
Abstract
Regional anesthesia for foot surgery has become increasingly popular, there are different reasons including: most surgeries are ambulatory, great pain management during the early postoperative phase, reduced time spent in the post-anesthesia care unit, and minimizing opioid use during the perioperative period are achieved through effective ankle blockade. This procedure involves blocking the five nerves responsible for sensory supply to the area below the malleoli. It can be used both as an anesthetic technique (used together with general or neuraxial anesthesia), as well as analgesia in the context of multimodal analgesia providing adequate post-operative analgesia. All five nerves can be blocked using ultrasonography, allowing for lower latency and a smaller volume of local anesthetic.
Keywords
- anesthesia
- ultrasonography
- nerve block
- ankle
- tibial nerve block
- peroneal nerve block
- sural nerve block
- saphenous nerve block
- regional anesthesia
1. Introduction
Regional anesthesia for foot surgery has become increasingly popular, there are different reasons including: most surgeries are ambulatory, great pain management during the early postoperative phase, reduced time spent in the post-anesthesia care unit, and minimizing opioid use during the perioperative period [1, 2, 3]. Foot surgery is a common procedure, and the patient population undergoing it represents a cross-section of society.
Foot surgery presents a challenge due to the intense postoperative pain, which is often difficult to manage despite employing balanced multimodal analgesia involving medications like paracetamol, non-steroidal-anti-inflammatory drugs (NSAIDs), and opioids [4]. The acute postoperative pain persists considerably beyond 24 hours [5]. After forefoot surgery, approximately 80% of patients endure severe pain, and about 32% experience nausea during the postoperative phase [6]. A majority of patients necessitate high doses of opioids for pain management following foot and ankle surgery [7].
The ankle block plays a pivotal role in multimodal analgesia, in many feet surgical procedures, the performance of this block is considered the first-option regional analgesic technique [8].
The recently adoption of enhanced recovery and ambulatory programs after fast-track orthopedic surgery protocols has sparked a renewed interest in ankle blocks [9].
Foot surgery typically involves regional anesthesia, commonly through a distal Sciatic Nerve block, occasionally complemented by a Saphenous Nerve block. These procedures may be conducted as single-shot injections or via catheter placement for continuous delivery of anesthesia [10]. The primary issue associated with the distal Sciatic Nerve block is its impact on motor function. This motor block leads to weakness in knee movement and foot mobility, potentially resulting in a higher risk of ankle sprains and inpatient falls. Difficulty in walking unassisted may prolong hospital stays or hinder prompt ambulation [11]. And therefore, delays postoperative mobilization, which is important in the context of ambulatory patients and when bilateral procedures are required [12]. Postoperative pain management using oral NSAIDs or opioids could potentially be harmful to organs and might have a negative impact on bone healing [13, 14, 15]. The existing perioperative pain management approaches for ankle and hindfoot surgeries may not always align with the fundamental principles of contemporary perioperative pain therapy, which involve ensuring efficient pain relief throughout the perioperative phase, facilitating early patient mobilization, and reducing adverse effects [16].
The ankle block entails blocking the five nerves responsible for sensory innervation to the area distal to the malleoli. It serves as an anesthesia method for foot surgery, provided a pneumatic tourniquet is not utilized during the procedure. Alternatively, it can be combined with general or neuraxial anesthesia to ensure sufficient analgesia in the postoperative phase [17]. If a tourniquet is required for the procedure, it is also proposed to use it at the ankle level, with good tolerance when ankle block is used as the sole anesthetic technique [18]. This approach minimally impacts motor function as it primarily targets the intrinsic muscles of the foot. Moreover, the use of long-acting local anesthetics enables extended postoperative analgesia [19].
Traditionally, the Ankle block has been conducted using landmark guidance, but there is a growing preference for ultrasound guidance [11]. These blind superficial infiltrations were very painful for the patient due to the need for high volumes of local anesthetics. In contrast, ultrasound-guided injections, unlike landmark-guided procedures relying on field infiltration, reduce discomfort associated with ankle block and enhance success rates [11].
The anatomical landmarks technique has reported high success rates (89–100%) [20, 21]; however, it has been perceived as technically challenging and unreliable. Various anatomical variations among the nerves could result in failure when employing a blind technique [22]. Additionally, it frequently encounters failure due to two primary reasons: first, a lack of comprehensive understanding regarding the fascial layers and the positioning of the five nerves relative to these fascias around the ankle; second, physicians occasionally overlook the necessity of blocking all five nerves, disregarding the fact that the sensory innervation areas of the foot partially overlap, and this overlap is not consistently predictable [23].
2. Indication (patient selection)
Anesthesia and pain management for surgical procedures involving the foot distal to the malleoli, particularly focusing on the forefoot, encompassing surgeries such as hallux valgus repair, forefoot arthroplasty, reconstruction, osteotomy, and amputation [24].
Perineural injections targeting the nerves around the foot and ankle may be proposed either for diagnostic purposes or as therapeutic interventions for individuals experiencing neuropathic pain, especially in cases involving peripheral nerve damage or entrapment [24].
For ankle surgeries, there is limited research on the effectiveness of local intraoperative infiltration. While some studies have demonstrated its efficacy in postoperative pain management, it does not provide intraoperative pain relief or eliminate the need for general anesthesia [25, 26]. Conversely, ankle block is a widely recognized regional anesthesia method for surgeries below the ankle [17, 27]. However, it is not suitable for procedures directly involving the ankle joint as the relevant nerve fibers exit their nerve roots 5–10 cm above the ankle joint.
