
Abstract
Nowadays, we are seeing radically interesting and promising changes in the treatment of patients with type-2 diabetes mellitus (T2 D), which favorably modify the prognosis related to fundamentally neuro-nephro and cardiorenal outcomes. Since no more than two decades ago, the pharmacological armamentarium for the treatment of people with T2D has basically consisted of the use of biguanides, sulfonylureas, insulin sensitizers, and insulins. A great amount of information has been accumulated through the results of new molecules such as sodium/glucose co-transporter type-2 inhibitors (SGLT2i), based on robust data arising from the experience of numerous studies, both clinical and experimental, as well as the glucagon-like peptide 1 receptor agonists (GLP-1ra), that has clearly shown multisystem benefits that improve the function of target organs and delay the onset of complications that ultimately impact the quality of life and the neuro-nephro-cardiovascular outcomes. In this review chapter, we not only highlight the different strategies for glucose control through SGLT2i, GLP-1ra or insulin, including even some fixed combinations, but also some information on different studies with GIP/GLP1 biagonist tirzepatide and on GIP/GLP1/Glucagon triagonist retatrutide primarily focused on weight loss, even though today, they are neither FDA approved nor a part of routine treatment.
Keywords
- type 2 diabetes mellitus
- Glycocentric
- SGLT2i
- glucagon like peptide-1 analog
- tirzepatide
- retatrutide
- Nephro-protection
- cardio-protection
- neuroprotection
1. Introduction
Diabetes is a chronic, metabolic syndrome affecting about 537 million people worldwide, without considering those with undiagnosed diabetes. Type 2 diabetes (T2D) is the most common, and it represents around 80–90% of the cases [1].
Type 2 diabetes is characterized by chronic high blood glucose levels due to a deficiency in insulin production, a peripheral body’s resistance to it, or both. The phenotypic expression of genetic defects in diabetogenic genes conditions alterations in insulin secretion, while peripheral insulin resistance is a consequence of the interaction of environmental risk factors (type of diet, sedentary lifestyle, etc.) [2].
The pathogenesis of diabetes has changed over time, from a unique approach collectively, from the insulin resistance in muscle and liver and β-cell failure referred to as the triumvirate (triumvirate), to the interaction of several phenomena as explained in the ominous octet. This ominous octet refers to the interaction of different pathways and organs related to the pathophysiology of T2D, including pancreatic β-cell failure, increased glucagon secretion, increased gluconeogenesis, increased lipolysis, insulin resistance, decreased incretin effect, decreased peripheral glucose uptake, increased renal glucose reabsorption, and alterations of neurotransmitters. All these leads are called the ominous octet (Figure 1) [3, 4, 5].
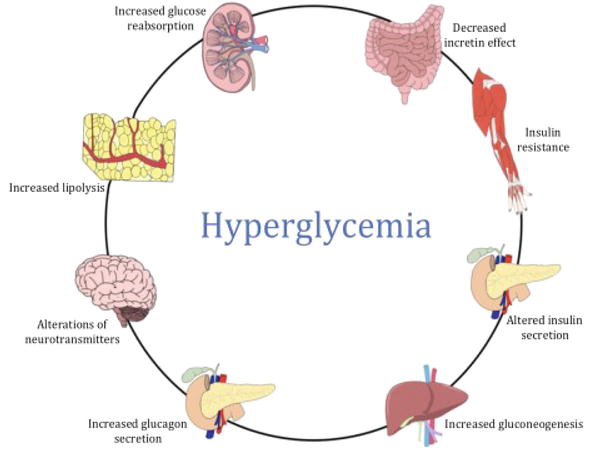
Figure 1.
The ominous octet summarizes the different mechanisms that lead to hyperglycemia.
2. Macrovascular complications
Type 2 diabetes is related to accelerating atherosclerosis and is a leading cause of macrovascular complications, which include coronary heart disease, heart failure, cerebrovascular disease, and peripheral artery disease [6].
2.1 Coronary heart disease
As the prevalence of obesity and diabetes is increasing, the incidence of coronary heart disease (CHD) is also increasing, and it is reported as the leading cause of morbidity and mortality in people with diabetes. T2D is related to an increased risk of angina pectoris and asymptomatic ischemic episodes [7].
2.2 Heart failure
The prevalence of heart failure in people with diabetes is high, and it is a factor with a high impact on cardiovascular mortality and morbidity. Observations over the years have shown that myocardial dysfunction can occur in the absence of other cardiovascular diseases such as CHD, valvular heart disease, or hypertrophy [8].
An important characteristic observed in diabetic myocardium by imaging studies is the left ventricular concentric remodeling, and it is possibly attributed to impaired myocardial energetics and reduced systolic strain. Myocardial hypertrophy is attributed to hyperinsulinemia, myocardial triglyceride deposition, and an increased extracellular volume, which promotes collagen deposition and fibrosis. Mortality and hospitalization due to heart failure are higher in people with diabetes compared with non-diabetics [9].
2.3 Cerebrovascular disease
People with diabetes are highly susceptible to suffering a cerebrovascular event, and they are 12 times more likely to be hospitalized due to those events. Diabetes is a high-risk factor syndrome for ischemic stroke due to a group of events that include excessive oxidation, formation of advanced glycation end products, increased platelet aggregation, endothelial dysfunction, insulin resistance, impaired fibrinolysis, and hypercoagulability; these factors increase the risk for large artery atherosclerotic occlusive disease, facilitating an ischemic event [10].
