Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
A safe and effective neonatal building is an aspect of Neonatal Rescue Scheme (NRS) concept as described in the literature. Observable habitual practices leading to various neonatal outcomes at tropical LMIC settings point to adverse facility-based mortality contributions from poor nursery layouts. Sadly, the negative impacts of building deficiencies are not well-understood or empirically quantified as tailored to the limitations in resource-constrained tropical climate. Lack of helpful building features may exacerbate high morbidity owing to adverse issues such as poor infection control, evening fever syndrome (EFS), noise pollution, medication safety, intra-ward traffic, nursing fatigue, and parental services. A tropical LMIC setting has the disadvantages of relative poverty, infrastructural inadequacies, and adverse equatorial climatic conditions, necessitating design-specific requirements for safe neonatal care. This chapter is proposed to explore the constraints, concepts, and features as integrated in some NRS nurseries at different tropical regions of Nigeria, which function to mitigate the climate, poor infrastructure, and societal poverty against neonatal survival.
Department of Bioengineering, Imperial College London, United Kingdom
Mohammed B. Kawuwa
Department of Obstetrics and Gynaecology, University of Maiduguri, Nigeria
Amina L. Abubakar
Department of Obstetrics and Gynaecology, Kaduna State University, Nigeria
Stephen K. Obaro
Section of Pediatrics Infectious Disease, University of Nebraska Medical Center, Omaha, USA
*Address all correspondence to: h.amadi@imperial.ac.uk
1. Introduction
The low- and middle-income countries (LMICs) of the world, particularly in Africa, are riddled with so many disadvantages emanating from poverty and lack of basic infrastructure for effective neonatal care. The lack of these basic neonatal practice needs, in turn, exposes the neonate to unimaginable hardships and unsafe environments in their struggle for survival. Literature is dominated by research, discoveries, advances in practices, methodologies, and technologies showcasing neonatal care in high-income countries (HICs) of the world. The attractive technologies and highly successful neonatal outcomes at HICs are made possible by highly sustainable funding and infrastructure, which are readily available to practitioners at HICs, the very opposite of the situations at LMICs. Whenever a typical practitioner at an LMIC setting searches the literature for new ideas to better practice, swarms of articles of HIC technologies and ideas would dominate the horizon, compelling the practitioner to gravitate to these ideas as the best that could be used. LMIC practitioners very often forget that all successes at HICs are fundamentally made possible by the sustainable infrastructure that creates the conducive environments and climate which helps the technologies to thrive and produce attractive results. Consequently, the LMIC practitioners need to be articulative and consciously understand that a rush into the adoption of many of these HIC technologies and ideas without initiation of commensurate sustainable funding and infrastructure would always amount to neonatal practice suicide. We hypothesize that lack of conscious understanding and reaction to this very situation of impoverishment is the backdrop of the perpetual high neonatal mortality rate at most LMIC settings, including Nigeria.
The advantages created by the opportunity of simultaneously being a senior medical professional at a top HIC institution as well as a visiting consultant at many top LMIC hospitals have enabled this corresponding author to amass a vast amount of experience to respond to the disadvantages of the LMIC settings. Therefore, it is essential to note that this LMIC ugly situation can be intelligently divided into two segments, which must be recognized and treated with prioritization. Hence, if an LMIC setting must successfully adopt the HIC, then it is necessarily required to proceed as follows: (1) The LMIC setting must put in place a good quality and sustainable infrastructure like power, access road, and sustainable treatment funding that is tailored after those in HIC settings, after which (2) The LMIC facility could proceed to adopt the efficient new ideas and technologies tailored after those in HIC settings. The LMIC governments and their neonatal practitioners who are often drawn to the HIC high-tech, without prioritizing their infrastructural base, would always end up in unsustainable outcomes and the re-emergence of facility failures that were once thought to have been resolved. However, in situations where the government and in-country policy makers fail to understand these arguments, then the practitioners and local facility management must come to the rescue of the endangered neonate by adopting other strategies at their disposal. Hospital management may be unable to bypass the government to build sustainable grid electric supply, good access roads and highway network, and prosperous economy for neonatal carers. However, they are certainly capable of ingeniously creating facility buildings, and onsite harnessing and exploitation of nature as a response to the adverse neonatal effects of government failures. Better survival rate of neonates using alternative ingenious techniques which did not rely on standard government-led infrastructure have previously been demonstrated [1, 2, 3, 4].
Neonates at LMIC facilities are notably exposed to all kinds of unsafe situations that threaten them with immediate death or later life disabilities. Many of the health threats can be avoided by designing and adopting some possible facility building features. However, these features can only be conceptualized with a good understanding of what these neonatal unsafe situations really represent. Neonatal facility buildings are erroneously, not often regarded as one of the most sensitive neonatal equipment that must not be compromised. Therefore, these buildings have been designed and constructed without any reference to the deadly dangers and unsafe environment the nursery building would present to the neonates. The deadly mistake of this ignorance has exacerbated the negative impacts of morbidities that neonates would have to deal with, hence, making many of them to easily lose their battles for survival. A nursery building that incorporates adequate responses to neonatal adverse effects and conditions is termed a ‘functional building’. A nursery building that exacerbates the negative climatic, economic, and socio-cultural effects is a ‘dysfunctional building’. Therefore, a knowledgeably designed nursery building can mitigate the effects of adverse climate, technology and policy-failures, socio-cultural dispositions, carer poverty, and lack of essential social infrastructure.
This chapter will explore a few of the neonatal unsafe conditions as have been identified across the entire regions of Nigeria, and the implemented nursery building designs and features that have been used to mitigate their impacts on neonatal survival.
