Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
Light is a very effective tool for the treatment of neonates with problems at birth. It includes different wavelengths that can cause damage for different reasons when misused. Taking into account the characteristics of the light rays applied to neonates is important in the field of phototherapy, for the application of good clinical practices and prudent avoidance, in risk management. In this chapter, research on the application of phototherapy will be presented, highlighting the non-visible risks of using light in incubators and thermal cradles. In addition, recommendations will be made about specific aspects regarding the use and application of light for both neonate. The results show that the application of phototherapy increases the levels of electromagnetic radiation. Therefore, it must be taken into account that, although it is of vital importance for the care of preterm neonates, artificial light is a tool whose operation depends on electrical energy and represents a risk that could subsequently affect their state of health.
Universidad Tecnológica de la Habana “José Antonio Echeverría”, La Habana, Cuba
Yenisel Díaz Roller
Universidad Tecnológica de la Habana “José Antonio Echeverría”, La Habana, Cuba
Iosvany Aguiar Ramos
Centro de Biomateriales de la Universidad de La Habana, La Habana, Cuba
*Address all correspondence to: janetco@automatica.cujae.edu.cu
1. Introduction
Jaundice is the yellowish discoloration of the skin and mucous membranes caused by the accumulation or deposit of bilirubin, which, according to clinical data, occurs in 60–70% of newborns [1]. Some authors claim that in newborns (NB), it is a condition that can cause neuronal damage when there are excessive amounts of it, producing permanent neurological sequelae in the patient [2]. This is why this pathological condition must be prevented by maintaining safe levels of bilirubin in the blood. To achieve these levels, phototherapy has been one of the most used techniques, through which the transformation of bilirubin into water-soluble photoisomers is achieved thanks to the effect of light on it, which allows them to be more easily excreted through feces and urine, without the need to be conjugated in the liver [3].
Phototherapy is a technique used in neonates to combat certain conditions that occur in them during birth, high levels of bilirubin being one of them. These phototherapy units are made up of four blue light tubes and two white light tubes. The blue ones are placed in the center, and the white ones on the sides. Light tubes or bulbs, whether LED, halogen, or fluorescent, are classified according to the maximum wavelength produced by the emitted light. Among the different types, there are: specialized blue fluorescent lamps, compact fluorescent lamps and halogen spotlights or lamps with an LED system. Some of these are also used to illuminate the work area in general.
Fluorescent tubes have plexiglass shields to filter out any ultraviolet radiation and do not emit dangerous levels of infrared radiation. LED bulbs emit blue light that does not increase temperature or emit ultraviolet radiation. However, these bulbs, with high levels of radiation, can damage the eyes and skin, so they must include internal filters and reflectors to reduce them.
According to Maxwell’s theory [4], light is a wavelength perturbation in an electromagnetic field in the form of radiation that propagates at a defined speed. Their characteristics are:
Amplitude (wave height).
Wavelength (spatial behavior): λ (nm).
Speed: c (km/sec) is the distance the wave travels in 1 second.
Frequency (temporal behavior): v (hz), defined by the number of waves that pass a fixed point in one second. It is related to the wavelength, since it depends on its size. It is estimated at the wavelength multiplied by 1014 cycles per second.
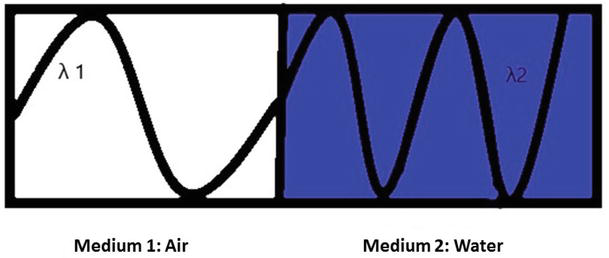
Light is transmitted in a vacuum at the speed of 299,792.458 km/sec, according to Einstein’s theory of relativity, comprising different wavelengths and frequencies. When the medium changes, its speed and wavelength change, but its frequency remains constant [5], as shown in Figure 1.
Figure 1.
Behavior of light from one medium to another. [own creation].
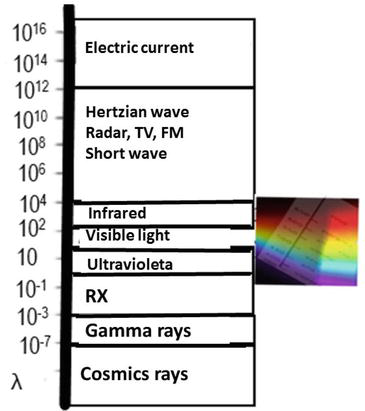
The electromagnetic spectrum is nothing more than the arrangement of radiant energy according to wavelength (λ) or frequency. It extends from wavelengths of 1016 to 10−7 m, as seen in Figure 2. At the lower end are the highest frequencies, which are the short wave and the highest energy, equivalent to cosmic rays. On the opposite side, long waves can be found, whose wavelength is highly variable and are used for radio communications, where X-ray, ultraviolet (UV), visible, and infrared (IR) rays are located.