The ankle block primarily involves infiltration and does not necessitate the elicitation of paresthesia; thus, patient cooperation is not mandatory. While it is most efficient for the anesthesiologist if the patient can assume both prone and supine positions, this is not essential [28].
Comparing ultrasound-guided and anatomical point techniques for ankle block, ultrasound has been shown to enhance clinical effectiveness, providing greater surgical anesthesia, reducing systemic opioid rescue requirements, and lowering total opioid doses in the postoperative period [29].
3. Contraindication
4. Anatomy
The sensory innervation below the malleoli originates from five nerves: the tibial, superficial peroneal, deep peroneal, sural, and saphenous. These nerves are all derived from the sciatic nerve, except for the saphenous nerve (which is the terminal sensory branch of the femoral nerve) [11].
Blood vessels accompany the deep peroneal, posterior tibial, saphenous, and sural nerves, providing valuable anatomical landmarks for ultrasound-guided approaches (Figure 1) [30]. The sensory innervation regions corresponding to each nerve in the foot are illustrated in (Figure 2) [30]. While it has been suggested that the saphenous nerve may be necessary in only 3% of patients undergoing foot surgery [23], it is recommended to perform a complete block rather than a selective one, regardless of the type of surgery, due to frequent overlap in nerve territories [17].
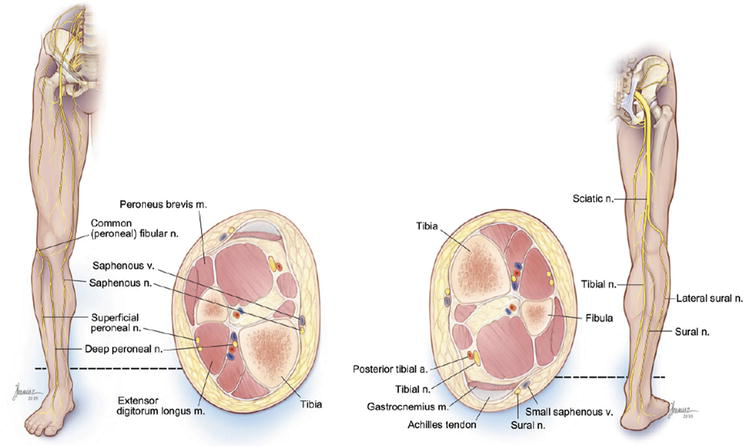
Figure 1.
Image of the anterior and posterior leg showing the course of the nerves as well as a cross section of the leg showing the location of the nerves in relationship to arteries, veins, muscles, and bones. The tibia is medial and anterior, and the fibula is lateral. Source: Ref. [
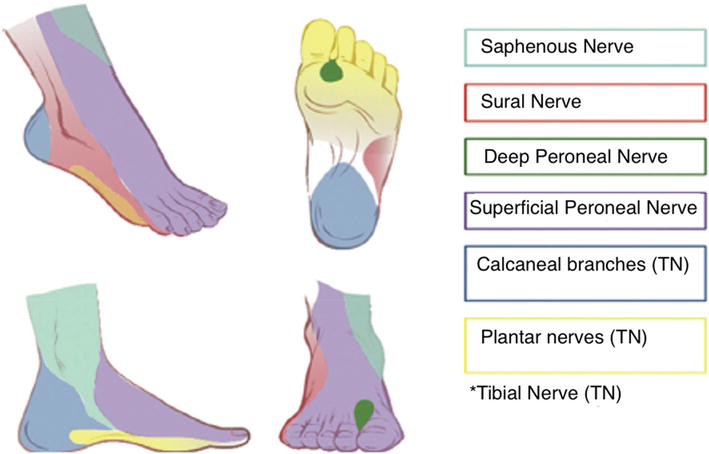
Figure 2.
Ankle block—Peripheral innervation. Source: Ref. [
4.1 Tibial nerve
This nerve exhibits mixed characteristics, encompassing both sensory and motor functions. It holds the distinction of being the largest nerve among the group of five nerves responsible for innervating the foot [31]. This nerve supplies sensation to the entire bottom surface (both bones and skin) of the foot, as well as the top surface of the first phalanx of the first, second, and half of the third toe [32]. In the ankle region, it is a direct extension of the tibial nerve beyond the point where the sciatic nerve splits in the popliteal fossa. Descending through the calf, it lies between the gastrocnemius/soleus muscles and the deep flexors. As it continues down the leg, it passes posterior to the medial malleolus and beneath the flexor retinaculum, typically located behind the artery. It sends branches to the medial heel (medial calcaneal branches) and eventually divides into two terminal branches: the medial and lateral plantar nerves, which innervate the sole of the foot, providing its sensory supply (Figure 3) [21].