2. Building with intent to shield neonates against hyperthermia
Sub-Saharan Africa is notable for high sunlight intensity for almost every month of the year, with some regions recording outdoor temperatures higher than 46°C and spanning many hours of the day [5]. The consequent high indoor nursery temperature has, for many years, been responsible for misdiagnoses of the iatrogenic fever as a disease-process requiring antibiotic intervention, from which neonates have lost their lives [5]. However, this climate-induced evening fever syndrome (EFS) would normally wear-off much later in the night or with the relocation of the neonate to a cooler spot within the nursery space, and without the need of antibiotics as has been demonstrated in the literature [5, 6]. The deadly effects of EFS could be avoided if the choice of the site and positioning of the nursery apartment within the neonatal building complex is made with full evaluation of the predictable interactions and impacts of light rays as the sun rises from the eastern cardinal direction and sets at the western. The neglect or ignorance of EFS mitigation would lead to daily neonatal hyperthermia, complications from needlessly administered antibiotics, and neonatal thermal-shock from practices that attempt to rapidly force-down the body temperature, which could lead to death [7].
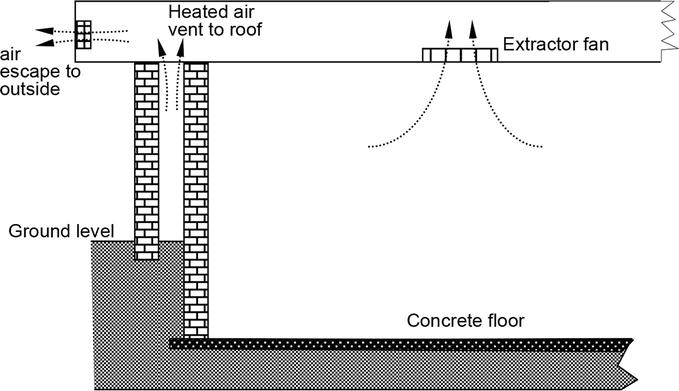
Unprotected sunrays interactions with nursery interiors have many other negative impacts on the workforce, including staff discomfort and tiredness. Since the neonates experiencing hyperthermia would not be left unattended, the nursing staff must expend extra labour in trying whatever possible to keep the neonates safe. This situation is made worse during occasions when many neonates are overpowered by EFS effects, simultaneously. Unfortunately, lack of adequate nursing manpower in a typical special care baby unit (SCBU) is an endemic LMIC situation [8]. Therefore, dysfunctional nursery apartments at LMICs, where there may not be sustainable luxuries of electric powered air-conditioning systems, create a wide variety of practice difficulties and unsafe environment for the neonate. Naturally cooled nursery environment at such high intensity sunny settings help to ensure conducive thermal tranquility for neonates and the staff who look after them. Therefore, features of ‘double-wall, air-lagged’ techniques, and SCBU-floor underground lowering, as described in the literature has been adopted in some recent SCBU buildings in Nigeria (Figure 1).
Figure 1.
Air-lagged double wall technique as described in Amadi et al. [5].
3. Building with intent to enhance low-cost facility lighting and power supply
Inadequate and erratic power supply has been blamed amongst other factors responsible for high mortality at LMIC health facilities [9]. The health facilities in Nigeria are notoriously crippled by incessant power blackouts, including at high vulnerability hospital segments such as the SCBU [10]. Hence, some useful methods of alternative or supplementary power provision have been suggested, including the use of solar panels and inverter technology [11]. The conventional technique of inverter power installation in Nigeria involves connection of the panel-battery-inverter assembly as a standby power supplier in the event of grid power failure. This technique has limitations that often create practice frustrations as has been observed across many Nigerian SCBUs applying this. Some centres have explained their frustrations for the lack of sustainability of this power option, including the high cost of frequent battery replacement. Other centres complained of the short lifespan of the standby inverter power supply after full charge, which could only support facility lighting and powering the essential neonatal machines at night for less than 3 h before the SCBU returned to utter blackout for the rest of the night. There are explainable technical reasons for this short lifespan, including inefficiency of the installation technique that are often applied. The separation of the duo of ‘facility lighting’ and ‘sockets powering’ into two independent systems when using renewable energy backup has previously been proposed [2]. The proposal demonstrated how the Neonatal Unit could be powered by two independent solar panel gangs, one supplying 12 V to its charge controllers and the other supplying 48 V, respectively. Therefore, nursery building design and construction must create adequate provision for the components that could be later installed for this purpose, such as various gangs of roof-mounted solar panels and rooftop wind breakers for panel protection (Figure 2).
Figure 2.
(A) Sideview Yobe NRS neonatal hubcentre complex (B) Part of rooftop – mothers’ dormitory segment – showing roof wind breaker parapet before solar panel installation.
3.1 Independent lighting system
Conventionally, the inverter power is typically wired into the existing nursery power distribution lines using ‘switchover gear’ controls via chosen fuse-lines. Using this technique, specific fuse-lines for power sockets and gangs of lighting points are selected to be supplied by the inverter. This measure is a power management technique to restrict the standby inverter power to the relevant sections of the nursery, where all the conventional high voltage outputs along the prioritized lines are enabled. Therefore, the inverter system is subjected to supply energy to all conventional light bulbs, some of which could be of high-power consumption ratings, such as 60–100 W, as often installed in a typical SCBU in Nigeria. It has been previously reported that the inverter system installed in this manner would readily get drained of its battery reserve in quick time, leading to automatic self ‘power off’. The use of low wattage bulbs, such as 5–12 W, had been tried but this did not yield much overall improvement. Also, illumination from the low wattage bulbs was described as insufficient in intensity for some aspects of clinical works, such as ‘neonatal line-setting’ in the night. Amadi and Abubakar [2] demonstrated their ‘polite-light-bank (PLB)’ system, which was a successful response to the need of making the solar power backup to sufficiently last an entire night with high intensity of illumination throughout. The PLB was a separate low voltage wiring independently distributed across the walkways and rooms of the nursery building. Hence, the lighting system so-demonstrated was a standalone 12 V system, which relieved the inverter system from the power-draining light bulbs. The application of the PLB technology as an essential system for an LMIC neonatal unit would require that a standard nursery building construction is strategically integrated with features for seamless installation of the PLB technology.
