regarding weeks showed that 72.9% die in the 0–6-day period. Whereas a mere 13.5% die in the 2nd, 3rd, and 4th weeks after delivery. The neonatal mortality data in percentage per day shows a decreasing trend as the days pass by. There is a difference of 29.5% among o day and day 1 or in just 24 hours. There is an increasing trend between day 1 and day 2. The difference between these 2 days is 2.7%. Thereafter from the 3rd day, the trend shows a continuous decrease. Day wise, the data shows that 36.9% die on day 0, 7.4% on day 1, 10.1% on day 2, 6.6% on day 3, 5.1% on day 4, 3.4% on day 5, and 3.5% on day 6 [42, 43].
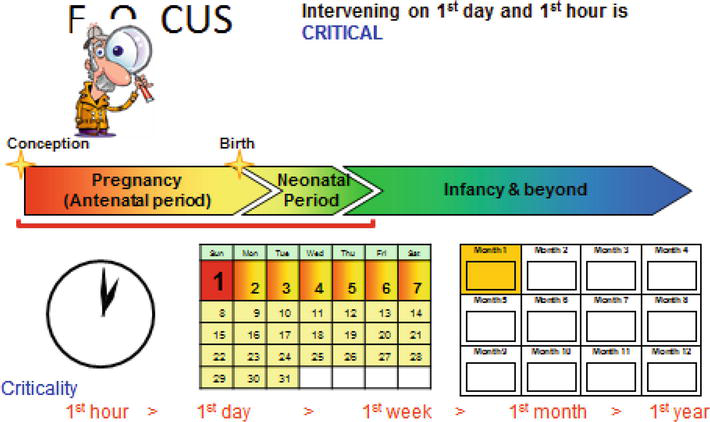
Hence, the abovementioned data proves that the first week of life is extremely critical and crucial for the newborn to be visited by the ASHA at the household level. The current chapter focuses on the HBNC model primarily, which is described in detail in the India Newborn Action Plan (INAP) of 2014 of GOI. To augment the home visits by ASHAs, incentivized home-based newborn care program was launched in the year 2011. As on 2023, all the ASHAs of India had been trained as per the training modules of National Health System Resource Centre (NHSRC) of GOI to improve the quality of newborn care services. The figure given below depicts that in the life of an infant, the 1st year of life is critical. In the first year of life, the 1st month of life is more critical. In the first month of life, the 1st week of life is most critical. In the first week of life, the 1st day is utmost critical. In the first day of life, the 1st hour of life is exponentially critical. The triad of activities related to newborn care cannot be missed in the first hour of life or in the first hour after birth as it is known as the golden hour, and it comes once in a life time of the child and does not return again in the life time of the child. Hence, it is re-emphasized that intervening on 1st day and 1st hour is a must [36, 42, 43].
Poor practices, such as prelacteal feed (PLF) and discarding of milk, further increase the risk of the life of the newborn. A related event is that 40% of all stillbirths, and neonatal deaths occur within first 48 hours of life. Further, analysis reflects that about 3/4th of the total neonatal deaths occur in the first week of life or in the 0–6 days period. As mentioned above, 37% of these deaths occur within first 24 hours or on the first day of life. This period is not only critical for NMR but also MMR. During this period, half or 50% of all maternal deaths also takes place. These deaths show the contribution of the poor practices, such as giving prelacteal feeds (PLF) to the newborns. Discarding the first breast milk is done by the lactating mothers who falsely believe that it leads to enhancement of milk secretion. The belief is strong as they the offering is attributed as a religious and cultural practice or taboo [11, 36, 42, 43].
Among the HBNC-related activities, maintaining the warmth component is of utmost importance. Every newborn baby is homoeothermic at birth. From among these newborns, the low birth weight (LBW) babies have decreased thermal insulation as they have reduced amount of brown fat that is situated below the white fat of the skin. The science of matter, physics, tells us that heat loss in the newborn is either due to phenomena such as evaporation, conduction, or convection. Evaporation is through amniotic fluid by surface. Conduction is through touch with cold object or cold skin or body of the caregiver or mother. Convection is through fan or window, where the heavier cold air replaces the lighter warm air. The indicator for the thermal comfort of the newborn child is his or her warm and pink feet. The healthy behaviors such as delayed bathing, delayed weighing, and kangarooing in case of low birth weight (LBW) babies contribute toward maintaining the warmth of the newborn baby. These practices are to be done at both home and institutional level [8, 18, 36].