2.4 Peripheral vascular disease
Peripheral vascular disease (PVD) is a common complication in people with diabetes, and it is usually a predictive factor for generalized artery dysfunction, including the prediction of cardiovascular events. Unfortunately, PVD is a disorder that occurs asymptomatic in many patients due to the presence of peripheral neuropathy; therefore, PVD is noticed until a complication like gangrene or ischemic ulcer appears, which inevitably leads to amputation [11].
3. Microvascular complications
The duration of the hyperglycemic state and genetic predisposition interacts and eventually affects the microvasculature, leading to complications in organs such as kidneys and eyes, as well as diabetic neuropathy [12].
3.1 Retinopathy
The most common cause of blindness worldwide is diabetic retinopathy (DR), and it appears in approximately 25.16% of the diabetic population. DR early signs are usually asymptomatic, so it is important to keep a regular eye examination in people with diabetes. DR is classified into two categories, non-proliferative DR and proliferative DR. It is important to identify early signs of DR to reduce the risk of visual loss [11].
3.2 Nephropathy
Diabetic nephropathy is defined as impaired kidney function in diabetic patients. This disease affects approximately 25% of people with diabetes. The diabetic nephropathy diagnosis is important because not all kidney alterations should be attributed to diabetes [11].
The American Diabetes Association (ADA) established that the diagnosis should be based upon the findings of decreased glomerular filtration rate (<60 ml/min/1.73 m2) and/or an increased urinary albumin excretion (≥30 mg/g creatinine) for at least 3 months [12].
4. Current treatment of type 2 diabetes mellitus
Despite the successful generation of a major difference in glycemic control between the intensive and conventional treatment arms, the well-known United Kingdom Prospective Diabetes Study (UKPDS) did not demonstrate the benefits on macrovascular disease, including the Action to Control Cardiovascular Risk in Diabetes (ACCORD), the Action in Diabetes and Vascular Disease (ADVANCE), and the Veterans Affairs Diabetes Trial (VADT) [13, 14, 15]. Even the ACCORD caused alarm when the trial was terminated prematurely at 3.5 years in response to an unexpected—and to date unexplained—22% increased mortality in the intensive glycemic control group [13, 16, 17]. The ACCORD investigators concluded that even though intensive glycemic control reduced non-fatal myocardial infarctions, this approach could not be recommended for high-risk patients with advanced type 2 diabetes [16].
On the other hand, in epidemiological studies, it is well known that cardiovascular risk rises with worsening glycemic control, defined by fasting glucose or HbA 1c [18]. For this reason, we must remember the essential role of insulin in glycemic control, which remains the therapy of choice, particularly when the patient is metabolically uncontrolled as reported in a meta-analysis and meta-regression in five RCTs involving 590 participants with type 2 diabetes, that insulin pump therapy continuous subcutaneous insulin infusion (CSII; insulin pump therapy) achieves better glycemic control than multiple daily insulin injections (MDI) in participants with poor diabetes control at baseline; even more, CSII therapy safely and significantly improved metabolic control with less insulin usage and with no sustainable reduction of BM, blood pressure, and lipid profile, in insulin-resistant T2D people, with excellent treatment adherence and satisfaction [19, 20]. Besides, it is worth noting the importance played by insulin analogs such as insulin glargine or degludec, as well as fixed combinations with glucagon-like peptide-1 receptor agonists such as liraglutide, where in a study carried out to demonstrate the efficacy and safety of a fixed-ratio combination of insulin degludec and liraglutide (IDegLira) compared with its components given alone, IDeLira reduced 1.9% HbA1c, and no clinically relevant differences between treatments with respect to standard safety assessments were noted, and the safety profile of IDegLira reflected those of its component parts [21]. However, recent landmark cardiovascular outcome trials (CVOTs) in patients with T2D have revealed major benefits of certain glucose-lowering medications in terms of reduction of cardiovascular events [18]. Trials of agents from two classes of novel glucose-lowering drugs, that is, sodium-glucose cotransporter-2 inhibitors (SGLT2i) and glucagon-like peptide receptor agonists (GLP-1ra), have shown statistically significant and clinically meaningful reductions in three- or four-point major adverse cardiovascular events (MACE), both in patients with established cardiovascular diseases and in those at high risk for such disease [13, 14, 15, 16]. These results stand in marked contrast to earlier trials trying to primarily lower HbA1c, by using combinations of antihyperglycemic agents that failed to show any benefit of lowering HbA1c in reducing macrovascular events.
In this regard, the ADA/EASD consensus report “Management of Hyperglycemia in Type 2 Diabetes, 2022” [22, 23, 24] recommends a holistic, multifactorial, person-centered approach accounting for the lifelong nature of type 2 diabetes. Person-specific factors that affect the choice of treatment include individualized glycemic and weight goals, impact on weight, hypoglycemia and cardiorenal protection, underlying physiologic factors, side effect profiles of medications, complexity of regimen, regimen choice to optimize medication use and reduce treatment discontinuation, and access, cost, and availability of medication. Lifestyle modifications and health behaviors that improve health should be emphasized along with any pharmacologic therapy. This chapter will broadly address the benefits of preventing or delaying the progression of complications, particularly at the cardiovascular and renal level, and in less detail the effects on the central nervous system observed in experimental studies with these pharmacological classes, such as SGLT2i, as well as GLP-1ra, which have shown a favorable impact, especially on cardiovascular and renal outcomes.