3.2 Individualized power buffer station
Modern day neonatology is highly reliant on machines and gadgets that are electrically powered. Experience from notable Neonatal Units in Nigeria, such as the Amina-centre in Minna and the Neoroom at CWCH Calabar, have shown that the application of the PLB enabled their standby power bank systems to sustain all power sockets longer than 12 h, covering the entire night hours of work [2]. However, this time coverage can easily drop by half during full unit capacity when many power-guzzling systems could be working simultaneously. A centre could have up to four oxygen concentrators, ten incubators, eight phototherapy machines, four ventilators, infusion pumps, and other life-support gadgets running at the same time. Our LMIC neonatal research efforts have strived to develop assembles of systems that could generate, store, and manage solar power for dusk-to-dawn facility energy supply to sustain facility operations until sunrise of the next day, when the batteries begin to re-charge again. Hence, our recent research has focused on the creation of an effective technical response to this scenario of ‘full house’ power demand to ensure all-night power coverage. The individualized power buffer station was, hence, conceptualized. In our concept, a typical 20 cot/incubator space capacity neonatal nursery is designed with a minimum of four power buffer stations, strategically located around the inner ward where two incubators could access the same buffer station for energy without being moved around. Unlike the main central powerbank system which is fully installed in the separate power room of the nursery complex, an individual buffer-station is located within the ward. This is a brick-built enclosure (length 600 mm, width 600 mm, height 300 mm) with ventilation openings on the sides and strongly secured wooden top cover. Each buffer-station is equipped with two numbers of 12 V, 150AH batteries connected in parallel, linked to the 12 V panel gang supply and recharged via a dedicated MTTP charge-controller. The buffer-station delivers outputs of 12 V DC via cigarette lighter sockets (Figure 3), and 230 V AC via a dedicated 3.0 KVA inverter.
Figure 3.
Cigarette lighter output at a buffer-station at SCBU-1 of the Federal Medical Centre, Owerri.
4. Building with intent to enhance nursing supervision
Shortage of nursing staff and poor nursing management techniques have all been previously associated with the factors identified to exacerbate high neonatal mortality in Nigeria [8, 12]. Amadi et al. [13] emphasized the need for LMIC facilities to improve on their staff strengths for their ever-busy neonatal centres, citing the Nigerian poor situation where the ratio of nurses-to-neonates per duty-shift was 1:10, or something worse. This poor ratio is not getting any better as the devastating economic situation in these countries has further fueled the massive exodus of qualified nurses out of the countries in search of better-paid jobs in foreign lands, particularly in the HICs. It has, therefore, become more difficult to stop or limit the Nursing Management of hospitals from their incessant staff-reshuffling, which leads to the posting of inexperienced nurses to work at the neonatal wards [13]. The exodus of experienced nurses has also resulted in a massive shortage of capable supervisors to guide the growing numbers of young or inexperienced nurses to whom the poor neonates are exposed in their on-the-job trial and error learning technique. The changing dynamics and SCBU nurses’ demography present the need for radical responses to counter the effects from any alterable avenues.
Typical, the Nigerian SCBU operations vests a lot of administrative duties on the Head Nurse (sometimes called the in-charge, chief-matron, or ward-manager), often keeping this senior staff away from the routine nursing work. SCBU-building segments in Nigeria are usually incorporated with ward-manager’s office, which are located away from the neonatal nursery halls. Head-nurses are unable to observe an on-going error in real-time for immediate intervention unless these happen during the few occasions when the head-nurse finds the time to walk into the hall for a quick look-around. Neonatal head-nurses could multitask the demanding administrative work with real-time nurses’ supervision to minimize fatal errors as has been orchestrated by the shortage of experienced neonatal nurses. This challenge, hence, inspired the new concept of creating nursery buildings that enhance the opportunity for head-nurses to multitask.
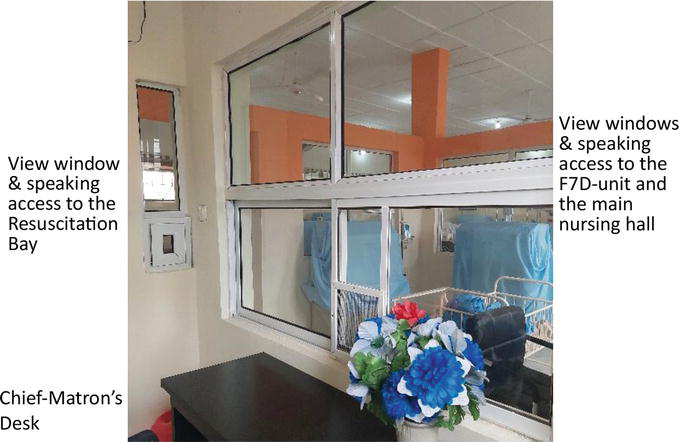
The new concept as has been implemented by our team ensures that the head-nurses’ office shares a common wall with the main nursery hall of the complex, such that the head-nurse is allowed a controllable panoramic view of all the work areas from the comfort of the managerial office. The adjoining walls could be developed into large see-through interactive windows and communication ports to aid the views of the manager and the ability to offer real-time instructions during work (Figure 4).