Figure 2.
Electromagnetic spectrum. [own creation].
It can be said that the three major regions of importance in the field of lighting are infrared light, visible light, and ultraviolet light. However, despite being so significant for human life, the visible spectrum corresponds to a tiny portion of the spectrum of electromagnetic waves. Although UV and IR rays are not detected by the human eye, their effect can be noticed physiologically. To measure the visible spectrum, the most used unit of measurement is the nanometer (nm), which is equivalent to 10−9 m.
2.1 Light spectrum
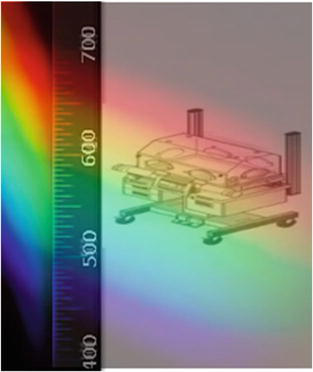
The light spectrum is nothing more than the decomposition of white or visible light into colors that delimit its wavelengths [6]. This ranges from ultraviolet to infrared, defined between wavelengths that range approximately from 380 to 770 nm, as can be seen in Figure 3.
Figure 3.
Light spectrum. [own creation].
Perceived white light, as mentioned above, is a mixture of all visible wavelengths. The visible spectrum can be broken down into its different wavelengths using a quartz prism, which refracts each of them selectively through colors. The human eye separates, by capturing color, each of the different wavelengths and frequencies present in this range.
Each wavelength interval is represented by a color:
Blue and violet correspond to short wavelengths, approximately 380 to 500 nm.
Red and orange correspond to long wavelengths, approximately 590 to 700 nm.
Green and yellow are found in the middle zone, which covers wavelengths from 500 to 590 nm.
Achieving monochromatic light radiation, that is, one that responds to a single wavelength, is very difficult. The light sources that most closely resemble this type of emission are the laser and the low-pressure sodium lamp.
Radiant energy is made up of electromagnetic waves with a range of frequencies (ѵ) ranging from 108 to 1024 s−1 and propagates at a constant speed (of light), whose value is exactly 299,792,458 m/s [5].
2.1.1 White light
White light is the result of the sum of countless wavelengths that, when added, become colored rays, giving rise to the perception of the color white. As stated by Mosquera Torres et al. [7], white light is 25% blue light.
Most lamps intended for lighting work areas in the health sector emit white light. This condition is necessary for the safety and protection of management and the health of both patients and workers.
2.1.2 Blue light
Basically, phototherapy applied to neonates with conditions at birth is based on the use of blue and white light. Wavelengths between 380 and 500 nm include the violet, blue, and green areas of the spectrum [8]. This part of the spectrum is also known as high-energy, short-wavelength visible light.
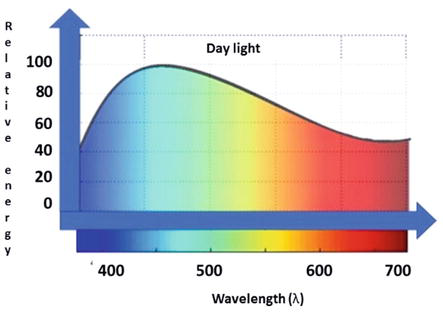
Sunlight is the main natural source of blue light, although there are enough sources of artificial blue light for humans to be exposed 24 hours a day. In 2013, a panel of American experts [8] pointed out that solar radiation is 25–30% blue light, as shown in the spectrum in Figure 4.
Figure 4.
Representation of the daylight spectrum. [own creation].
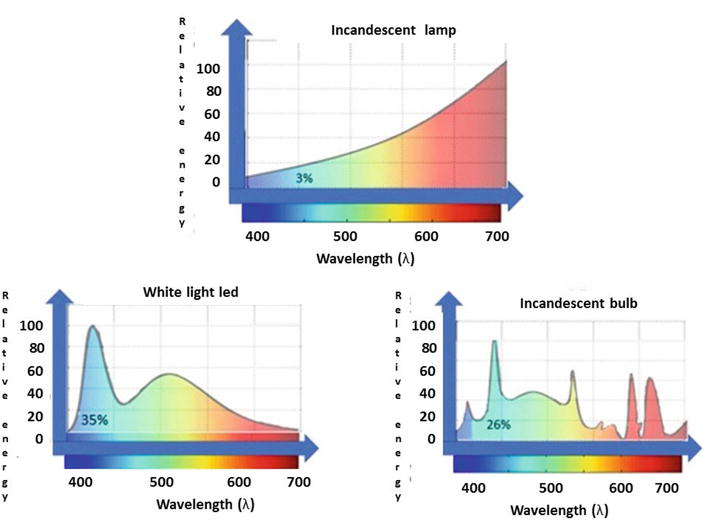
All artificial light sources have blue light in their spectrum in different percentages; thus, conventional incandescent light lamps have the least with around 3%, low consumption compact fluorescent lamps at approximately 26%, and LED lamps, which emit cool white light, blue light is 35% one of the strongest components [8], as shown in Figure 5.