5. The role of glucose/sodium cotransporter type 2 (ISGLT2) inhibitors
Sodium-glucose cotransporter-2 inhibitors (SGLT2i), also known as gliflozins or flozins, are relatively new glucose-lowering drugs that include empagliflozin, dapagliflozin, canagliflozin, and ertugliflozin; they are used as a T2D treatment. By inhibiting the SGLT2 expressed in the proximal convoluted tubule of the nephron (responsible for 90% of glucose reabsorption), these drugs favor glycosuria and hence lower glycemia levels. Although they are believed to cause smaller HbA1C reductions (between 0.5 and 0.7%) than other antidiabetics, the multi-organic benefits addressed in this section, which comprehend neuro, cardio, and nephroprotective effects, are simply outstanding [25] (Figure 2).
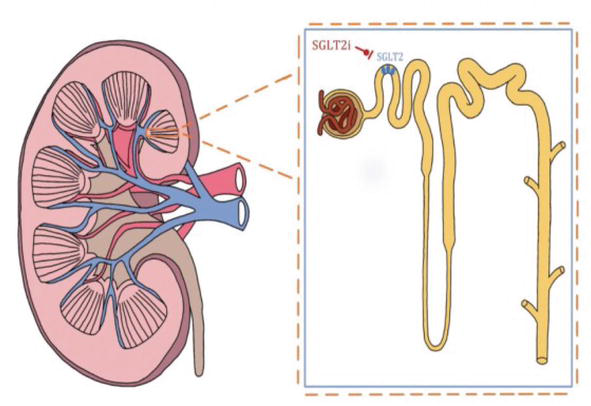
Figure 2.
Shows the site of action of SGLT2i in the nephron.
5.1 Empagliflozin and neuroprotective effects
Since iSGLT2 are lipid-soluble drugs, they can cross the brain–blood barrier and exert interesting neuroprotective effects. Among the ones to be highlighted, empagliflozin states the fact that, when the appropriate brain concentrations are reached (around 0.5 μM), this medicament works as an acetylcholinesterase (AChE) inhibitor. When AChE activity is decreased, acetylcholine M1 receptors face an important increment and thus favor a functional cognitive improvement [25].
T2D patients tend to have low brain-derived neurotrophic factor (BDNF) levels. This becomes relevant when realizing that BDNF plays a crucial role in neuronal growth and plasticity, neurotransmission, memorizing, and learning processes. Hence, cognitive impairment is propitiated, not to mention that it’s been associated with inflammation and consequent atherosclerosis risk. When being treated with Empagliflozin, at least in mice, BNDF levels show an important increase [25].
5.2 Empagliflozin and cardioprotective effects
Empagliflozin has been associated, among randomized clinical trials, to lower hospitalization, myocardial infarctions, nonfatal strokes, and death from cardiovascular disease rates. Although these may sound like greater effects, there are other significant ones such as decreases in both systolic and diastolic blood pressures (without compensatory higher heart rates) and reduction in weight, waist circumference, and uric acid level [26].
On the other hand, heart failure is recognized as an important diabetic comorbidity; hence, considering Empagliflozin’s diuretic effect, it can be said that its main effect focuses on reducing plasma volume, leading to increased hematocrit and an expected blood pressure drop (3–4 mmHg in 12 weeks), alleviating the heart’s workload. Another significant myocardial effect consists of reducing diastolic stiffness and improving diastolic function [27].
5.3 Empagliflozin and nephroprotective effects
T2D patients are susceptible to developing microvascular complications such as kidney disease, which afflicts around 35% of them and magnifies mortality rates. This reason is sufficient to look for innovative therapies, such as SGLT2i’s use. In several clinical trials, Empagliflozin has been demonstrated to have renal protective effects, even though the underlying mechanism is not well evidenced. Nevertheless, it is believed to be a summation of the association with blood pressure and body mass reduction, diuresis, and activation of tubuloglomerular feedback [28, 29, 30].
5.4 Dapagliflozin and neuroprotective effects
Dapagliflozin exerts no significant improvement in cognitive domains, nor in impaired brain activation, compared to other drugs. However, rat models suggest quite impressive effects. Likewise, it’s been associated with the improvement of brain mitochondrial membrane depolarization, function, swelling, and decreased ROS production [31]. Among other numerous benefits, the medicament demonstrated both antioxidant and antiapoptotic properties by alleviating memory and cognition impairment in Streptozotocin (STZ)-induced diabetic rats, probably through its effect on Wnt/β-Catenin and cAMP-response element binding protein (CREB) pathway [32].
5.5 Dapagliflozin and cardioprotective effects
T2D people harbor considerable risk factors, which make them more susceptible to developing atherosclerotic cardiovascular disease and its derivatives. Supporting this idea states the relevance of clinical studies, which show findings such as that prejudicial cardiovascular outcomes in T2D patients treated with Dapagliflozin, according to DECLARE-TIMI 58 clinical trial results, were proven to diminish. This is a fact sustained by an evident lowering of hospitalizations for heart failure and cardiovascular death [33].