Figure 4.
Ward manager’s office at SCBU-1 of the Federal Medical Centre (FMC), Owerri.
5. Building-features with intent to enhance low-cost oxygen availability
Our on-the-job experience shows that piped-oxygen systems are too expensive to acquire and install at the resource constrained settings we assessed. However, the few hospitals that managed to procure and set up the oxygen system could not sustain these, and soon abandoned the use of the system due to high operational costs. Therefore, we conclude that many adverse factors make the imported brands of the technology unsustainable, even at the moderately well-to-do places of the LMICs [3].
One of the neonatal healthcare limitations of hinterland LMICs is unsustainable access to adequate supply of oxygen for neonatal respiratory support. Respiratory distress is a common condition that presents in very-low preterm or extremely-low birthweight neonates. Premature neonates who are born in the hinterlands are, by default, left to faith for survival as most attempts to access specialist care in the city are usually unsuccessful due to the often-treacherous transportation methods used. Neonatal lives can be easily saved if local healthcare Centre practitioners are trained in simple mechanized assistive breathing techniques. However, one of the major impediments would remain source-able oxygen for the mechanized applications. This chapter has already explored and presented ideas of sustainable generation, storage, and management of solar-harnessed power for usage at these remote locations of the world. We have used such energy to directly operate low-voltage (12 V DC) oxygen concentrators that produce up to 5 LPM oxygen flow, as this technology is commonly available in the internet market. At some of our centres, we use inverted high-voltage (220 V AC) from our battery storage to operate higher-power oxygen concentrators producing 8–10 LPM of oxygen flow. These technologies for real-time oxygen production at remote locations can be easily assembled. However, the high-power consumption rate of the compressors that operate the concentrators makes it difficult to run more than one or two such machines, simultaneously, without a quick depletion of the limited energy storage. This problem inspired our recent research to develop a low-cost sustainable method of distributing the generated oxygen to reach multiple patients, simultaneously. This is our ‘politeoxygen splitter system (the PSS)’ technology [3].
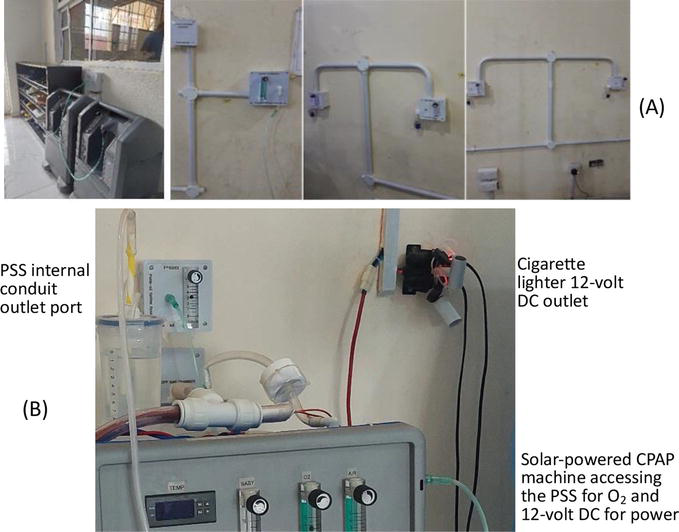
The PSS is capable of sharing and delivering the output from a single oxygen concentrator to reach up to eight neonates with patient-specific controls of prescribed individual flowrates simultaneously. This makes the PSS an essential feature of an NRS neonatal building design, within the cities and rural places of Nigeria. Therefore, modern LMIC nursery building constructions are recommended to feature internal conduiting sleeves and inspection chambers that are specifically integrated for the installation of the PSS. The conduiting creates invaluable channels for the survival of many neonates who would soon require sharing the minimally available oxygen amongst themselves, simultaneously. The earlier version of the PSS was achieved via surface installation of its distribution sleeve round the internal perimeters of the nursery hall (Figure 5). However, fresh builds of nursery halls are equipped with predesigned internal conduit sleeves for this purpose.
Figure 5.
The PSS (A) surface distribution sleeves (B) conduit installation.
6. Building with intent to mitigate neonatal infection and other deadly exposures
Neonatal infection has been implicated amongst the major causes of mortality in the newborn in Nigeria [14]. The efforts towards the prevention of a disease may always be cheaper than the huge and often unaffordable costs of treatment of infected patients. A variety of measures has been introduced as the standards of practice across Nigerian SCBUs, for example, to curb high neonatal infection rates. These include the use of ‘sharps boxes’, automatic electric hand driers that blow hot air, hand gloves and the use of hand sanitizing gels for the practitioners. Other measures include compulsory wearing of foot scrubs, gowns, and head covers for visitors at some Units. Observably, these sanitary measures are not equally enforced across all the SCBUs in Nigeria as most of these are completely missing in practices at so many facilities. These measures are considered helpful at other facilities; however, the practices are not strictly respected all the time, especially during the odd hours when high work pressure distracts the nurses from paying a full attention to the rules. Many of the managers agreed that enforcement of sanitary measures is also hampered by lack of specifically designated security officers to control visitor’s traffic, as well as poor workflow due to the structural layout of the floor plan of their facility. The efficiency of these infection-curbing measures, where practiced, can improve or dwindle depending on the structural plan of the SCBU layout.