Figure 5.
Representation of the spectrum of some artificial light sources. [own creation].
Jiménez-Rubio et al. [9] mention that blue light provides benefits to the synchronization of circadian cycles and the production of melatonin, if it is properly provided during the day and night cycles, also as it has been shown to provide the newborn with high levels of bilirubin an effective treatment [10], but at the same time, it must be taken into account that the indiscriminate use of this type of light poses specific risks to vision and skin that are irreversible due to its power of penetration into biological material [11].
For their part, studies carried out in the last decade have suggested that phototherapy is associated with type 1 diabetes [12, 13], damage to the immune system, leukemias [14], and asthma [15] as late and long-term effects. The relationship, according to these investigations, is due to the fact that by applying phototherapy 24 hours a day, the neonate is inhibited from producing what is necessary to raise the immature immune level. This situation, as stated by Boidi [16], causes a deficiency of T lymphocytes, molecular alterations in the DNA of mononuclear leukocytes, alterations in the concentrations of interleukins that tend to slow down the change in an immune response, increasing the risk of suffering in the long term—the mentioned diseases.
3. Lighting environment in a neonatal intensive care unit
Currently, there are no standards that standardize adequate light levels in a Neonatal Intensive Care Unit (NICU), as this structurally depends on the geographical characteristics of the place, the type of care provided in the unit, and the design and location of the Windows. Additionally, the condition of the newborn and its location within the area must be taken into account.
For premature babies, reducing light, as well as maintaining the light and dark cycle, is of vital importance, which is why it is convenient to have intensity regulators to adjust the light power depending on the needs that arise daily around them. Him.
As recommendations to maintain the minimum lighting conditions, it is adopted that, during the day, the light oscillates between 100 and 200 lux, preferably supported by natural light and, at night, artificial light of approximately 50 lux, but allowing it to be adapted between 10 and 600 lux independently depending on the case [17]. If a short-term evaluation of a specific RN is necessary, between 1000 and 1500 lux can be used, avoiding interference with nearby children.
In nursing work areas, it is advisable to have moderate levels of lighting with the possibility of regulation and during the day to take advantage of natural light, somewhat distorting its direct action on the work area.
3.1 Types of phototherapy that an incubator can offer
Today, there are several modalities of phototherapy such as:
White light, which is used everywhere (in the thermal crib (TC) or radiant crib, in the case of premature babies).
Blue light and fiber optic or biwhite light (in which the child can be dressed during phototherapy and phototherapy can be performed at home).
High-intensity phototherapies, which are double phototherapies, have shown greater benefits.
The effectiveness of phototherapy depends on the irradiation of the light source. Irradiance is expressed in units of watts or microwatts per square centimeter per nanometer (W/cm2/nm) (μW/cm2/nm), respectively, within a given wavelength band [3].
Depending on the maximum wavelength produced by light and the hours of exposure to it, there are different types of phototherapy, such as:
Simple, standard, or conventional phototherapy: radiation of 8–10 μW/cm2/nm emitted by a lamp with fluorescent tubes, two white and four blue, is used.
Intermittent or continuous phototherapy: as the name indicates, it works with cycles of light exposure and cycles of rest. The lamps used for standard phototherapy are used and are classified as:
Intermittent phototherapy: characterized by cycles of light exposure and rest cycles, it is normally composed of 12 hours of exposure and 12 hours of rest. Only simple or conventional phototherapy can be applied intermittently.
Continuous phototherapy: in this type of phototherapy, light exposure is carried out 24 hours a day, pausing only during essential moments such as feeding or diaper changes.
Double or intensive phototherapy: uses radiation greater than 30 μW/cm2/nm and uses lamps with six blue tubes.
Miriam Janet de la Rosa [18] suggests that, when placed 20 cm above the newborn, phototherapy units with conventional or standard light should provide spectral irradiation of 8–10 μW/cm2/nm, in the 430–490 nm, while special blue fluorescent lamps provide 30–40 μW/cm2/nm, in that same band.
On the other hand, there are investigations [1, 19] that show that the benefits that light therapy provides on bilirubin have reported negative clinical results on the pathophysiology of NBs, such as lower weight gain, alterations in sleep development and stress in very premature or seriously ill patients. What could be associated with electromagnetic radiation resulting from the use of electrical energy to keep the phototherapy equipment and other elements that make up preterm NB treatments in operation?
Electromagnetic fields (EMF) are a combination of electrical and magnetic waves that travel simultaneously [20]. They propagate at the speed of light and are characterized by a frequency and its corresponding wavelength. These two characteristics are directly related to each other: the higher the frequency, the shorter the wavelength. All equipment that needs to be connected to the electrical energy network emits electromagnetic radiation when it comes into operation. Light lamps of all types have this condition, which is why they emit electromagnetic radiation.