5.6 Dapagliflozin and nephroprotective effects
Worrisome renal outcomes in T2D patients, if they have not already progressed into a kidney disease stage, are major events. Therefore, the fact that a sodium-glucose cotransporter-2 inhibitor like Dapagliflozin has been studied and tested in clinical studies represents a scenario leading to new windows of opportunity. Trials such as DAPA-CKD and DECLARE-TIMI 58 found that when administering this medication (compared to placebo), there was a lowering of the declines in the eGFR, meaning a reduction in the progression of kidney disease, a situation that simultaneously translates into less renal-caused deaths [34].
5.7 Others gliflozins
Canagliflozin and Ertugliflozin are also relevant medicaments, belonging to the SGLT2i class. As could be expected, they both have demonstrated their efficacy in lowering hyperglycemia and exerting favorable cardiorenal effects in their principal clinical studies: CREDENCE and VERTIS CV, respectively [35, 36].
6. Glucagon-like peptide 1 receptor agonists
Glucagon-like peptide 1 (GLP-1) is an incretin hormone released from intestinal L-cells of the distal ileum. It is postprandially secreted and binds to a seven-transmembrane G protein-coupled receptor to activate signaling cascades, leading to beneficial downstream effects that include increased insulin secretion in a glucose-dependent manner, somatostatin secretion, lipolysis, decreased glucagon secretion, decreased gastric emptying, and satiety, which leads to a promotion of weight loss (Figure 3) [37, 38, 39].
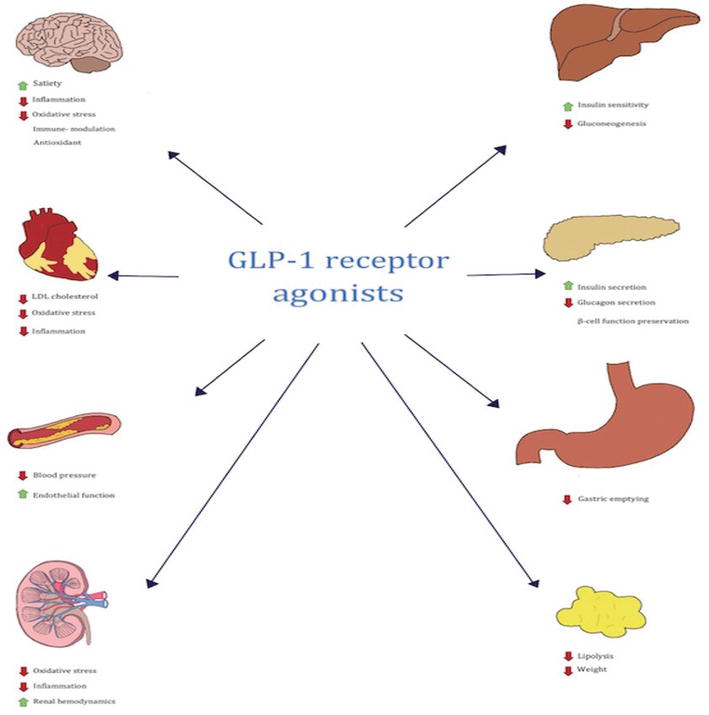
Figure 3.
Shows the different sites of action of GLP-1 receptor agonists.
The beta-cell mass (responsible for insulin secretion) is reduced in the later stages of T2D, resulting in the requirement of exogenous insulin therapy. Therefore, beta-cell mass preservation and strategies to stimulate beta-cell replication is an important aim in a recent investigation. In this respect, GLP-1 has also shown beta-cell preservation effects (beta-cell proliferation, neogenesis, and prevention of apoptosis) [35, 38]. There are six GLP-1 receptor agonists approved as T2D treatment. Those are dulaglutide, semaglutide (oral and injected), exenatide, albiglutide, liraglutide, and lixisenatide [39].
6.1 Dulaglutide and neuroprotective effects
GLP-1 receptor agonists have demonstrated neuroprotective effects in a range of neurodegenerative conditions. Since GLP-1 receptors are expressed throughout the brain, this type of drug is considered to have neurotrophic and anti-inflammation effects for central nervous system (CNS) diseases. A recent study demonstrated that dulaglutide possessed protective effects on the pathogenesis of experimental autoimmune encephalomyelitis (EAE), which is an established animal model to study human multiple sclerosis [40, 41].
In EAE pathogenesis, the CD4 positive T cells especially Type 1 helper T (Th1) and Type 17 helper T (Th17), which are also interferon (IFN)-y secreting and interleukin (IL)-17 A producing, are inflammatory T cells that mediate the demyelination of neurons in the CNS. In this sense, dulaglutide holds protective effects via immune-modulation of CD4-positive T helper cell lineage in the CNS parenchyma by suppressing the percentage of encephalitogenic Th1/Th17 cells [40].
On the other hand, Parkinson’s is one of the most common neurodegenerative diseases that is often linked with diabetes. They both are chronic disorders with pathogenic mechanisms being mitochondrial failure, oxidative stress, and protein aggregation; therefore, patients with T2D are more likely to experience severe Parkinson’s disease (PD) symptoms and accelerated neurodegeneration. That being the case, there has been research done to examine the neuroprotective effects of these antidiabetic medications [41, 42, 43].