In our privileged inspection of over 50 SCBU facilities across more than 80% of the States of Nigeria, we can reveal that less than 10 of the SCBUs could be adjudged adequate to enable effective sanitary control. Habitually, the government and heads of hospitals in Nigeria do not seek sufficient professional consultations before the design and construction of hospitals. Adult patients in the adult facility wards may easily cope with most fallouts from poorly designed or constructed building. However, the relatively unknown protective features of a functional SCBU-building are often missing, hence, most of the Nigerian SCBU-buildings are lacking in the ability to better protect the neonates. Unlike adult patients, the neonates are unable to cope, hence, some of them would die as a result. Therefore, it is essential that neonatal facilities are professionally earmarked and purposely structured during the design stage of any hospital facility. Purposeful and efficient neonatal building layout is one single factor amongst many considerations; however, it is one factor that saves huge amount of resources for LMIC practices when properly executed. Poor building positioning (as in defending against EFS) and structural layout (as in defending against infection) could be unquantifiably costly in losses of neonatal lives and in funding human traffic control, which could have been achieved naturally. Neonatal infection is caused by the propagation of bacteria that overpowers the non-immuned neonate. Infection could, therefore, be reduced by limiting the access of microbial vendors into the SCBU and by the application of a proper isolation-system for infected neonates. In this section, we highlight some often neglected aspects of SCBU positioning, layouts and features that could minimize infection and hence, neonatal deaths. Some of these features and specialized segments are usually difficult to adequately integrate into an already existing building through renovations, unless the building is substantially demolished to enable a better professional reconstruction. This is the concept our team applied in the newly reconstructed SCBU structure at the Federal Medical Centre, Owerri, Nigeria [15]. It is usually easier to conceptualize and integrate these into the original nursery building design ahead of construction.
Many channels of hospital infection are well-known adverse environmental conditions. Some of these adverse situations could be mitigated by a properly designed SCBU facility that specifically integrates important features as explained below:
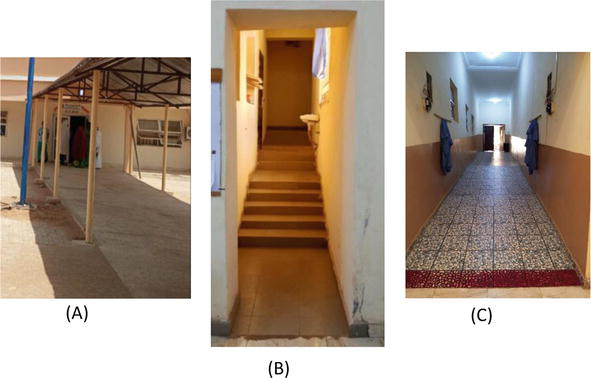
Exclusive neonatal transfer corridors linking the delivery and neonatal Units. During facility accreditation for postgraduate training licensing, strict demands are made in Nigeria for SCBUs to be located very proximal to Labour Wards and obstetrics-theaters for aiding a quick and seamless transfer of newly-born neonates from the obstetrics to the neonatal wards. This, they argue, is essential for the protection of the fresh neonate from environmental pollutions during transfer, especially in the prevailing circumstance where most tertiary hospitals in Nigeria do not have functional transport incubators. Over the years, quite a few tertiary hospitals have been able to comply with this requirement through the modification of their centres, or re-allocating possible facility spaces to relocate the SCBU closer to the obstetrics units. However, some of these modifications have still failed to maximally isolate the transported neonate from the so-called environmental contagions as the newly born neonates still have to be moved through public-shared corridors to access the SCBU. It is evident that environmental pollution can be high at some LMIC settings, hence, a demand for an exclusive neonatal transfer corridor, which can naturally keep-off wandering members of the public and non-related hospital staff, remains as valid as all efforts to keep the neonates alive. Exclusive neonatal transfer corridors have been intentionally implemented in the modification of some recent Nigerian centres that were anchored by our research team, for example, the NRS hubcentres of Yobe State in northeast Nigeria (Figure 6).
Specialized first-seven-days of life (F7D) room. The higher vulnerability of neonates during their F7D period of life has been highlighted in the Nigerian demographic survey reports, showing that 4-of-5 deceased neonates would die at this stage [16]. This fact inspired the concept of the F7D room of our team. Newly born neonates easily fall victims of cross-infection at Nigeria’s busy SCBUs due to a habitual nursing staff shortage [8]. The ratio of on-duty nurses-to-neonates can easily get worse than 1:9, with neonates on admission ranging from the most vulnerable ‘day-old extremely-low birthweight infants’ to more tolerable ‘full-term 20-days old’ infants [13]. Feeding time and the associated extreme work pressure makes the overworked staff to attend to all neonates, moving continuously from one to another, often forgetting to observe the in-between washing of hands or change of gloves to avoid transmission of infection. Observably, our research team can affirm that this is habitual in the Nigerian practice, requiring only one nearly impossible solution, which is the employment of adequate staff strength. Cross-infection is a high-risk situation, especially to the few days’ old more vulnerable preterm neonates who may not survive this. Inadequate staff strength can promote high cross-infection rate with its relatively higher consequences for the F7D-classified neonates. Staff employment is often a government policy, and uncontrollable by the local hospital management. However, an effective SCBU layout, which is controllable by the management, can help mitigate against cross-infection errors, which is common with inexperienced nurses. We created the F7D Room as an exclusive segment of the nursery hall where the premature and low birthweight neonates are nursed until their seventh day. The F7D nursing is only assigned to the best experienced nurses on duty rota.