According to the Council of the European Union, the basic constraint limit allowed for any point or spatial measurement is equivalent to a magnetic induction (β) of 6.25 μT [21]. Electromagnetic radiation capable of exciting the retina and creating the sensation of vision belongs to the area of the spectrum called visible light, as shown in Figure 2.
Electromagnetic radiation has been recognized by the World Health Organization (WHO) since 2002 [22] to cause health damage. This damage is subject to the behavior of different variables, such as:
Exhibition time
Radiation level
Distance at which the source of the radiation object is located
Person’s health criterion
Adding fields near the radiation source.
Electromagnetic fields are not subtracted; they only add the radiation that they emanate to others and themselves. To reduce the levels of radiation that reach the irradiated object, it must be taken into account at what distance to place it. Issue that is regulated by the International Electrotechnical Commission (IEC) to avoid interference between equipment. In the case of lamps or luminaires, it is recommended that they be located approximately 1.5 m away from people, due to the levels of radiation they emit.
The objective of this research is to demonstrate that the use of light in intensive care units brings dangers that are not taken into account by the people dedicated to working in them, either because it is not visible or due to a lack of knowledge.
For this, a research protocol divided into three stages was drawn up:
Stage 1: The magnetic field of the NICU area was measured using a PCE-G28 gaussmeter. This area includes a monitoring cubicle (indicated as 1) and seven confinement cubicles for the care of neonates (indicated from 2 to 8).
The gaussmeter was placed one meter away from the ground (the height at which the babies are lying), meter by meter was measured in a timely manner, moving the measuring equipment throughout the area and always starting with the area furthest from the entrance door and counterclockwise.
Stage 2: The magnetic field radiated by an incubator with only six months of operation and a thermal cradle with the same operating time was measured. The measurements were carried out in isolated rooms where no medical equipment coexisted around them and turned on one at a time. Furthermore, these values were taken with the incorporation of light therapy, to use them as a behavioral pattern of emitted radiation for future comparisons.
The gaussmeter was positioned vertically on the four sides of the incubators and thermal cradles, averaging the specific value to which the baby would be subjected while inside it. This operation was performed five times to achieve statistical validation.
For this, the percentage, chosen by brand and model, that these would occupy within the equipment in operation, at the time of the investigation, was taken into account.
Stage 3: The values irradiated by the incubators and thermal cradles were measured during their operation in each of the cubicles in the area to be investigated, using the same procedure as for the reference standard. A comparison graph was made with respect to the pattern measured in isolation, taking into account those that were applying light and those that were not.
Note: The investigation was carried out with a general air conditioning regime and light on only in the measured areas.
As a result of the application of the methodology explained above, the color maps shown below were obtained; these represent the magnetic field values irradiated in each of the stages mentioned above. For greater understanding, they will be presented in stages.
5.1 Stage 1
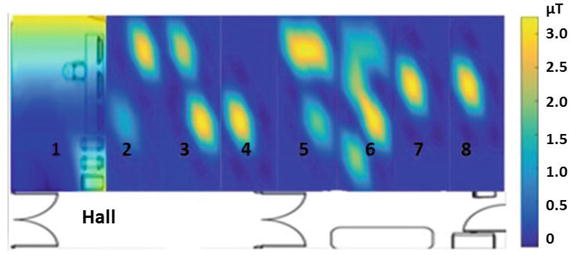
In this stage, general magnetic field values were obtained in each cubicle. They are represented by a color map in Figure 6.
Figure 6.
Color map of the magnetic field of the general area with the equipment in operation.
The color bar shows that the highest radiation values are above 2 μT, represented in yellow, and can be observed in specific areas that symbolize the presence of a magnetic field generator in operation. The generators in this case are incubators and thermal cradles with or without phototherapy light applied.
5.2 Stage 2
For this stage of the research, the percentage of incubators in terms of brand and model was taken into account, and the one with the shortest operating time was taken, in the same way as thermal cribs. The values obtained from the measurements are presented, as averaged in Table 1.
Equipment
Average of five measurements
Light off
Light on
ATOM Medical V-85 Incubator
0.68 μT
1.17 μT
Medix Thermal Crib
0.45 μT
0.93 μT
Table 1.
Measurements were made in an incubator and a thermal cradle to obtain a behavior pattern with respect to magnetic field radiation.
With respect to technological equipment, ten incubators were in use, eight of which were Atom Medical V-85 brand (located in cubicles 2, 3, 4, 5, 7, and 8) and five thermal cribs, all of which were Medix brand. (located in cubicle 6). All equipment in operation has been in that condition for more than five years.
5.3 Stage 3
Once the reference values to be used were obtained, the magnetic fields irradiated by the equipment in operation were measured following the protocol of stage 2. The values grouped in Table 2 were obtained. The light used was continuous blue light.