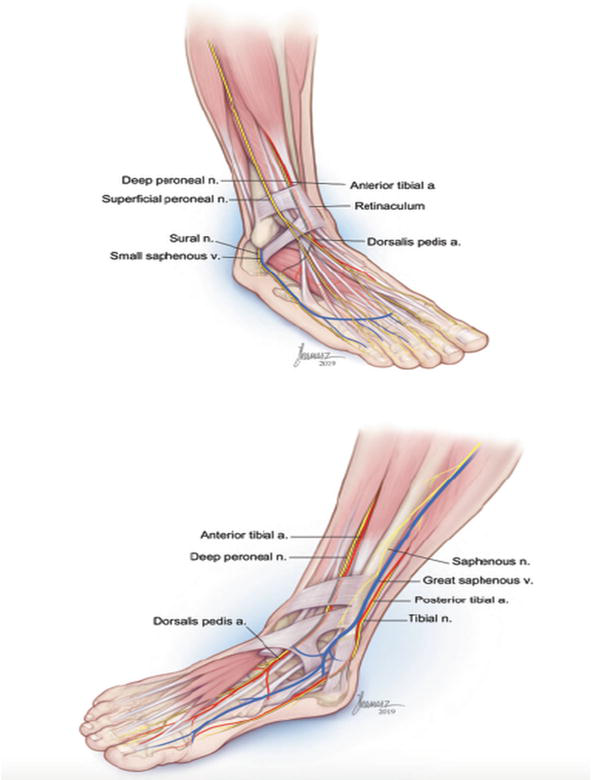
Figure 3.
Image of the lateral and medial ankle showing the course of the nerves in relationship to arteries and veins. Source: Ref. [
4.2 Superficial peroneal (fibular) nerve
This nerve originates from the common peroneal (fibular) nerve and traverses through the peroneus longus muscle before coursing between the peroneus longus and brevis muscles. In the lower leg, it travels between the peroneus brevis and extensor digitorum longus (EDL) muscles, within the intermuscular septum that separates the anterior and lateral compartments of the leg. Its trajectory gradually shifts to a more superficial position as it progresses, ultimately piercing the crural fascia. At a subcutaneous or subfascial level, it divides into two branches: the larger medial dorsal cutaneous nerve and the smaller intermediate dorsal cutaneous nerve. These branches provide sensory innervation to the skin on the dorsal aspect of the foot and toes, covering a significant portion of the foot’s dorsal surface (Figure 3) [24].
4.3 Deep peroneal (fibular) nerve
The deep peroneal nerve, a branch of the common peroneal nerve, originates at the fibular neck, paralleling the path of the superficial peroneal nerve. This nerve runs between the tibialis anterior muscle and the extensor hallucis longus (EHL) muscle toward the ankle, where it divides into medial and lateral branches. The medial branch continues its course alongside the dorsalis pedis artery to the first interosseous space. Passing beneath the extensor hallucis brevis tendon, it extends to the distal end of the interosseous space, where it merges with a strand of the superficial peroneal nerve (SPN) before branching into terminals for the dorsal surfaces of the first and second toes, although anatomical variations exist [33].
Conversely, the lateral branch turns outward to innervate the extensor digitorum brevis muscle, giving rise to three interosseous nerves. It supplies sensation to the area between the first and second toes, the lateral aspect of the first toe, and the medial aspect of the second toe, in addition to providing innervation to the bones on the dorsal side of the foot (Figure 3) [24].
4.4 Sural nerve
This nerve is formed from branches of both the tibial nerve and the common peroneal nerve at the junction of the gastrocnemius in the upper third of the calf. Specifically, the medial sural cutaneous nerve emerges in the proximal part of the popliteal fossa, descending between the two heads of the gastrocnemius muscle. It then combines with the peroneal communicating branch (lateral sural nerve) to create the sural nerve. Traveling alongside the small saphenous vein, the sural nerve passes behind the lateral malleolus within the same superficial fascial sheath. Continuing as the lateral dorsal cutaneous nerve along the lateral aspect of the foot, it sends a connecting branch to the intermediate dorsal cutaneous nerve. Ultimately, it terminates as the dorsalis digiti minimi nerve on the lateral edge of the dorsum of the small toe (Figure 3).
Behind the lateral malleolus, it branches into the lateral calcaneal branches, providing sensory supply to the skin in that area and at the heel. Additionally, branches for the lateral side of the ankle, the anterior capsular wall, and the tarsal sinus originate proximal to the malleolus [24].
It offers sensory innervation to the lateral aspect of the heel, the outer malleolus, and the dorsal side of the 5th and 4th toes, often extending to the 3rd toe (Figure 3) [34].
4.5 Saphenous nerve
The saphenous nerve is distinctive in its origin from the lumbar plexus, serving as the terminal branch of the femoral nerve. Below the knee, it runs along the tibial surface in close proximity to the great saphenous vein. The positioning of the nerve relative to the vein may vary, with the nerve situated either posteriorly or anteriorly to the vein. In the distal third of the calf, a common fascia encloses both the vein and the nerve. As it descends into the lower leg, the saphenous nerve follows a path along the medial side and anterior to the medial malleolus, emitting branches to the skin of the medial aspect of the foot. Typically, it ends in the metatarsal area without extending to the big toe. Providing sensory innervation to the medial part of the ankle and foot, it extends up to the head of the first metatarsal [32]. The extent of skin innervation may vary, with an average distance of 6.5 cm from the medial malleolus, though it may exceed 9 cm in certain cases .
There are reports of the saphenous nerve reaching deep to the periosteum of the distal tibia, the capsule of the medial malleolus in the ankle joint, and in some instances, the capsule of the talocalcaneonavicular junction in the medial area (Figure 3) [35].