External Oxygen cylinder chambers instead of frequent cylinder traffics into the SCBU. Most SCBUs across the regions of Nigeria do not operate on piped oxygen. Oxygen for daily work is supplied in oxygen-cylinders that are dragged right inside the SCBU, beside the cots and incubators, and maintained on refill-and-replace basis. Hence, the frequent back-&-forth movement of cylinders encourage transfer of microbes from dirty storage and gas-refilling shops via the indiscriminate entries of the ‘dirty’ gas technicians. Transmission of organisms owing to high traffic of dirty oxygen cylinders may be a major contributor to high neonatal infection rate in Nigeria, and this needs to be studied. We proposed and implemented building designs with inbuilt oxygen cylinder chambers behind the walls of the SCBU and connected via short pipes across the walls into the SCBU’s wall-mounted humidified flow gauges and controllers. Access to the cylinders is restricted with locks depending on how the chamber is exposed to passers-by (Figure 7).
Mothers’ dormitory exclusive access to the ‘milking’ and ‘kangaroo mother care (KMC)’ rooms. Personal hygiene of nursing mothers is highly emphasized but may be easily implemented through some building enabled restrictions. Nurses, who are mostly women in Nigeria, assist in various inspections that help to educate and remind the mothers on the vital rules of hygiene to keep their babies safe. These needs inspired designs for adjoining mothers’ dormitory with exclusive access to the milking and KMC rooms. The typical structure created by our team ensures private assistance of nurses to the nursing mothers through the exclusive corridor (Figure 6B). This allows mothers to enter the KMC room for any interaction with their own babies who are brought to them in the KMC room, without the mothers entering the main nursing nursery halls where the other neonates are.
Figure 6.
Exclusive neonatal transfer corridor at Potiskum NRS hubcentre in Yobe State (A) public access to SCBU office sections (B) nursing mothers’ exclusive access to milking/KMC rooms (c) neonate exclusive corridor linking Delivery room & SCBU.
Figure 7.
External oxygen cylinder chambers behind the Neoroom walls at Calabar Women & Children Hospital (CWCH), Calabar, Nigeria.
The other building features include:
The integration of external public access to administrative and ward mangers’ office without passing through the nursery’s nursing halls by non-SCBU staff on duty.
The integration of access to the seminar and conference sections of the Unit without entering or passing through the nursery’s nursing sections.
The integration of a scrub and gowning room and locating this just before the entrance of the nursery’s nursing halls.
The integration and location of an independent ‘septic or isolation’ room for infectious neonates, with its exclusive cross-ventilation, separate from the rest of the nursery’s nursing halls.
7. Building with intent to sustain high sanitary standards through running water supply
It is well-known, even at private homes, that availability of water is essential to keeping a good hygiene standards to reduce contaminations and diseases. The hospital environment is a setting too dangerous to compromise water availability due to high vulnerability of patients. It is difficult to operate an efficient hospital, even in the hinterlands of the LMICs, without adequate infection controls. Sanitary measures for minimisation of infection outbreaks are often mediated using sustainable running water supply through pipes and taps that are distributed around the facility. Lack of sustainable running water supply in hospitals at LMICs is widespread. This situation is easily observable in many well-known healthcare institutions in Nigeria, and as has been reported from other LMIC settings [17]. Although a situation of health practice without water may be horrifying to imagine from the standards at HICs, it is nevertheless, a situation that seems not to bother practitioners in these LMIC centres irrespective of the observable consequences of the spread of diseases and poor overall health outcomes.
Public infrastructure such as pipe borne water supply is either irregular or completely inexistent at many city settings in Nigeria where hospitals are located. Therefore, private borehole installation powered by electricity is the most common solution at these facilities. The drawback, however, remains the well-known epileptic public power supply to these centres and the high cost of fossil fuel to run power generators. Hence, the problem is a ‘round the circle’ nightmare. Needless to say that this is more terrible for facilities located in the hinterlands of the LMICs, where we must create a viable solution to support our NRS advocacy of “reversal of neonatal traffic by taking our medicine to the neonates where they are” to eliminate the transport-induced distress that worsens their death rates [4].
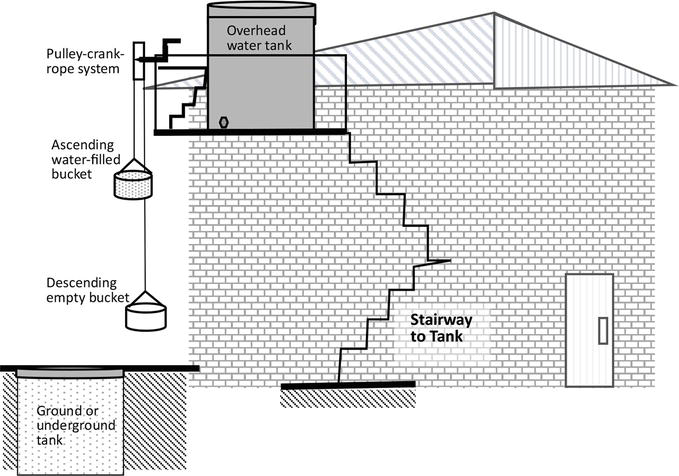
In our NRS facility designs, an appropriate segment of the building is featured with a stairway access to the loft or rooftop, where an appropriate flat surface is constructed for the installation of an overhead water tank that would be linked to supply the pipes and taps in the SCBU facility. Safety barriers are constructed to confine the tank against the wind and protect people accessing the tank platform from falling. A very simple pulley-crank-rope mechanism could be locally constructed on the provided barrier, with buckets tied to the two ends of the rope (Figure 8).
Figure 8.
Illustration of NRS-building featuring overhead water tank system.