Cubicle
Equipment
Light on
Light off
Reference
2
Incubator 1
2.30 μT
1.17 μT
Incubator 2
0.66 μT
0.68 μT
3
Incubator 1
2.22 μT
1.17 μT
Incubator 2
1.87 μT
4
Incubator 1
2.15 μT
5
Incubator 1
2.20 μT
Incubator 2
2.67 μT
Incubator 3
0.2 μT
0.68 μT
6
Thermal crib 4
0.84 μT
0.45 μT
Thermal crib 5
0.5 μT
Thermal crib 6
0.54 μT
Thermal crib 7
0.45 μT
Thermal crib 8
2.1 μT
0.93 μT
7
Incubator 1
2.19 μT
1.17 μT
8
Incubator 1
2.19 μT
Table 2.
Table showing the magnetic field radiated by the equipment in operation, at the time of measurement with the phototherapy light on or off.
As has been proven by some researchers, as electrical or electronic equipment comes into operation, the ambient magnetic field of the area increases its radiation level.
In Figure 7, the range of colors shows the difference in the levels of electromagnetic radiation radiated by the incubators. In this figure, it can be seen that:
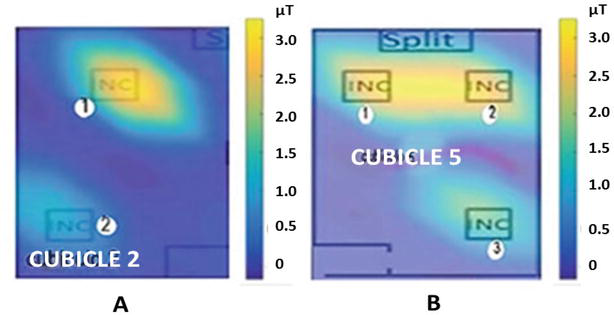
In cubicle 2, incubator 1 has an intense yellow color that indicates a higher level of radiation (2.30 μT), while in incubator 2 it has a blue color that, according to the color bar, represents lower levels (0.66 μT, in this case).
In cubicle 5, the difference is revealed between incubator 3 and incubators 1 and 2 (approximately from 2.0 to 2.47 μT), showing that as the blue light treatment of phototherapy is incorporated, they reach higher values in incubators 1 and 2 (2.20 and 2.67 μT, respectively), than the value obtained in incubator 3 (0.2 μT), which does not have associated phototherapy.
Figure 7.
Representation of the difference in electromagnetic radiation generated by incubators with phototherapy, (A) 1 and (B) 1 and 2 and without phototherapy included in the treatment of preterm newborns, (A) 2 and (B) 3.
The difference in values represented between (A) and (B) for the incubators where the use of phototherapy is present, could be given by the exploitation time, an issue that influences one of the factors mentioned above as a behavioral variable of the electromagnetic field. Also, the amount of equipment used in the treatment to keep the newborn alive is sometimes between 4 and 5, located around the incubator.
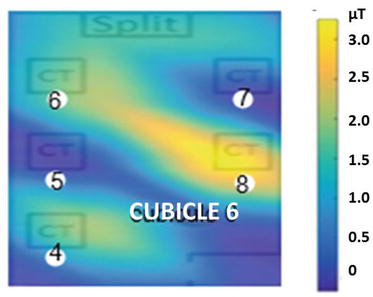
Figure 8 represents the behavior of electromagnetic radiation, when the phototherapy lights are working or not. During the operation of the thermal cradles, it is represented by the display of colors whose values are incorporated numerically in the bar. In the thermal cribs located in cubicle 6, only five cribs were providing service, and the only one that had the phototherapy treatment incorporated was number 8 (2.1 μT), and this is expressed by the intense yellow color that is represented in the map. Here, it can be seen that the difference between values when phototherapy is being applied and, when not, ranges approximately between 1.2 and 2 μT, values lower than the difference shown in the comparison of the incubators.
Figure 8.
Representation of the difference in electromagnetic irradiation, through colors, while the phototherapy treatment is applied in the thermal cots in cubicle 6.
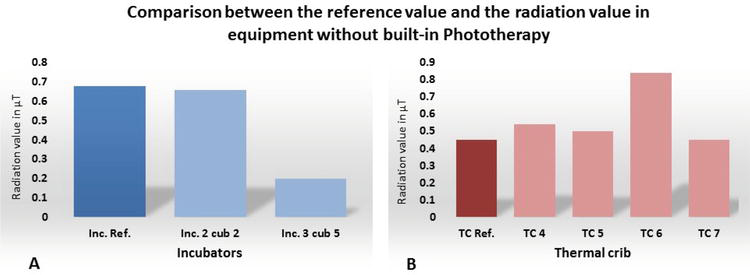
If the reference patterns are taken into account with respect to the values measured during the investigation, to make a comparison about the levels reached by this life support equipment in a NICU, the graphs shown in Figures 9 and 10 were obtained. They will be shown separately depending on whether the equipment incorporates light therapy or not.
Figure 9.
Comparison graphs of electromagnetic radiation without applying phototherapy in incubator (A) and thermal cradles (B).