6.2 Dulaglutide and cardioprotective effects
The REWIND trial carried out in 24 countries to assess the cardioprotective effects of dulaglutide in people with cardiovascular risk factors, who were under antihyperglycemic regimens, suggested that dulaglutide reduced cardiovascular events. It also reduced weight, LDL cholesterol, and blood pressure, suggested as the mechanisms by which dulaglutide exerts cardioprotective effects. Moreover, the study also showed dulaglutide’s long-term safety effects and durability [44].
6.3 Dulaglutide and nephroprotective effects
In the REWIND trial, renal outcomes were collected as part of the secondary microvascular outcome. It showed that dulaglutide reduced all three components of composite renal outcome (the development of new macroalbuminuria, a sustained ≥30% decline in eGFR, and chronic renal replacement therapy), having a robust effect on the development of macroalbuminuria.
The study suggested that dulaglutide reduced the progression of kidney disease and preserved renal function by reducing HbA1c and systolic blood pressure. However, there is evidence that proposes GLP-1 receptor agonists as agents that directly affect the kidney by reducing inflammation and oxidative stress and improving endothelial function. Therefore, analyses concluded that dulaglutide is an antidiabetic treatment that is likely to confer additional renal benefits [44].
6.4 Semaglutide and neuroprotective effects
Although GLP-1 receptors are expressed in some brain regions, there are some reports suggesting that semaglutide does not cross the blood–brain barrier (BBB). However, it may have access to GLP-1 receptors through leaks in BBB or have an entry into additional regions of the brain. Besides, semaglutide improves insulin resistance and signaling pathways and reduces body mass, which are important factors in the progression of metabolic and neurodegenerative diseases. There have been studies that have demonstrated the neuroprotective efficacy of semaglutide in the rat model and in human neuroblastoma by decreasing inflammation and apoptosis. It has been demonstrated that semaglutide can be safely administered to adults including geriatric patients with renal, hepatic, and cardiovascular disorders [45].
6.5 Semaglutide and cardioprotective effects
Semaglutide is a long-acting GLP-1 analog for T2D with an extended half-life of approximately 1 week that has been shown to inhibit exercise-induced myocardial oxidative stress and inflammation, which are mechanisms that also occur in hyperglycemic states. Semaglutide exerts cardioprotective effects by activating the AMPK pathway and reducing ROS production and inflammation-related proteins. Moreover, this medicament ameliorated myocardial morphological changes and lipid accumulation, which leads to an increase of myocardial oxidative stress response, common in diabetic cardiomyopathy, and decreased the expression of NF-kB, TNF-α, and IL-1β [45, 46].
Both studies (SUSTAIN-6 and PIONEER-6) demonstrated that semaglutide therapy reduces 24% of cardiovascular adverse effects. Moreover, semaglutide-treated patients had a lower risk of nephropathy but a higher risk of diabetic retinopathy complications (vitreous hemorrhage, blindness, or the need for treatment with an intravitreal agent or photocoagulation) in comparison with those receiving placebo. This drug also showed sustained weight loss and a reduction in systolic blood pressure vs. placebo group over 2 years. Given this, semaglutide was the first long-acting GLP-1 receptor agonist to be approved by the United Food and Drug Administration for obesity management [46, 47].
6.6 Semaglutide and nephroprotective effects
Recent evidence supports that GLP-1 receptor agonists improve cardiovascular and renal outcomes in T2D by promoting weight loss, blood pressure, and glycemic control. In this sense, semaglutide has been demonstrated to improve cardiorenal outcomes in patients with T2D. One recent study shows semaglutide’s effect on renal outcomes in the db/db UNx-Renin AAV mouse model of hypertension accelerated DKD, which reported a reduced glomerulosclerosis severity and improvements in hyperglycemia, systolic and diastolic blood pressure, and albuminuria. The antihypertensive action of GLP-1 receptor agonists may be secondary to their diuretic and natriuretic effects, and there is speculation that the nephroprotective activity of semaglutide could be linked to the improvement in renal hemodynamics. GLP-1 receptors in the kidney are reported to be in the vascular smooth muscle cells; therefore, their activation mediates renal vasorelaxant and blood flow, which translates to the preservation of glomerular function [37, 48].
6.7 Other GLP-1 analogs, dual and triple agonist
Several trials have reported that apart from the improvement in glucose control and the decrease in body mass and blood pressure, liraglutide and albiglutide reported a reduced hazard of the primary cardiovascular outcome (nonfatal myocardial infarction, nonfatal stroke, or death from cardiovascular causes). In addition, liraglutide and lixisenatide reduced the predefined composite renal outcome mainly by a lower incidence of macroalbuminuria [39, 49].
Regarding the neuroprotective effects of the GLP-1 agonists, lixisenatide was found to be a protective treatment of behavioral and neurological functions. It also has a suppressing effect on cerebral oxidative stress and inflammation in diabetic rats. On this subject, liraglutide was reported to suppress neuroinflammation. Lastly, exenatide was also found to have neuroprotective effects in preclinical models of Parkinson’s disease [50, 51]. Finally, a novel dual glucose-dependent insulinotropic polypeptide and GLP-1 receptor agonist tirzepatide (Figure 4) and a GIP/GLP1/Glucagon triagonist retatrutide are being investigated, both in clinical trials and in experimental studies, respectively, which have shown a benefit in metabolic control through the reduction of HbA1c, and in body mass mainly, with reductions around 20–30% compared with the results observed through bariatric surgery, although currently, they are neither FDA approved nor of routine treatment [52, 53].