5. Technique—Ultrasound-guided approach
5.1 Preparation for the block
Prior to the procedure, it is imperative to provide comprehensive information to the patient. Since the nerves are located superficially, a 25–50 mm 25-G needle should be sufficient [24]. The patient can be positioned supine with a footrest or pillow under the calf. During the block, the leg may need to be rotated internally or externally depending on the nerve being targeted. The proceduralist may find it efficient to maneuver around the foot while performing the block. The entire foot should be thoroughly cleaned, and the procedure must be conducted using sterile technique [28].
A high-frequency linear ultrasound probe is employed, starting at a depth of 2 cm. Long-acting local anesthetics such as 0.5–0.75% ropivacaine, 0.25–0.5% bupivacaine, or a combination of 2% lidocaine and 0.5% bupivacaine in a 1:1 ratio are utilized [24].
Regarding the volume of local anesthetic, a recommended volume of 5 ml is advised for each nerve, except for the tibial nerve, for which a volume of 5–10 ml is used due to its larger size. The literature generally advocates for a total volume ranging between 30 and 40 ml [12, 17, 23, 29]. With respect to the approach, for the five nerves a technique can be performed outside or inside the plane, recommendations varying among literature based on authors’ experiences [12, 31].
This total volume aligns closely with the volume used in ankle block procedures for anatomical issues. Fredrickson et al. [36] studied 72 patients undergoing foot surgery who received ankle blocks. They were divided into two groups: one using a low volume of local anesthetic (approximately 16 ml) and the other using the conventional total volume (30 ml). The authors concluded that while a low volume resulted in a high success rate compared to the conventional volume, there might be a compromise in the duration of postoperative analgesia.
5.2 Sonoanatomy and injection technique
5.2.1 Tibial nerve
The patient is positioned supine with the hip externally rotated, allowing the medial side of the ankle to face upward. Placing the ultrasound probe in a transverse orientation between the medial malleolus and the Achilles tendon (Figure 4) facilitates visualization. The primary landmark for this procedure is the posterior tibial artery, often accompanied by two venae comitantes. The tibial nerve is visualized as a hyperechoic structure, typically located behind the artery and resting on the fascia of the flexor hallucis longus (FHL), although occasional anterior placement is possible. To aid in identification, the tibial nerve can be observed moving up and down by extending and flexing the big toe, as demonstrated in Figure 5. Performing this block proximal to the prominence of the medial malleolus is recommended to ensure sufficient blockade of the calcaneal branch [37].

Figure 4.
Position of the patient and the transducer for tibial nerve block. Source: Authors.
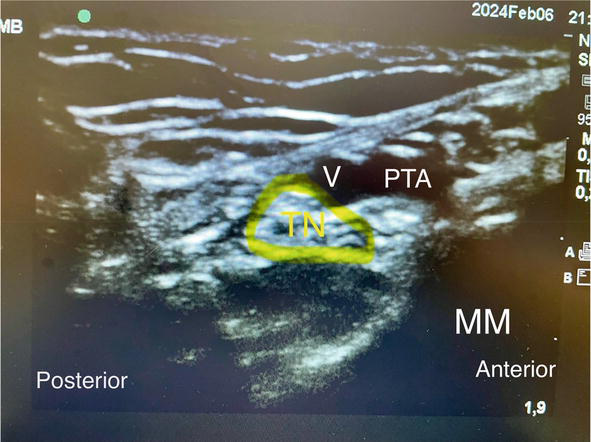
Figure 5.
Sonography of the tibial nerve at the level of medial malleolus (MM). From anterior to posterior, the structures are tibialis posterior tendon (TP), flexor digitorum, posterior tibial artery (A) and veins (V), tibial nerve (TN). Source: Authors.
Care should be taken to differentiate the flexor hallucis longus tendon, which lies deep to the tibial nerve and may be mistaken for a nerve structure due to similar sonoanatomical characteristics [30].
Both the in-plane and out-of-plane needle approaches to the nerve are viable options. The nerve is enveloped within a fascial sheath, and injecting the local anesthetic within this sheath leads to a distinctive circumferential spread of the anesthetic around the nerve. The author prefers the in-plane technique, guiding the needle into the space behind the nerve created between the flexor retinaculum and the fascia of the flexor hallucis longus. Typically, 8 to 10 ml of local anesthetic is adequate to achieve a satisfactory block.
In a study by Redborg et al. [38], a prospective randomized controlled trial was conducted involving 18 healthy volunteers. This study investigated the efficacy of the anatomical landmark technique versus the ultrasound-guided technique for tibial nerve block. The findings revealed a greater proportion of complete blocks at 30 minutes with ultrasound guidance (72% vs. 22%).
5.2.2 Saphenous nerve
The patient is positioned with the hip externally rotated, and the transducer is placed proximal to the medial malleolus, aligning with the position used for tibial nerve scanning (Figure 6) . The probe is gently positioned just above the medial malleolus in the approximate location of the greater saphenous vein. While the saphenous nerve, a small hyperechoic structure, may not always be clearly visible and does not consistently relate to the vein, the great saphenous vein serves as a reference point (Figure 7). In cases where the saphenous nerve is not visualized, a tourniquet can be applied around the calf to enhance venous filling (Figure 8).

Figure 6.
Patient position and transducer for saphenous nerve block. Source: Authors.