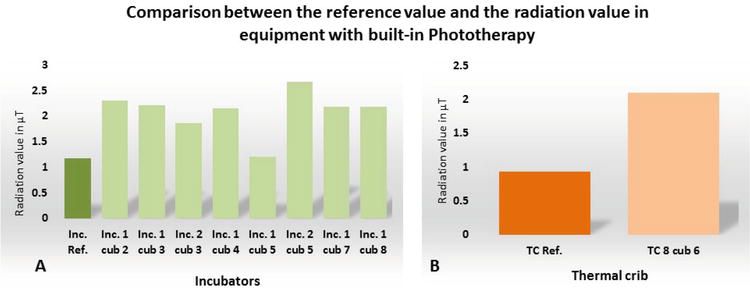
Figure 10.
Comparison graphs of electromagnetic radiation with application of phototherapy in incubator (A) and thermal cradles (B).
If the values obtained for electromagnetic radiation are compared with respect to the reference standards (Inc. Ref. and CT Ref.), it can be seen in the graphs of Figures 9 and 10 that, except for incubator 2 of cubicle 2 (Inc. 2 cub. 2) and incubator 3 of cubicle 5 (Inc. 3 cub. 5), which do not have incorporated light treatment, the rest have values above the reference. This issue can be attributed to the presence in its surroundings of other equipment used in the treatment of the baby. This shows that electromagnetic radiation, being invisible, is not taken into account for diagnostic treatment in incubators and the application of phototherapy treatment.
Incubators and thermal cribs are quintessential equipment for exclusive use in NICUs. It is known that they provide the preterm newborn with comfort and safety, but incubators are electrical equipment that provide electromagnetic fields and this, in turn, exerts influences on body parameters responsible for maintaining the physiological safety of the newborn.
When using phototherapy on a baby who is in an incubator, you are providing photonic radiation, which emits a level of electromagnetic radiation that, in turn, is accompanied by a level of non-ionizing radiation provided by the electrical components they have the same.
The International Commission for Non-Ionizing Radiation Protection (ICNIRP) maintains a research protocol on non-ionizing radiation that leads to modifying from time to time the recommendations regarding the levels of radiation that can be absorbed by humans, without causing physiological or cellular damage [23].
Electromagnetic fields are waves of energy that exert their effect on the medium they pass through. The ability they have to alter temperature, change polarity, and transform metallic compounds of the periodic table are the tools that are attributed to say that these are capable of causing damage at a physiological and cellular level, especially in the stage where the child is most vulnerable trying to adapt to the postnatal transition. These damages are based on scientific research [24], stating hypotheses such as:
Appearance of childhood leukemia in the first decade of life, this statement is based on research carried out, in vitro and in vivo. Leukemia is a disease characterized by arrest in the maturation of the cells responsible for the formation of blood constituents, with proliferation and uncontrolled growth of immature blood cells. This proliferation originates at the level of the bone marrow, from which it spreads to the blood and different tissues. If a child receives electromagnetic radiation during the first days of life where the organs are trying to balance the differences between the prenatal and postnatal environment, completion of that maturation may not occur or may occur very slowly. This is because EMFs act on cell membranes by distorting signals from the outside, which are directed to the organelles inside the cell, including the nucleus [25]. This could modify the electrochemical balance of the cells, affecting protein synthesis and causing a distortion of the bioelectric functions of the organism and changes in genetic transmission; which suggests their possible relationship with the development of different types of cancer [26] and alterations in the cellular ionic level caused by the influence of the polarization they induce on the cell membrane.
Chronic immunology problems and the appearance of different types of cancer before adulthood. Neonates are the most vulnerable people to receive these damages because they are in a stage of development where they do not have the defenses that the mother’s womb could provide. It is known that melatonin is the hormone par excellence that regulates sleep cycles and the immune system. It is also an efficient fighter against free radicals that generate cancer cells [27, 28]. This is produced during the part of the day when darkness reigns, and the sun’s electromagnetic radiation is attenuated due to the distance between it and the position in which the person is located. In a neonate, there is almost no generation of this hormone in the first weeks of birth, and the body is dedicated to spending the reserves generated by the mother during pregnancy [29, 30]. As long as the child receives electromagnetic radiation through any means in the circadian sleep cycle, melatonin generation does not occur or is deficient, so it cannot fulfill the functions for which it is intended and can cause long-term damage in this regard.
5.4 Recommendations about the use of light in a NICU
The recommendations proposed are aimed at both the use of light for treatment and the use of light in the environmental environment:
The effectiveness of phototherapy depends on the absorption of light photons by bilirubin molecules [31]. Bilirubin has a yellow pigment, so blue light is the most recommended because bilirubin molecules absorb light photons of this wavelength better than any other. It is recommended to only use blue light, in case of high bilirubin levels, spaced during the day and not at night.
Although white light has 35% blue and green light in its composition [8], it does not achieve the effectiveness of blue light, so treatment with this type of light, although it may have an effect, would over a long period of time (taking into account that it is only recommended during the day) and the child would be exposed for a prolonged period to the effect of electromagnetic radiation that could cause long-term damage to his or her health.