Water is delivered to the overhead tank via solar powered water pumps that lift water from the conventional underground tanks or locally dug wells, as normally seen in the rural areas. It is essential to apply low-cost sustainable techniques that the local people can manage to sustain without much external assistance. Therefore, the low-voltage pumps, which are powered via our 12 VDC solar pannel gang (see Section 3), is the default method of lifting water into the overhead tank. At other likely times of pump failure, two other methods could be activated – manual and semi-manual. In the manual method, hospital oderlies would be required to climb the stair ways with water cans to fill up the overhead tank. The semi-manual option is performed by two persons, one on ground level refilling buckets and the other on the overhead tank platform, cranking the pulley-crank-rope system to lift water-filled bucket at one end of the rope whilst lowering an empty bucket for a re-fill at the other end of the rope (Figure 8). A servicing-hole with removable cork near the bottom of the overhead tank is used for a quick evacuation of contaminated water whenever this becomes necessary, or during the periodic washing of the tank. The orderlies are taught on how to use a ‘provided’ wash-stick for cleaning. The wash-stick is a construct of a long PVC pipe that is screwed to a spongy brush.
The nursery building is a vital equipment factor to consider without compromise in the setting up of a special care baby unit (SCBU) anywhere in the world. The LMICs are trailed with a lot of social and infrastructural limitations that often hinder the delivery of safe neonatal services, but little is known about possible building features and layouts that could effectively mitigate the effects of these limitations. Over the last 25 years, our group has carefully and consistently researched and implemented some of these various features, which are currently reaping good positive impacts.
A lot of SCBUs across Nigeria have benefitted from the wealth of knowledge so-generated through our research findings, trialing and implementations. In recent years, some freshly built or ‘demolished-and-rebuilt’ SCBUs have succeeded in the integration of a multitude of these individual features, simultaneously, thereby witnessing a delightful new experience of successful and safe neonatal environment. One of such efforts was implemented at Owerri, southeast of Nigeria. The re-engineering of the little space that accommodated what is referred to as the ‘SCBU-1’ of the Federal Medical Centre Owerri by our team in 2022, endaevoured to integrate as many of these features as possible. Thereby, a highly revolutionized practice setting was created. At the end of 12 months of continuous usage of the new SCBU-1, an interview team of two nurses from another department of the hospital was constituted. The team was commissioned to discretely target five unsuspecting senior nursing officers (SNO), who were longserving staff members of SCBU-1, to obtain their qualitative assessments of the new SCBU-1 as compared to the functionality of the demolished SCBU-1. The team applied a guided questionnaire technique involving a private informal chat session with the unsuspecting interviewee. It was necessary to apply this technique to avoid biased responses. Each of the five SNOs was interviewed separately by someone who was familiar, hence creating a friendly setting that encouraged the unsuspecting SNO to provide an honest comparison based on the content of the questionnaire (Table 1).
S/N
Criteria (Score: 0–100%)
Details of criteria and scoring benchmarks
The Federal Medical Centre, Owerri
1
Usage till date
How long has the new SCBU-1 been in use till date?
12 months
2
Lighting coverage
The corridor
By how much satisfaction does the polite-light-bank (PLB) illumination sufficiently cover walking around safely at night without the need for extra lighting? No illumination (0%) – extremely sufficient (100%)
100100100100100
100%
Inner SCBU
100100100100100
100%
3
Workflow
This relates to the nurse’s sitting arrangement, ease of observation and swift attendance to the neonate on admission during nursing care [equal level as former (0%) – completely far better (100%)]
10010010010080
96%
4
Ease of reception of new patient
By what % improvement has the new building design made easier the process of admitting new neonates?
8010010010080
92%
5
Nurses’ private areas
The new concepts of (1) napping couch and study privacy (2) storage and (3) showering. By how much % has this encouraged nursing efficiency and services
10080100100100
96%
6
Matron’s office
The new concept created a kind of ‘bird eyes’ view for the matron from the comfort of her office desk. How does this compare to previous situations [gives her no better control (0%) – best effective control (100%)]
100100100100100
100%
7
Mini conference/utility area
What is your fair score of this section?
10010010010080
96%
8
Mothers’ milking cubicle
How do you score this privacy for milking mothers?
5070607080
66%
9
Equipment base
How does the amount and caliber of installed equipment compare to your expectations? Poorer than expected (0%)..(100%) more than expected
808080100100
88%
10
Overall satisfaction
What is your overall satisfaction rating for the ingenuity in this new concept compared to what you knew previously? No difference (0%)..maximally satisfied (100%)
1008090100100
94%
Table 1.
Qualitative assessment of nursing functionality of the new SCBU-I compared to the former.
Five senior user nurses were discretely and unsuspectingly questioned by another colleague from a different hospital Unit specifically requesting: “if you scored the former “0%”, how much could you score the new SCBU-1 on these criteria?”
The obtained answers evidently show a strong agreement amongst the nurses that these features have made some remarkable impacts in their experiences. It is also noteworthy that all five interviewees expressed disappointment with the smallish capacity of the ‘milking cubicle’ as this could only take a maximum of five nursing mothers at a time. Therefore, each of the interviewees returned a low score for the cubicle. However, the question of size was a fundamental issue of the available landspace, which was too small to accommodate a larger room for the milking mothers.
We wish to thank our interviewers who helped us to achieve our unbiased assessment of the NRS-inspired designs of the special care baby units. This work was supported by Neonatal Concerns for Africa, a subsidiary of the Mastermind group, Nigeria. Professor Hippolite Amadi’s outreach in Nigeria is supported by the Hornchurch Baptist Church, England, United Kingdom.