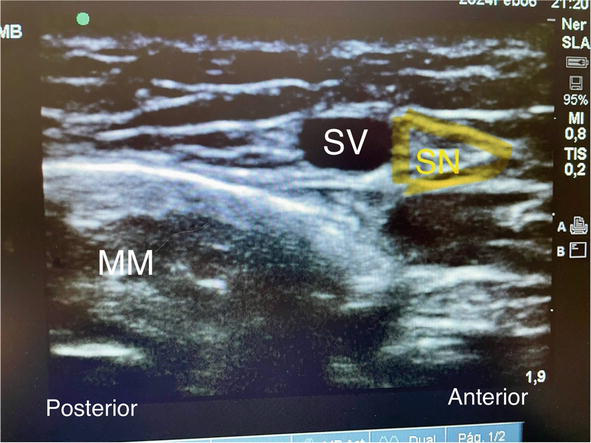
Figure 7.
Sonography of the saphenous nerve (SN) at the level of medial malleolus. It lies within the same fascia plane with the greater saphenous vein (SV). Source: Author.

Figure 8.
A tourniquet can be placed around the calf to enhance the venous filling. Source: Author.
During injection, the saphenous nerve may appear as a small hyperechoic structure superficial and posterior to the great saphenous vein. However, its visibility can vary, and in such instances, the primary landmark is the vein, and light pressure should be applied with the ultrasound probe [39]. The target area is the plane around the vein, and the needle can be inserted either in-plane or out-of-plane. Usually, a volume of 3–5 ml of local anesthetic is administered.
5.2.3 Deep peroneal (fibular) nerve
The patient is positioned supine with the leg in a neutral position. The ultrasound probe is placed transversely on the anterior surface of the ankle at the intermalleolar line, which is proximal to the ankle joint (Figure 9). The primary landmark for this procedure is the anterior tibial/dorsalis pedis artery, typically located deep to the extensor hallucis longus. While the deep peroneal nerve (DPN) may sometimes appear as a small hyperechoic structure lateral to the artery in the same tissue plane, its visualization is not essential for performing the block. The main purpose of visualizing the nerve is to avoid inadvertently puncturing it with the block needle (Figure 10), as surrounding the artery with local anesthetic ensures nerve blockade [24].

Figure 9.
Patient position and transducer for deep peroneal (fibular) nerve block. Source: Authors.

Figure 10.
Ultrasound still of the deep peroneal nerve and surrounding anatomy. Sonography of deep peroneal (fibula) nerve (DPN) at the low tibia area. The nerve is seen lateral to the anterior tibial (dorsalis pedis) artery (ATA) which is deep to the extensor digitorum longus (EDL). Source: Authors.
Both in-plane and out-of-plane needle approaches can be employed, with the out-of-plane approach offering a more direct needle entry for a superficial nerve. The needle tip should be directed to either side of the artery, and local anesthetic should be injected to distend the plane in which the artery lies. Care should be taken not to apply excessive pressure on the transducer, as this may occlude the artery and hinder adequate visualization. Typically, 3–5 ml of local anesthetic is adequate for achieving effective blockade.
Antonakakis et al. [40] conducted a prospective, randomized, controlled study involving 18 healthy volunteers to compare the technique for anatomical landmark-based blocks with the ultrasound-guided technique for deep peroneal nerve blockade. The authors concluded that although the use of ultrasound for deep peroneal nerve block reduced latency times, it did not improve the quality of the final block compared to the conventional technique using anatomical landmarks.
5.2.4 Superficial peroneal (fibular) nerve
With the patient in the supine position, the knee is flexed and the hip is internally rotated to facilitate access to the lateral aspect of the leg. Alternatively, the patient can be positioned in the lateral decubitus position, with the procedural side facing upward (Figure 11). The ultrasound (US) probe is placed transversely on the lateral aspect of the mid-leg, positioned above the subcutaneous part of the fibula. The fibula serves as the anatomical reference point, generating a rectangular echo. The superficial peroneal nerve is visualized as a small triangular hyperechoic structure situated within the intermuscular septum between the peroneus brevis and extensor digitorum longus muscles, just beneath the crural fascia (Figure 12). Its identity can be confirmed by moving the probe distally and observing the nerve emerging through the crural fascia, eventually becoming more prominent in a superficial location [41, 42].

Figure 11.
Patient position and transducer for superficial peroneal (fibular) nerve block. Source: Authors.
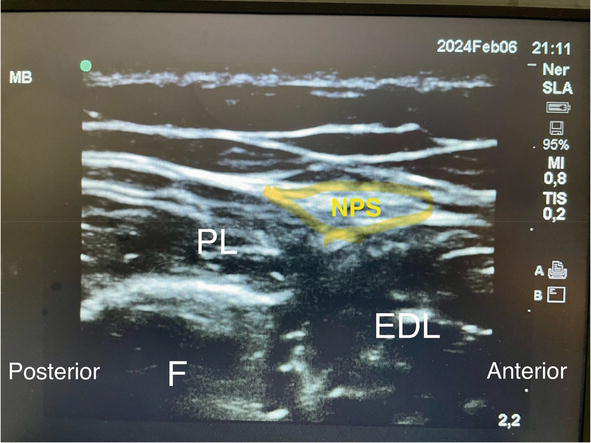
Figure 12.
Sonography of the superficial peroneal (fibula) nerve (NPS) at the distal third of the leg. The NPS is seen in the intermuscular septum between peroneus longus (PL) and extensor digitorum longus (EDL) deep to the crural fascia. Source: Authors.