The recommended distance for placing the lamps on the RN is 20 to 30 cm. It is requested that review this existing recommendation in the phototherapy protocol because light lamps are magnetic field emitters whose installation standard proposes a minimum distance of 1.5 m from people.
It is recommended to place lamps in each position occupied by an incubator or thermal crib, so that, if it is necessary to turn them on at night, they do not affect the sleep of other babies.
If fluorescent lamps are used for general lighting, they must be replaced from time to time to avoid a decrease in visibility when required.
For general lighting, the use of LED lamps is recommended due to their long life in terms of hours (30,000) and the advantage of not producing heat, which gives them the superiority of increasing irradiance.
The use of light in a neonatal intensive care unit is of vital importance for the care of preterm neonates.
Taking into account the characteristics of the composition of visible light is a premise for the efficient use of phototherapy in newborns with conditions at birth.
Keep in mind that artificial light, although it is a tool whose operation depends on electrical energy, is vital for the subsequent state of health of children born with conditions; it provides invisible risks that affect their subsequent development.
1.Rodríguez RG, Pattini AE. Iluminación en unidades de cuidados intensivos neonatales: actualización y recomendaciones. Archivos Argentinos de Pediatría. 2016;114(4):361-367. DOI: 10.5546/aap.2016.361
2.Soto Conti CP. Bilirrubina: mecanismos tóxicos de una molécula antioxidante. Archivos Argentinos de Pediatría. 2021;119(1):e18-e25. DOI: 10.5546/aap.2021.e18
3.Duran M, García JA, Sánchez A. Efectividad de la fototerapia en la hiperbilirrubinemia neonatal. Enfermería Universitaria. 2015;12(1):41-45. DOI: 10.1016/j.reu.2015.05.006
4.Gabàs MJ. Maxwell: la teoría electromagnética de la luz. Arbor. 2015;191(775):a265. DOI: 10.3989/arbor.2015.775n500
5.Henao Robledo F. In: ECOE Ediciones, editor. Riesgos Físicos II: Iluminación. In: Colección Ingeniería y salud en el trabajo. 2nd ed. 2014. p. 234 consultado en Abril de 2023. Available from: https://books.google.co.ve/books?id=8MK4DQAAQBAJ&printsec=frontcover&hl=es#v=onepage&q&f=false
6.del Mazo VA, Velasco Maillo S, García-Molina R. Recomposición de un rayo de luz blanca descompuesto por un prisma. Eureka sobre Enseñanza y Divulgación de las Ciencias. 2020;17(3):340201-340209 https://doi.org/10.25267/Rev_Eureka_ensen_divulg_cienc.2020.v17.i3.3402
7.Mosquera Torres AM, Basto Guevara JA, Reyes Domínguez JF. La popular luz azul: ¿por qué es nociva para la salud visual? Ámbito Investigativo. 2020;5(2):72-80. Available from: https://ciencia.lasalle.edu.co/ai
8.Boulton ME, Brainard GC, Jones W, Karpecki P, Melton R, Thomas R. Blue light hazard: New knowledge, new approaches to maintaining ocular health. In: Points de Vue - International Review of Ophthalmic Optics; Report of a roundtable 16 march 2013. New York city, USA: Essilor International; 2015. pp. 2-12. Available from: www.ko-go.org.tr
9.Jiménez-Rubio G, Solís-Chagoyán H, Domínguez-Alonso A, Benítez-King G. Alteraciones del ciclo circadiano en las enfermedades psiquiátricas: papel sincronizador de la melatonina en el ciclo sueño-vigilia y la polaridad neuronal. Salud Mental. 2011;34:167-173. Available from:https://www.scielo.org.mx/scielo.php?script=sci_arttext&pid=S0185-33252011000200010
10.Jeffrey MM, AF MD. Fototerapia para la ictericia neonatal. Revista del Hospital Materno Infantil Ramón Sardá. 2008;27(3):100-111. Available from:https://www.redalyc.org/articulo.oa?id=91227302
11.Sadowska M, Narbutt J, Lesiak A. Blue light in dermatology. Life. 2021;11(7):670. DOI: 10.3390/life11070670
12.Ruiz Sánchez JG, de León FB, González Pérez-de Villar N, Gomes Porras M, Herranz de la Morena L. Niveles de bilirrubina como predictor favorable en la diabetes mellitus Tipo 2. In: XXIX Congreso Nacional De La Sociedad Española De Diabetes, Oviedo, 18-20 de abril de 2018. Endocrinología, Diabetes y Nutrición. 2018;65(Espec Cong 1):79. Available from: https://static.elsevier.es›congresos ›pdf›cong_sed2018
13.Slaughter JL, Kemper AR, Newman TB. Technical report: Diagnosis and management of hyperbilirubinemia in the newborn infant 35 or more weeks of gestation. Pediatrics. 2022;150(3):e2022058865. DOI: 10.1542/peds.2022-058865