Moving ahead, maintaining three other components, such as clean airway, breathing and temperature, is also essential in the newborn just like an adult to survive. Above all, the warmth component is of prime importance for low birth weight (LBW) babies because if the LBW babies are not kept warmth, the LBW babies cannot feed and will eventually not gain body weight in the early neonatal period or in the 0–6-day period. To help LBW babies gain weight, timely home visits by ASHAs are not to be missed. The strategy encourages the family members to ensure proper care of the LBW babies there by leading to healthy weight gain in these susceptible LBW babies. It is seen that low-weight neonates are most prone to noncommunicable diseases (NCD) such as diabetes, hypertension, and heart diseases in later life [2, 3, 4, 8, 11, 12, 15, 29, 31, 32, 33, 34, 35, 44].
13. Neonatal deaths and the modalities
A close look at the analytical epidemiology of deaths of newborns elicits a triad of causes. These are preterm birth complications (PBC) followed by infections. The third cause is intrapartum period related or during delivery. Analysis of the rest of the causes of death shows that there is equal weightage given to congenital anomalies and the “others” category (Figure 5) [19, 42, 43].
Figure 5.
Critical times of the infancy stage [42, 43]—PowerPoint by the lead author.
The figure given above reiterates the importance of the timing of home visits by ASHAs (Accredited Social Health Activists) in HBNC strategy newborn care. The figure emphasizes that the ASHAs need to plan for the home visits of the newborns. In India, An ASHA covers 1000 population on an average. Hence, at any point of time of the year, there will be 10–12 newborns in her area taking into account the ENMR, LNMR, IMR, abortions and stillbirths (SB) [6, 8].
As mentioned above, when we look at the life risk of the neonate, infant & the U5, we find that among the 1st 5 years of life, 1st year of life is critical. Out of the first 12 months, 1st month is critical. Out of the 1st 4 weeks, the 1st week is critical. Out of the 1st 7 days, the 1st day is critical. Out of the 1st 24 hours, the 1st hour is critical. This 1st at all these levels have a direct relationship with the timing of deaths of the newborns [36, 42, 43].
In India, when we analyze the deaths in weeks, we find that 3/4th of the total neonatal deaths occur in the 1st week of life as discussed above. Among the 1st 7 days of life, the 1st day accounts for more than 1/3rd or 33% as 36.9% of the total neonatal deaths. In other words, the first day deaths are the most critical among the deaths in the entire neonatal period in India at the national level [36, 42, 43].
Further, in another article on neonatal deaths at global level, the lead author M J Shankar deciphers that in the developing countries, the first week of life (0–6 day) period accounts for 77.7% of all neonatal deaths. Further, analysis reflects that 11.1% die in the 2nd week, whereas 11.2% die in 3rd week to 4th week [36, 42, 43].
Epidemiologically, when we the see the deaths in proportions, we find the following proportions of neonatal deaths from among all the neonatal deaths. The proportion in the 1st week of life is given for each of the days of the 1st week in the developing countries [36, 42, 43].
The proportion is 44.4% on day 0. The proportion is 10.1% on day 1. The proportion is 8.3% on day 2. The proportion is 5.8% on day 3. The proportion is 3.6% on day 4. The proportion is 2.7% for days 5 & 6 [36, 42, 43].
Similarly, the same proportion of deaths in India per each day of the 1st week of life shows that on 0 day, the proportion of deaths is 36.9%. The proportion of deaths on 1st day is 7.4%. The proportion of deaths on 2nd day is 10.1%. The proportion of deaths on 3rd day is 6.6%. The proportion of deaths on 4th day is 5.1%. The proportion of deaths on 5th day is 3.4%. The proportion of deaths on 6th day is 3.6% [36, 42, 43].
After seeing the proportion in days, let us see the proportion in weeks. The data reflects that the proportion of deaths in the 1st week is 72.9%. The proportion of deaths in the 2nd to 4th week is 13.5% for each of the 3 weeks [36, 42, 43].
HBNC guidelines are not only regarding newborn care but also on maternal care. It is a package of maternal and child health (MCH0). The guidelines include the care of the mother during pregnancy till 42 days after delivery. To ensure effectiveness of HBNC, during the last trimester of pregnancy, the front line workers (FLWs), such as ASHAs, are expected to visit the homes of the would-be mothers. The discussions of the visits must include appropriate elements of HBNC and the related activities to be done by the household members so that the critical “newborn triad care” is taken care of. As discussed above these are “Warmth,”, “Food,” and “Security” [4, 8, 36].
During the home visits to the homes of would-be mothers during their last trimester, the FLW should reinforce on four basic activities. These are “wrapping” the newborn immediately after birth, drying the newborn immediately after birth, not bathing the newborn for 7 days after birth and finally giving Kangaroo Mother Care (KMC) to the newborn. All these four activities help maintain the warmth of the child [4, 8, 36].