The nerve can be blocked at the point where it lies superficial to the crural fascia, using either an in-plane or out-of-plane approach. The in-plane approach is typically preferred as it allows for easier needle entry into the narrow fascial plane. A volume of 5 ml of local anesthetic is generally sufficient to achieve a satisfactory block.
5.2.5 Sural nerve
The patient is positioned in the lateral decubitus position with the knee flexed and the hip internally rotated. The ultrasound probe is positioned transversely across the groove between the lower fibula (lateral malleolus) and the Achilles tendon (Figure 13), applying minimal pressure to prevent compression of the lesser saphenous vein. Both the vein and the nerve are situated within the fascial plane between the peroneus tendon and Achilles tendon (Figure 14). The sural nerve is observed as a small, round hyperechoic structure located adjacent to the lesser saphenous vein within the same fascial subcutaneous plane. If the sural nerve is not immediately visible, the peroneal sheath can be located, with the nerve typically found anteriorly and outside it. Another method to aid in visualizing the sural nerve is to apply a tourniquet to the upper third of the leg to distend the small saphenous vein and facilitate locating the nerve (as shown in Figure 15) [30, 43].

Figure 13.
Patient position and transducer for sural nerve block. Source: Authors.
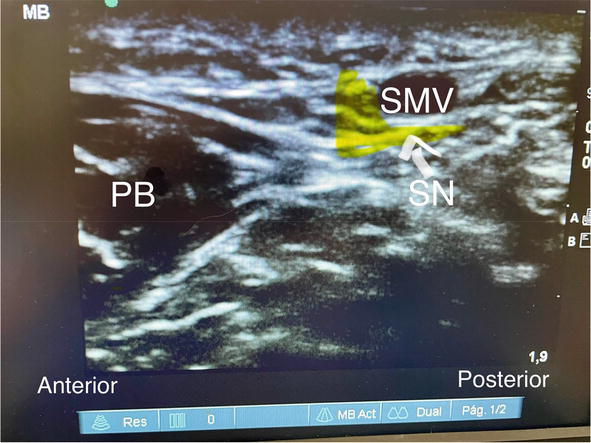
Figure 14.
Sonography of the sural nerve (indicated by line arrow). It is accompanied by the lesser saphenous vein, and both are located within the fascia plane (block arrows) between the peroneus brevis (PB) muscle and tendon Achilles (TA). Source: Author.

Figure 15.
A tourniquet can be placed around the calf to enhance the venous filling. Source: Author.
The target for injection is the fascial expansion between the fibula and Achilles tendon. If the nerve remains elusive, local anesthetic can be injected around the vein. The nerve may be approached using either an in-plane or out-of-plane technique, with caution taken to avoid piercing the nerve itself. A volume of 3–5 ml of local anesthetic is then injected into the fascial plane surrounding the nerve.
In a study by Redborg et al. [43], a randomized, prospective, and blinded study was conducted with 18 healthy volunteers divided into two groups: one receiving sural nerve block guided by ultrasound and the other by anatomical landmarks. The study concluded that ultrasound-guided (USG) techniques produced a more comprehensive and longer-lasting block.
6. Conclusion
With the development of US we are enabled to perform very selective and precise nerve blocks. The primary clinical justification for employing ultrasound guidance lies in its capacity to pinpoint the precise location of the nerve, offer real-time visualization of the needle, and allow observation of the spread of local anesthetic, providing immediate feedback to the practitioner [44].
One of the best examples of the accuracy of this technology is the ankle block, small sensory end nerves, at the ankle level, can be identified and blocked using very low dose comparing with landmark techniques.
The ankle block is an effective regional technique, providing excellent intraoperative anesthesia as well as long postoperative pain relief in foot surgeries, the advantages are less motor block with similar analgesic effectiveness compared to sciatic block [45]. In the context of modern times, this holds greater significance in outpatient scenarios due to the implementation of enhanced recovery programs and fast-track orthopedic surgery protocols, which prioritize rapid patient mobility and discharge [9]. Some evidence suggests that the USG technique improves block success rates, facilitates faster block progression, without prolonging the procedure time [46].
7. Practical tips
When administering the ankle block, prioritize blocking the tibial nerve first, as it is the largest nerve and takes longer to achieve a full block onset [24].
During the superficial peroneal nerve block, begin scanning from a higher position when the nerve is deep to the crural fascia, and observe its emergence superficially. The nerve may be challenging to visualize in this location due to its smaller size and hypoechoic nature [24].
Visualizing the deep peroneal and saphenous nerves can pose challenges. However, by concentrating on the fascial plane that delineates the vessel, inject the local anesthetic within that plane. The sural nerve consistently resides within the fascial expansion between the peroneus and Achilles tendons [24].
Patients undergoing this block should be adequately sedated since it involves multiple needle insertions and superficial injections of local anesthetic, which can cause discomfort. Patient alertness is not crucial for the block [28].
When injecting local anesthetic to block superficial nerves, ensure the presence of a wheal to confirm correct placement of the needle in the superficial plane [28].
Both the posterior tibial and deep peroneal nerves are situated deep to the fascia [28].
Ankle block used for outpatient foot surgery enables most patients to walk with assistance, facilitating earlier discharge from the surgical center [28].
References
- 1.
Collins L, Halwani A, Vaghadia H. Impact of a regional anesthesia analgesia program for outpatient foot surgery. Canadian Journal of Anaesthesia. 1999; 46 :840-845 - 2.