1.Amadi HO, Adesina CT, Olateju EK, Omokaro S, Okechukwu AA, Alabi P, et al. Validation of a novel technique that minimises early neonatal deaths – A comparative study. Journal of Paediatrics and Neonatal Care. 2017;6(1):00232
2.Amadi HO, Abubakar AL. LMIC facility-lighting limitation in Nigeria fully resolved by a novel frugal Polite-light-bank technology. Global Journal of Medical Research. 2023;23(3). Available from: https://globaljournals.org/GJMR_Volume23/1-LMIC-Facility-Lighting-Limitation-in-Nigeria.pdf
3.Amadi HO. The Politeoxygen splitter system (PSS) – A frugal LMIC oxygen delivery technology that expands the utility by up to 700%. Journal of Paediatrics and Neonatal Care. 2023, 2023;13(2):75-80. DOI: 10.15406/jpnc.2023.13.00495. Available from: https://medcraveonline.com/JPNC/JPNC-13-00495.pdf
4.Amadi HO, Kawuwa MB, Abubakar AL, Adesina CT, Olateju EK. A community integrated concept that minimises death of most vulnerable neonates at poor-resource environments. Journal of Paediatrics and Neonatal Care. 2022;12(3):170-173. DOI: 10.15406/jpnc.2022.12.00475
5.Amadi HO, Mohammed IL, Kawuwa MB, Oyedokun A, Mohammed H. Synthesis and validation of a weatherproof nursery design that eliminates tropical Evening-Fever-Syndrome in neonates. International Journal of Paediatrics. 2014;2014:986760. DOI: 10.1155/2014/986760
6.Amadi HO. Neonatal thermoneutrality in a tropical climate. In: Alfonso J. Rodriguez-Morales Ed, Current Topics in Tropical Medicine. London, UK: InTech Open, Croatia; 2012. p. 513-544. Available from: http://www.intechopen.com/books/current-topics-in-tropical-medicine/neonatal-thermoneutrality [Accessed March 16, 2012]
7.Amadi HO, Olateju EK, Kawuwa MB, Osibogun AO, Alabi P, Ibadin MO. Neonatal hyperthermia and thermal stress in low- and middle-income countries: A hidden cause of death in extremely low-birthweight neonates. Paediatrics and International Child Health. 2015;35(3):273-281. Available from: http://www.maneyonline.com/doi/pdfplus/10.1179/2046905515Y.0000000030
8.Uchendu C, Windle R, Blake H. Perceived facilitators and barriers to Nigerian Nurses’ engagement in health promoting behaviors: A socio-ecological model approach. International Journal of Environmental Research and Public Health. 2020;17(4):1314. DOI: 10.3390/ijerph17041314
9.Adair-Rohani H, Zukor K, Bonjour S, Wilburn S, Kuesel AC, Hebert R, et al. Limited electricity access in health facilities of sub-Saharan Africa: A systematic review of data on electricity access, sources, and reliability. Global Health Science Practise. 2013;1(2):249-261. DOI: 10.9745/GHSP-D-13-00037
10.Ohajianya AC, Abumere OE, Owate IO, Osarolube E. Erratic power supply in Nigeria: Causes and solutions. International Journal of Engineering Science Invention. 2014;3(7):51-55
11.Ekanem EE, Fajola AO, Ogbimi R, OgievaB JI. Use of solar energy for the provision of cost-effective and environmentally friendly power supply in health facilities in the developing world- lessons from a community cottage hospital in Southern Nigeria. International Journal of Research Science & Management. 2014;4(4):32-37. DOI: 10.5281/zenodo.546865
12.Amadi HO, Kawuwa MB. 2018. Reducing early neonatal mortality in Nigeria – the solution. Selected Topics in Neonatal Care. Barria R Mauricio. London, UKInTech Open, Croatia, 221-237 10.5772/intechopen.69221. https://www.intechopen.com/books/selected-topics-in-neonatal-care/reducing-early-neonatal-mortality-in-nigeria-the-solution [Accessed November 13, 2018]
13.Amadi HO, Osibogun AO, Eyinade O, Kawuwa MB, Uwakwem AC, Ibekwe MU, et al. Challenges and frugal remedies for lowering facility based neonatal mortality – A comparative study. International Journal of Paediatrics. 2014;2014:986716. DOI: 10.1155/2014/986716
14.Odejimi A, Quinley J, Eluwa GI, Kunnuji M, Wammanda RD, Weiss W, et al. Causes of deaths in neonates and children aged 1-59 months in Nigeria: Verbal autopsy findings of 2019 Verbal and Social Autopsy study. BMC Public Health. 2022;22(1):1130. DOI: 10.1186/s12889-022-13507-z
15.Neonatal Concerns for Africa. A Range of Solar Powered Devices that Enables Neonatal Intervention at Remote Locations – FMC Owerri Video Report. 2022. https://www.youtube.com/watch?v=lAC0H-CwOSc [Accessed June 2, 2023]
16.MCA, World Health Organisation. Maternal and Perinatal Health Profile of Nigeria, Africa Region. Maternal and Perinatal Country Profile [Internet]. Available from: http://www.who.int/maternal_child_adolescent/epidemiology/profiles/maternal/nga.pdf [Accessed: February 02, 2017]
17.Chawla SS, Gupta S, Onchiri FM, Habermann EB, Kushner AL, Stewart BT. Water availability at hospitals in low- and middle-income countries: Implications for improving access to safe surgical care. Journal of Surgical Research. 2016;205:169-178. DOI: 10.1016/j.jss.2016.06.040
Written By
Hippolite O. Amadi, Mohammed B. Kawuwa, Amina L. Abubakar and Stephen K. Obaro
Submitted: 09 June 2023Reviewed: 03 July 2023Published: 19 September 2023