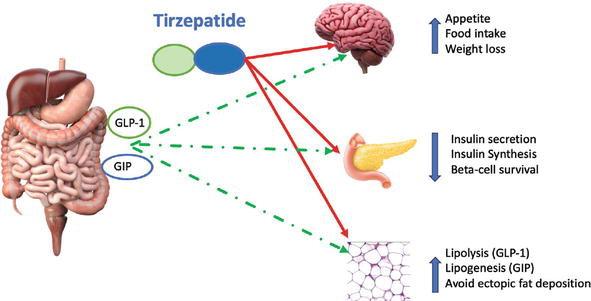
Figure 4.
Shows the different mechanisms of action of Tirzepatide.
7. Conclusion
With all this information and in view of this promising panorama with these new molecules whose outcomes favor a better prognosis regarding, control glucose, weight reduction, microvascular, and macrovascular complications, it is necessary to consider a personalized holistic therapy for each patient to improve their quality of life and reduce their morbidity and mortality.
References
- 1.
International Diabetes Federation. IDF Diabetes Atlas 10th edition 202. diabetesatlas.org . 2021. Available from:https://diabetesatlas.org/ - 2.
Conget I. Diagnóstico, clasificación y patogenia de la diabetes mellitus. Revista Española de Cardiología. 2002; 55 (5):528-535 - 3.
DeFronzo RA. From the triumvirate to the ominous octet: A new paradigm for the treatment of type 2 diabetes mellitus. Diabetes. 2009; 58 (4):773-795. DOI: 10.2337/db09-9028 - 4.
Yap-Campos K, Sánchez-Gálvez X, Rivero-López C. El papel de los inhibidores de la DPP4: un enfoque actual en el manejo de la diabetes mellitus tipo 2. Aten Fam. 2017; 24 (3):136-139 - 5.
Huang D, Refaat M, Mohammedi K, Jayyousi A, Al Suwaidi J, Abi KC. Macrovascular complications in patients with diabetes and prediabetes. BioMed Research International. 2017; 2017 :1-9 - 6.
Viigimaa M, Sachinidis A, Toumpourleka M, Koutsampasopoulos K, Alliksoo S, Titma T. Macrovascular complications of type 2 diabetes mellitus. Current Vascular Pharmacology. 2019; 18 (2). DOI: 10.2174/1570161117666190405165151 - 7.
Wilson PWF. Diabetes mellitus and coronary heart disease. Endocrinology and Metabolism Clinics of North America. 2001; 30 (4):857-881. DOI: 10.1016/S0889-8529(05)70219-X - 8.
Lehrke M, Marx N. Diabetes mellitus and heart failure. The American Journal of Medicine. 2017; 130 (6S):S40-S50. DOI: 10.1016/j.amjmed.2017.04.010 - 9.
Lukovits TG, Mazzone T, Gorelick PB. Diabetes mellitus and cerebrovascular disease. Neuroepidemiology. 1999; 18 (1):1-14. DOI: 10.1159/000026190 - 10.
Huysman E, Mathieu C. Diabetes and peripheral vascular disease. Acta chirurgica Belgica. 2009; 109 (5):587-594. DOI: 10.1080/00015458.2009.11680493 - 11.
Faselis C, Katsimardou A, Imprialos K, Deligkaris P, Kallistratos M, Dimitriadis K. Microvascular complications of type 2 diabetes mellitus. Current Vascular Pharmacology. 2020; 18 (2):117-124. DOI: 10.2174/1570161117666190502103733 - 12.
Summary of Revisions. Standards of medical Care in diabetes—2020. Diabetes Care. 2019; 43 (Supplement 1):S4-S6. DOI: 10.2337/dc20-srev - 13.
Gerstein HC, Miller ME, Byington RP, et al. Effects of intensive glucose lowering in type 2 diabetes. The New England Journal of Medicine. 2008; 358 (24):2545-2559 - 14.
Patel A, MacMahon S, Chalmers J, et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. The New England Journal of Medicine. 2008; 358 (24):2560-2572 - 15.
Duckworth W, Abraira C, Moritz T, et al. Glucose control and vascular complications in veterans with type 2 diabetes. The New England Journal of Medicine. 2009; 360 (2):129-139 - 16.
Dluhy RG, McMahon GT. Intensive glycemic control in the ACCORD and ADVANCE trials. The New England Journal of Medicine. 2008; 358 (24):2630-2633 - 17.
Group AS, Gerstein HC, Miller ME, et al. Long-term effects of intensive glucose lowering on cardiovascular outcomes. The New England Journal of Medicine. 2011; 364 (9):818-828 - 18.
Dal Canto E, Ceriello A, Ryden L, et al. Diabetes as a cardiovascular risk factor: An overview of global trends of macro and microvascular complications. European Journal of Preventive Cardiology. 2019; 26 (2S):25-32 - 19.