14.Faulhaber FRS, Procianoy RS, Silveira RC. Side effects of phototherapy on neonates. American Journal of Perinatology. 2019;36(3):252-257. DOI: 10.1055/s-0038-1667379
15.Newman TB, Wu YW, Kuzniewicz MW, et al. Childhood seizures after phototherapy. Pediatrics. 2018;142(4):e20180648. DOI: 10.1542/peds.2018-0648
16.Boidi, del artículo C. Efectos secundarios de la luminoterapia en neonatos. Revista Enfermería Neonatal. 2019;31:38-42. Available from:https://riu.austral.edu.ar/handle/123456789/1016
17.García del Río M, Sánchez Luna M, Doménech Martínez E, et al. Revisión de los estándares y recomendaciones para el diseño de una unidad de neonatología. Anales de Pediatría (Barcelona, Spain). 2007;67(6):594-602. DOI: 10.1016/S1695-4033(07)70810-X
18.de la Rosa Castillo MJ. Análisis de los cambios de coloración cuantificados por colorimetría en la piel de recién nacidos expuestos a fototerapía. Tesis para obtener el diploma de la Especialidad en Pediatría. San Luis Potosí: Universidad Autónoma de San Luis Potosí; 2020
19.Pickler R, McGrath J, Reyna B, Tubbs-Cooley H, Best AI, et al. Effects of the neonatal intensive care unit environment on preterm infant oral feeding. Research and Reports in Neonatology. 2013;2013(3):15-20. DOI: 10.2147/RRN.S41280
20.Riad SM, Salama IM. Electromagnetic Fields and Waves Fundamentals of Engineering. McGraw-Hill Education; 2020. p. 688 consultado en mayo de 2023. Available from: https://www.mhprofessional.com/electromagnetic-fields-and-waves-fundamentals-of-engineering-9781260457148-usa
21.Council of the European Union. Council Recommendation of 12 July 1999 on the Limitation of Exposure of the General Public to Electromagnetic Fields (0 Hz to 300 GHz). Brussels, Belgium: Official Journal of the European Communities; July 1999
22.International Agency for Research on Cancer (IARC). Non-ionizing Radiation, Part 1: Static and Extremely Low-frequency (ELF) Electric and Magnetic Fields. In: IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Vol. 80. Lyon, France; 2002. p. 445 ISBN 92 832 1280 0
23.ICNIRP. Guidelines for limiting exposure to time-varying electric and magnetic fields (1 Hz - 100 kHz). Health Physics. 2010;99(6):818-836. DOI: 10.1097/HP.0b013e3181f06c86
24.Moon JH. Health effects of electromagnetic fields on children. Clinical and Experimental Pediatrics. 2020;63(11):422-428. DOI: 10.3345/cep.2019.01494
25.Brabant C, Geerinck A, Beaudart C, Tirelli E, Geuzaine C, Bruyere O. Exposure to magnetic fields and childhood leukemia: A systematic review and meta-analysis of casecontrol and cohort studie. Reviews on Environmental Health. 2021;38(2):1-12. DOI: 10.1515/reveh-2021-0112
26.Seomun G, Lee J, Park J. Exposure to extremely low-frequency magnetic fields and childhood cancer: A systematic review and meta-analysis. PLoS One. 2021;16(5):e0251628. DOI: 10.1371/journal.pone.0251628
27.Reiter RJ, Manchester LC, Dun-Xian T. Neurotoxins: Free radical mechanisms and melatonin protection. Current Neuropharmacology. 2010;8(3):194-210. DOI: 10.2174/157015910792246236
28.Hacışevki A y Baba B. An overview of melatonin as an antioxidant molecule: A biochemical approach. In: Melatonin Drăgoi CM, Nicolae AC, editors. Intech Open; 2018. DOI:10.5772/intechopen.79421
29.Carvajal de la Osa J, Santana GJ, Herrera GM, Sánchez GA, Pérez Almirall I. Campo magnético ambiental en una Unidad de Terapia Intensiva Neonatal. Importancia de su verificación. Archivos Argentinos de Pediatría. 2020;118(3):e246-e251. DOI: 10.5546/aap.2020.e246
30.Muñoz Hoyos A, Bonillo Perales A, Ávila-Villegas R, González-Ripoll M, et al. Melatonin levels during the first week of life and their relation with the antioxidant response in the perinatal period. Neonatology. 2007;92(3):209-216. DOI: 10.1159/000102957
31.Ávila Reyes R, Suárez Llanas BA, Pérez Abrego CE, Masud Yunes-Zárraga JL, et al. Luz emitida por diodo (LED) en el tratamiento de la hiperbilirrubinemia neonatal. Un prototipo de fototerapia a bajo costo hecho en México. Pediatría de México. 2013;15(3):73-79. Available from: https://1library.co/document/dzx1e4oy-emitida-diodo-tratamiento-hiperbilirrubinemia-neonatal-prototipo-fototerapia-mxico.html
Written By
Janet Carvajal de la Osa, Yenisel Díaz Roller and Iosvany Aguiar Ramos
Submitted: 03 August 2023Reviewed: 20 September 2023Published: 12 March 2024