The FLW should also mention two additional activities during her abovementioned home visit. The activities are giving only colostrums (EIBF) without any pre- and post-lacteals. These activities are to be done in the 0–6-day period. The next activity is exclusive breastfeeding (EBF) the child. Both these activities are toward addressing the food component of the newborn child [4, 8, 36].
Regarding the security aspect, keeping the umbilical cord clean without any application will help prevent Omphalitis. A 24*7 vigil or attending the newborn baby are the activities pointing toward the security needs of the newborn [4, 8, 36].
All the above sections dealt, in the chapter, hope that the objective of the proposed or discussed newborn care approaches is envisaged at a large scale in India. The following section mentions the identification of research gap in the chapter. Addressing this gap will help the country to get optimum output in neonatal care, its positive effect on neonatal care in India and the positive influence it will have in the development of the society and finally its influence on positive trends in framing of newborn friendly health policies in India [6, 41].
Thereafter, the chapter expects that a focused plan to augment and integrate HBNC and FBNC in neonatal health in India is made. It is feasible as it is not only cost effective but also feasible effective as it is done at family or household level without the support of a skilled health provider, such as a clinician/therapeutic provider. It is to be recalled that the HBNC component or the community-level strategy is achieved through the active support of an outreach worker of the public health system, such as the ASHA and the auxiliary nurse midwife (ANM) [3, 8, 11, 12, 15, 32, 40].
14. Identification of research gap
As in any study, the chapter also focuses on the “research gap” following the extensive literature review. The study identifies that outreach approaches of the health systems on EBNC package have not been actively integrated into the entire EBNC package in India. The grassroot level dispensaries of the public health systems work are the “outreach” related stakeholders. These “outreach” centers in fact work vertically, and there is no horizontal integration among the “in-reach” & “outreach” related stakeholders. The integration is especially poor at the community level. The all-important HBNC component is rolled out at this level. As discussed above, the community approaches through the HBNC package roll out have proved its credentials time & again. The credentials are not only in EBNC but also in the field of entire maternal and child health (MCH). Therefore, the research gap concludes that the potential of HBNC has not been actively and appropriately streamlined into the current programmatic interventions on MCH both at subnational and national level in India [12, 24, 28, 32, 33, 35, 37, 38, 39].
15. Conclusion
All the elements discussed in the chapter points to the efficacy of the newborn triad of warmth, food, and security. Reduction in NMR is the baseline. If this baseline is taken care of, reduction in IMR and U5MR will eventually happen. As a result, the CMR will reduce which will lead to socioeconomic development through reduction in extreme poverty-stricken families [9, 10, 35, 36].
The normative theory of developmental social policy (DSP) cites that health systems can sustain themselves in the long run. To sustain, health policy (HP) and the health care policy (HCP) paradigm must focus on saving early lives from premature death. Further, lives should be saved from illness, accidents, misery, and poverty. India is adopting the same path of DSP through the various effective and proven strategies on newborn care. It is significant to note that the efforts have percolated across the globe from India, especially on the HBNC strategy of the NHM [11, 45].
Acknowledgments
The lead author wants to acknowledge that Professor Shankar Das, a co-author, was the Ph.D. guide of the lead author at the Tata Institute of Social Sciences (TISS), Mumbai, India during 2011-2018.
Professor D.P.Singh was the teacher of the lead author at TISS, Mumbai during 1995-1997.
The lead author also acknowledges the contributions of all other co-authors.
All the figures given in the chapter have been made by the lead author using the data from the sources mentioned in the chapter against the figures.
Conflict of interest
There is no conflict of interest to write the chapter.
Financial Support
No financial support was received to write the chapter.