Pickup JC, Reznik Y, Sutton AJ. Glycemic control during continuous subcutaneous insulin infusion versus multiple daily insulin injections in type 2 diabetes: Individual patient data meta-analysis and meta-regression of randomized controlled trials. Diabetes Care. 2017; 40 :715-722 - 20.
Chlup R, Runzis S, Castaneda J, Lee S, Nguyen X, Cohen O. Complex assessment of metabolic effectiveness of insulin pump therapy in patients with type 2 diabetes beyond HbA1c reduction. Diabetes Technology and Therapeutics. 2018; 20 (2):153-159 - 21.
Gough SC, Bode B, Woo V, Rodbard HW, Linjawi S, Poulsen P, et al. Efficacy and safety of a fixed-ratio combination of insulin degludec and liraglutide (IDegLira) compared with its components given alone: Results of a phase 3, open-label, randomised, 26-week, treat-to-target trial in insulin-naive patients with type 2 diabetes. Lancet Diabetes Endocrinol. 2014; 2 (11):885-893. DOI: 10.1016/S2213-8587(14)70174-3 - 22.
Davies MJ, D’Alessio DA, Fradkin J, et al. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of diabetes (EASD). Diabetes Care. 2018; 2018 (41):2669-2701 - 23.
Buse JB, Wexler DJ, Tsapas A, et al. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of diabetes (EASD). Diabetes Care. 2018; 2020 (43):487-493 - 24.
Davies MJ, Aroda VR, Collins BS, et al. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of diabetes (EASD). Diabetes Care. 2022; 2022 (45):2753-2786 - 25.
Pawlos A, Broncel M, Woźniak E, Gorzelak-Pabiś P. Neuroprotective effect of SGLT2 inhibitors. Molecules. 2021; 26 (23):7213. DOI: 10.3390/molecules26237213 - 26.
Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, et al. EMPA-REG OUTCOME Investigators. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. The New England Journal of Medicine. 2015; 373 (22):2117-2128. DOI: 10.1056/NEJMoa1504720 - 27.
Pabel S, Wagner S, Bollenberg H, et al. Empagliflozin directly improves diastolic function in human heart failure. Journal of Cardiac Failure. 2018; 20 (12):1690-1700. DOI: 10.1002/ejhf.1328 - 28.
Kowalska K, Walczak J, Femlak J, Młynarska E, Franczyk B, Rysz J. Empagliflozin—A new chance for patients with chronic heart failure. Pharmaceuticals (Basel). 2021; 15 (1):47. DOI: 10.3390/ph15010047 - 29.
Wanner C, Inzucchi SE, Lachin JM, Fitchett D, von Eynatten M, Mattheus M, et al. Empagliflozin and progression of kidney disease in type 2 diabetes. The New England Journal of Medicine. 2016; 375 (4):323-334. DOI: 10.1056/NEJMoa1515920 - 30.
Perrone-Filardi P, Avogaro A, Bonora E, Colivicchi F, Fioretto P, Maggioni AP, et al. Mechanisms linking empagliflozin to cardiovascular and renal protection. International Journal of Cardiology. 2017; 241 :450-456. DOI: 10.1016/j.ijcard.2017.03.089 - 31.
Erdogan MA, Yusuf D, Christy J, Solmaz V, Erdogan A, Taskiran E, et al. Highly selective SGLT2 inhibitor dapagliflozin reduces seizure activity in pentylenetetrazol-induced murine model of epilepsy. BMC Neurology. 2018; 18 (1):81. DOI: 10.1186/s12883-018-1086-4 - 32.
El-Safty H, Ismail A, Abdelsalam RM, El-Sahar AE, Saad MA. Dapagliflozin diminishes memory and cognition impairment in streptozotocin induced diabetes through its effect on Wnt/β-catenin and CREB pathway. Brain Research Bulletin. 2022; 181 :109-120. DOI: 10.1016/j.brainresbull.2022.01.017 - 33.
Wiviott SD, Raz I, Bonaca MP, Mosenzon O, Kato ET, Cahn A, et al. DECLARE–TIMI 58 Investigators. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. The New England Journal of Medicine. 2019; 380 (4):347-357. DOI: 10.1056/NEJMoa1812389 - 34.
Heerspink HJL, Stefánsson BV, Correa-Rotter R, Chertow GM, Greene T, Hou F-F, et al. For the DAPA-CKD trial committees and Investigators. Dapagliflozin in patients with chronic kidney disease. The New England Journal of Medicine. 2020; 383 :1436-1446. DOI: 10.1056/NEJMoa2024816 - 35.
Jardine MJ, Zhou Z, Mahaffey KW, Oshima M, Agarwal R, Bakris G, et al. Renal, cardiovascular, and safety outcomes of canagliflozin by baseline kidney function: A secondary analysis of the CREDENCE randomized trial. Journal of the American Society of Nephrology. 2020; 31 (5):1128-1139. DOI: 10.1681/ASN.2019111168 - 36.
Pratley RE, Cannon CP, Cherney DZI, Cosentino F, McGuire DK, Essex MN, et al. Cardiorenal outcomes, kidney function, and other safety outcomes with ertugliflozin in older adults with type 2 diabetes (VERTIS CV): Secondary analyses from a randomised, double-blind trial. Lancet Healthy Longev. 2023; 4 (4):e143-e154. DOI: 10.1016/S2666-7568(23)00032-6 - 37.