Chelly JE, Greger J, Casati A, Al-Samsam T, McGarvey W, Clanton T. Continuous lateral sciatic blocks for acute postoperative pain management after major ankle and foot surgery. Foot & Ankle International. 2002; 23 :749-752 - 3.
Pearce CJ, Hamilton PD. Current concepts review: Regional anesthesia for foot and ankle surgery. Foot & Ankle International. 2010; 31 :732-739 - 4.
Stefani KC, Ferreira GF, Pereira Filho MV. Postoperative analgesia using peripheral anesthetic block of the foot and ankle. Foot & Ankle International. 2018; 39 :196-200 - 5.
Chaudier P, Bourdin M, Gauthier J, et al. Similar levels of pain are reported in forefoot surgery after management as a day case and admission for 48 hours: A continuous prospective study of 317 patients. The Bone and Joint Journal. 2015; 97-B :1645-1650 - 6.
Mouton A, Le Strat V, Medevielle D, et al. Patient's satisfaction after outpatient forefoot surgery: Study of 619 cases. Orthopaedics & Traumatology, Surgery & Research. 2015; 101 :S217-S220 - 7.
Merrill HM, Dean DM, Mottla JL, et al. Opioid consumption following foot and ankle surgery. Foot & Ankle International. 2018; 39 :649-656 - 8.
Korwin-Kochanowska K, Potié A, El-Boghdadly K, Rawal N, Joshi G, Albrecht E. PROSPECT/ESRA Working Group Collaboration. PROSPECT guideline for hallux valgus repair surgery: a systematic review and procedure-specific postoperative pain management recommendations. Regional Anesthesia and Pain Medicine. Sep 2020; 45 (9):702-708. DOI: 10.1136/rapm-2020-101479. Epub 2020 Jun 28. PMID: 32595141; PMCID: PMC7476301 - 9.
Marty P, Rontes O, Chassery C, et al. Perineural versus systemic dexamethasone in front-foot surgery under ankle block: A randomized double-blind study. Regional Anesthesia and Pain Medicine. 2018; 43 :732-737 - 10.
Hofmann-Kiefer KF, Gaube F, Groene P, Böcker W, Polzer H, Baumbach SF. “High ankle block” for surgery at the ankle joint. Foot and Ankle Surgery. Dec 2022; 28 (8):1254-1258. DOI: 10.1016/j.fas.2022.05.006. Epub 2022 May 26. PMID: 35654730 - 11.
Delbos A, Philippe M, Clément C, Olivier R, Coppens S. Ultrasound-guided ankle block. History revisited. Best Practice & Research. Clinical Anaesthesiology. 2019; 33 (1):79-93. DOI: 10.1016/j.bpa.2019.05.002. PMID: 31272656. Epub 2019 May 7 - 12.
Fredrickson MJ. Ultrasound-guided ankle block. Anaesthesia and Intensive Care. 2009; 37 :143-144 - 13.
Bindu S, Mazumder S, Bandyopadhyay U. Non-steroidal anti-inflammatory drugs (NSAIDs) and organ damage: A current perspective. Biochemical Pharmacology. 2020; 180 :114147. DOI: 10.1016/j.bcp.2020.114147 - 14.
Burd TA, Hughes MS, Anglen JO. Heterotopic ossification prophylaxis with indomethacin increases the risk of long-bone nonunion. The Journal of Bone and Joint Surgery. British Volume. 2003; 85 :700-705 - 15.
Chrastil J, Sampson C, Jones KB, Higgins TF. Postoperative opioid administration inhibits bone healing in an animal model. Clinical Orthopaedics and Related Research. 2013; 471 :4076-4081. DOI: 10.1007/s11999-013-3232-z - 16.
Scuderi GR. The challenges of perioperative pain management in total joint arthroplasty. The American Journal of Orthopedics. 2015; 44 :S2-S4 - 17.
Fraser TW, Doty JF. Peripheral nerve blocks in foot and ankle surgery. The Orthopedic Clinics of North America. 2017; 48 :507-515. DOI: 10.1016/j.ocl.2017.06.008 - 18.
Vadivelu N, Kai AM, Maslin B, Kodumudi V, Antony S, Blume P. Role of regional anesthesia in foot and ankle surgery. Foot & Ankle Specialist. 2015; 8 :212-219 - 19.
Albaqami MS, Alqarni AA. Efficacy of regional anesthesia using ankle block in ankle and foot surgeries: A systematic review. European Review for Medical and Pharmacological Sciences. Jan 2022; 26 (2):471-484. DOI: 10.26355/eurrev_202201_27872. PMID: 35113423 - 20.
Tryba M. Ankle block: A safe and simple technique for foot surgery. Current Opinion in Anaesthesiology. 1997; 10 :361-365 - 21.
Lee TH, Wapner KL, Hecht PJ, Hunt PJ. Regional anesthesia in foot and ankle surgery. Orthopedics. 1996; 19 :577-580 - 22.
Rudkin GE, Micallef TA. Impediments to the use of ankle block in Australia. Anaesthesia and Intensive Care. 2004; 32 :368-371 - 23.
López AM, Sala-Blanch X, Magaldi M, Poggio D, Asuncion J, Franco CD. Ultrasound-guided ankle block for forefootsurgery: The contribution of the saphenous nerve. Regional Anesthesia & Pain Medicine. 2012; 37 :554-557 - 24.