References
1.The Bhagwat Gita. A Scripture of Hindu Mythology. Gorakhpur, Uttar Pradesh, India: Gita Press; 2023
3.GOI, RGI, SRS, Ministry of Home. Statistical Report, 2020. GOI, Vital Statistics Division, RGI. New Delhi, India: Ministry of Home Affairs; 2022. Available from: http://censusindia.gov.in
5.UN, SDG. Goal #3. New York, United States: UN Head Quarters; 2015
6.NHM. GOI, MCH guidelines. New Delhi, India: NHM; 2007
7.GOI, NHSRC. Training Modules for ASHAs. New Delhi, India: NRHM; 2005
8.GOI, MOHFW. India Newborn Action Plan. New Delhi, India: GOI, MOHFW; 2014
9.GOI. Indian Public Health Standards. New Delhi, India: MOHFW; 2023
10.Alkire Sabina, Maria Emma Santos. Multidimensional Poverty Index, Oxford Poverty and Human Development Initiative. New York, US: UNDP; 2010
11.NHM. GOI, MCH guidelines. New Delhi, India: NHM; 2007
12.GOI, MOHFW. Routine Immunization of India. New Delhi, India: GOI, MOHFW; 2023
13.Neogi SB et al. Does facility based newborn care improve neonatal outcomes—A review of evidence. Indian Paediatrics. 2012;49(8):651-658
14.GOI, MOHFW. Intensified Mission Indradhanush, Child Health Division. New Delhi, India: GOI, MOHFW; 2023
15.Neogi SB et al. Inpatient care of small & sick newborns in health care facilities. Journal of Perinatology. 2016;36(s3):S18-S23
16.Sen A et al. Impact of a district level sick newborn care unit on neonatal mortality rate; 2 year follow up. Journal of Perinatology. 2009;29:150-155
17.GOI, MOHFW. IAPPD Guidelines. New Delhi, India: GOI, MOHFW; 2013
18.National Neonatology Forum teaching aids, new-born care. 2015. Available from: www.nnfi.org/index.php
19.Liu L et al. National, regional & state level all causes and cause specific U5 mortality in India in 2000-15, a systematic analysis with implications for the SDGs. The Lancet Global Health, Open Access. 2019;7(6):e721-e734. DOI: 10.1016/s2214-109x(19)30080-4
20.Park JE, Park K. Text Book of Preventive & Social Medicine. 11th ed. Jabalpur: M/s Banarasi Bhanot publishers; 1987
21.Singh M, Saini S. Conceptual Review of Preventive & Social Medicine. 2nd ed. Darya Ganj, New Delhi, India: CBS Publishers & Distributors Pvt. Ltd; 2020. ISBN-978-93-88725-84-2
25.Victoria C et al. Breast Feeding Series. London, UK: The Lancet; 2016. Available from: https://www.thelancet.com/series/breastfeeding
26.Biederer T. PNAS study, the importance of myo-inositol in breast milk for baby’s brain development. PNAS. 2023;120:e2221413120. Available from: www.metroamericas.com/en/noticias-2
27.Phillips S et al. Global View of Human Milk, GEHM Study. San Diego, CA, United States: PNAS, Neuroscience, University of California; 2021. Available from: www.southeastneo.com/wp-content/uploads/2021
28.Darnstadt GL et al. Neonatal Survival Series. The Lancet. 2006;367(9521):1541-1547
29.Rasaily R et al. Effect of home based newborn care on neonatal & infant mortality: A cluster randomized trial in India. BMJ Global Health. 2020;5:e000680
30.Dutta AK. Home based newborn care, how effective & feasible? Indian Paediatrics. 2009;46:835-840
31.Baqui AH et al. Newborn Care in Rural Uttar Pradesh. Indian Journal of Paediatrics. 2007;74:241-247
32.Spector JM et al. Improving quality of care in improving maternal & newborn health, prospective pilot study of the WHO safe child birth checklist program. PLoS One. 2012;7(5):e35151
33.Gould JB et al. Expansion of community based perinatal Care in California. Journal of Perinatology. 2002;22(8):630-640
34.Pathak PK et al. Study to assess the HBNC visit in rural areas of Lucnow: A cross-sectional study. Journal of Family Medicine & Primary Care. 2021;10(4):1673-1677
35.Blencowe H, Lee AC, Cousens S, et al. Preterm birth associated neuro developmental impairment estimates at regional and global level for 2010. Paediatric Research. 2013;74(Suppl. 1):17-34
36.Tripathy T et al. FBNC & Homoeopathy. Vol. 12. Issue 07. IJAR. July 2022. pp. 51-54. Print ISSN-2249-555X. 2022
37.Chaudhury K et al. Deman, awareness & implementation gap of HBNC in rural area of Meerut, UP. IOSR-JDMS. 2019;18(6):43-49
38.Bang AT, Bang RA, Reddy Hanimi M. Home-based neonatal care: Summary and applications of the field trial in rural Gadchiroli, India (1993 to 2003). Journal of Perinatology. 2005;25:S108-S122, Nature Publishing Group
42.Shankar MJ et al. When do newborns die? A systematic review of timing of overall & cause specific neonatal deaths in developing countries. Journal of Perinatology. 2016;36:S1-S11
43.Shankar MJ et al. State of newborn health in India. Journal of Perinatology. 2016;36(Suppl. 3):S3-S8
44.GOI. GOI, Ministry of H&FW, MCH Guidelines. New Delhi, India: GOI; 2015
45.Das S, Cottler LB. The health care system in India, chapter 8. In: Aspalter C, Pribadi KT, Gauld R, editors. Health Care Systems in Developing Countries in Asia. 1st ed. UK: Routledge; 2020. ISBN: 9780367594961