Lee Y-S, Jun H-S. Anti-diabetic actions of glucagon-like peptide-1 on pancreatic beta-cells. Metabolism. 2014; 63 (1):9-19. DOI: 10.1016/j.metabol.2013.09.010 - 38.
DeFronzo RA, Abdul-Ghani MA. Preservation of β-cell function: The key to diabetes prevention. The Journal of Clinical Endocrinology and Metabolism. 2011; 96 (8):2354k-23566k. DOI: 10.1210/jc.2011-0246 - 39.
Tommerdahl KL, Kendrick J, Bjornstad P. The role of glucagon-like peptide 1 (GLP-1) receptor agonists in the prevention and treatment of diabetic kidney disease: Insights from the AMPLITUDE-O trial. Clinical Journal of the American Society of Nephrology. 2022; 17 (6):905-907. DOI: 10.2215/CJN.00020122 - 40.
Kristensen SL, Rørth R, Jhund PS, Docherty KF, Sattar N, Preiss D, et al. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: A systematic review and meta-analysis of cardiovascular outcome trials. The Lancet. 2019; 7 (10):776-785 - 41.
Madsbad S. Review of head-to-head comparisons of glucagon-like peptide-1 receptor agonists. Diabetes, Obesity and Metabolism. 2016; 18 (4):317-332. DOI: 10.1111/dom.12596 - 42.
Chiou H-YC, Lin M-W, Hsiao P-J, Chen C-L, Chiao S, Lin T-Y, et al. Dulaglutide modulates the development of tissue-infiltrating TH1/Th17 cells and the pathogenicity of encephalitogenic Th1 cells in the central nervous system. International Journal of Molecular Sciences. 2019; 20 (7):1584. DOI: 10.3390/ijms20071584 - 43.
Maskery MP, Holscher C, Jones SP, Price CI, Strain WD, Watkins CL, et al. Glucagon-like peptide-1 receptor agonists as neuroprotective agents for ischemic stroke: A systematic scoping review. Journal of Cerebral Blood Flow & Metabolism. 2021; 41 (1):14-30. DOI: 10.1177/0271678X20952011 - 44.
Gerstein HC, Colhoun HM, Dagenais GR, Diaz R, Lakshmanan M, Pais P, et al. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): A double-blind, randomised placebo-controlled trial. The Lancet. 2019; 394 (10193):121-130. DOI: 10.1016/S0140-6736(19)31149-3 - 45.
Mahapatra M, Karuppasamy M, Sahoo BM. Therapeutic potential of semaglutide, a newer GLP-1 receptor agonist, in abating obesity, non-alcoholic steatohepatitis and neurodegenerative diseases: A narrative review. Pharmaceutical Research. 2022; 39 (6):1233-1248. DOI: 10.1007/s11095-022-03302-1 - 46.
Marso SP, Bain SC, Consoli A, Eliaschewitz FG, Jódar E, Leiter LA, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. The New England Journal of Medicine. 2016; 375 (19):1834-1844. DOI: 10.1056/NEJMoa1607141 - 47.
Bain SC, Mosenzon O, Arechavaleta R, et al. Cardiovascular safety of oral semaglutide in patients with type 2 diabetes: Rationale, design and patient baseline characteristics for the PIONEER 6 trial. Diabetes, Obesity & Metabolism. 2019; 21 :499-508. DOI: 10.1111/dom.13553 - 48.
Dalbøge LS, Christensen M, Madsen MR, Secher T, Endlich N, Drenic V, et al. Nephroprotective effects of semaglutide as mono- and combination treatment with lisinopril in a mouse model of hypertension-accelerated diabetic kidney disease. Biomedicines. 2022; 10 (7):1661. DOI: 10.3390/biomedicines10071661 - 49.
Mann JFE, Ørsted DD, Brown-Frandsen K, Marso SP, Poulter NR, Rasmussen S, et al. Liraglutide and renal outcomes in type 2 diabetes. The New England Journal of Medicine. 2017; 377 :839-848. DOI: 10.1056/nejmoa1616011 - 50.
Adel-Latif RG, Heeba GH, Taye A, Khalifa MMA. Lixisenatide, a novel GLP-1 analog, protects against cerebral ischemia/reperfusion injury in diabetic rats. Naunyn-Schmiedeberg's Archives of Pharmacology. 2018; 391 :705-717. DOI: 10.1007/s00210-018-1497-1 - 51.
You J, Manaenko A, Hakon J, Hansen-Schwartz J, Tang J, Zhang JH. Liraglutide, a long-acting GLP-1 mimetic, and its metabolite attenuate inflammation after intracerebral haemorrhage. Journal of Cerebral Blood Flow and Metabolism. 2012; 32 :2201-2210. DOI: 10.1038/jcbfm.2012.133 - 52.
Sattar N, McGuire DK, Pavo I, Govinda J, et al. Tirzepatide cardiovascular event risk assessment: A pre-specified meta-analysis. Nature Medicine. 2022; 28 :591-598. DOI: 10.1038/s41591-022-01707-4 - 53.
Knerr PJ, Mowery SA, Douros JD, et al. Next generation GLP-1/GIP/glucagon triple agonists normalize body weight in obese mice. Molecular Metabolism. 2022; 63 :101533. DOI: 10.1016/j.molmet.2022.101533