Peng P. Ankle nerve block. In: Jankovic D, Peng P, editors. Regional Nerve Blocks in Anesthesia and Pain Therapy. Cham: Springer; 2022. DOI: 10.1007/978-3-030-88727-8_67 - 25.
Hancock KJ, Rice OM, Anthony CA, Glass N, Hogue M, Karam M, et al. Efficacy of multimodal analgesic injections in operatively treated ankle fractures: A randomized controlled trial. The Journal of Bone and Joint Surgery. American Volume. 2019; 101 :2194-2202. DOI: 10.2106/jbjs.19.00293 - 26.
Davidovitch R, Goch A, Driesman A, Konda S, Pean C, Egol K. The use of liposomal bupivacaine administered with standard bupivacaine in ankle fractures requiring open reduction internal fixation: A single-blinded randomized controlled trial. Journal of Orthopaedic Trauma. 2017; 31 :434-439. DOI: 10.1097/bot.0000000000000862 - 27.
Kaller P, Hohenberger G, Holweg P, Seibert FJ, Ornig M. Ankle block. Operative Orthopädie und Traumatologie. 2020; 32 :29-34. DOI: 10.1007/s00064-019-00634-x - 28.
Yared M, Brown DL. Ankle block. In: Brown’s Atlas of Regional Anesthesia. 6th ed. Elsevier; 2021. pp. 157.e1-164.e1. ISBN: 978-0-323-65435-7 - 29.
Chin KJ, Wong NWY, Macfarlane AJR, Chan VWS. Ultrasound-guided versus anatomic landmark-guided ankle blocks: A 6-year retrospective review. Regional Anesthesia and Pain Medicine. 2011; 36 :611-618 - 30.
Girón-Arango L, Vásquez-Sadder MI, González-Obregón MP, Gamero-Fajardo CE. Bloqueo de tobillo guiado por ultrasonido: Una técnica anestésica atractiva para cirugía de pie. Colombian Journal of Anesthesiology. 2015; 43 (4):283-289. Retrieved January 24, 2024, fromhttp://www.scielo.org.co/scielo.php?script=sci_arttext&pid=S0120-33472015000400005&lng=en&tlng=es - 31.
Peer S, Gruber H. Atlas of Peripheral Nerve Ultrasound. Berlin: Springer; 2013 - 32.
Delbos. Peripheral Nerve Blocks on DVD Version 3- Lower Limbs. Philadelphia: Lippincott; 2012 - 33.
Lawrence SJ. The deep peroneal nerve in the foot and ankle: An anatomic study. Foot & Ankle International. 1995; 16 :724-728 - 34.
Mazzella NL, McMillan AM. Contribution of the sural nerve to postural stability and cutaneous sensation of the lower limb. Foot & Ankle International. 2015; 36 :450-456 - 35.
Chen J, Lesser J, Hadzic A, Resta-Flarer F. The importance of the proximal saphenous nerve block for foot and ankle surgery. Regional Anesthesia and Pain Medicine. 2013; 38 :372 - 36.
Fredrickson MJ, White R, Danesh-Clough TK. Low-volume ultrasound-guided nerve block provides inferior postoperative analgesia compared to a higher-volume landmark technique. Regional Anesthesia and Pain Medicine. 2011; 36 :393-398 - 37.
Lin E, Gaur A, Jones M, Ahmed A. Sonoanatomy for Anesthetists. United Kingdom: Cambridge University Press; 2012 - 38.
Redborg KE, Antonakakis JG, Beach ML, Chinn CD, Sites BD. Ultrasound improves the success rate of a tibial nerve block at the ankle. Regional Anesthesia and Pain Medicine. 2009; 34 :256-260 - 39.
De Mey JC, Deruyck LJ, Cammu G, de Baerdemaeker LE, Mortier EP. A paravenous approach for the saphenous nerve block. Regional Anesthesia and Pain Medicine. 2001; 26 :504-550 - 40.
Antonakakis J, Scalzo DC, Jorgenson AS, Figg KK, Ting P, Zuo Z, et al. Ultrasound does not improve the success rate of a deep peroneal nerve block at the ankle. Regional Anesthesia and Pain Medicine. 2010; 35 :217-221 - 41.
Canella C, Demondion X, Guillin R, Boutry N, Peltier J, Cotten A. Anatomic study of the superficial peroneal nerve using sonography. AJR. American Journal of Roentgenology. 2009; 193 :174-179 - 42.
Chin KJ. Ultrasound visualization of the superficial peroneal nerve in the mid-calf. Anesthesiology. 2013; 118 :956-965 - 43.
Redborg KE, Sites BD, Chinn CD, Gallagher JD, Ball PA, Antonakakis JG, et al. Ultrasound improves the success rate of a sural nerve block at the ankle. Regional Anesthesia and Pain Medicine. 2009; 34 :24-28 - 44.
Falyar CR. Ultrasound-guided ankle blocks: A review of current practices. AANA Journal. 2015; 83 :357-364 - 45.
Migues A, Slullitel G, Vescovo A, Droblas F, Carrasco M, Perrin TH. Peripheral foot blockade versus popliteal fossa nerve block: A prospective randomized trial in 51 patients. The Journal of Foot and Ankle Surgery. 2005; 44 :354-357 - 46.
Gbejuade H, Squire J, Dixit A, Kaushik V, Mangwani J. Ultrasound-guided regional anesthesia in foot and ankle surgery. Journal of Clinical Orthopaedics and Trauma. 2020; 11 :417-421