Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
Anal dysplasia, a precancerous condition of the anal canal, is increasingly recognized as a significant health concern, particularly among individuals with high-risk factors such as patients living with human immunodeficiency virus, men who have sex with men, a history of anogenital cancer, and immunosuppression. Screening for anal dysplasia has emerged as a critical measure for early detection and treatment, in order to prevent progression to invasive AC. This chapter provides an overview of anal dysplasia screening modalities, including anal cytology and high-resolution anoscopy, while discussing their benefits and limitations. The significance of risk stratification and prevention measures is also emphasized. The potential benefits of anal dysplasia screening in reducing the burden of anal cancer and improving patient outcomes are highlighted, along with the need for further research and comprehensive screening programs to optimize early detection and management of anal dysplasia.
Gastroenterology and Hepatology Department, Centro Hospitalar Universitário de São João, Porto, Portugal
World Gastroenterology Organization (WGO) Porto Training Center, Porto, Portugal
† Both authors contributed equally to the manuscript
João Afonso
Gastroenterology and Hepatology Department, Centro Hospitalar Universitário de São João, Porto, Portugal
World Gastroenterology Organization (WGO) Porto Training Center, Porto, Portugal
† Both authors contributed equally to the manuscript
Rosa Coelho
Gastroenterology and Hepatology Department, Centro Hospitalar Universitário de São João, Porto, Portugal
World Gastroenterology Organization (WGO) Porto Training Center, Porto, Portugal
Guilherme Macedo
Gastroenterology and Hepatology Department, Centro Hospitalar Universitário de São João, Porto, Portugal
World Gastroenterology Organization (WGO) Porto Training Center, Porto, Portugal
*Address all correspondence to: isabelmng@hotmail.com
1. Introduction
The anal cancer (AC) incidence has been rising in most of the developed countries, particularly in high-risk populations such as men who have sex with men (MSM), immunocompromised individuals, and patients infected with human papillomavirus (HPV) [1, 2]. Currently, the incidence of squamous cell carcinoma of the anus (SCCA) among MSM infected with human immunodeficiency virus (HIV) has surpassed the incidence of cervical cancer in women. Moreover, in contrast to other HIV-related neoplasia, the incidence of SCCA in patients living with HIV has been rising even after the advent of antiretroviral drugs, probably due to a longer life expectancy and an increase in the incidence of sexually transmitted infections (ISTs) [3, 4].
AC prevention works in two distinct phases. Primary prevention focuses on reducing the incidence of malignant and premalignant lesions, and secondary prevention focuses on the early diagnosis and treatment of those lesions [5].
Primary prevention can be accomplished through HPV vaccination. This should occur before HPV infection, at a targeted age of 11-12 years old, before sexual initiation. Adequate vaccination policies can prevent high-risk genotype infection, leading to a decrease of mucosal infection and reducing the carcinogenic cascade that is initiated by HPV infection [5].
Secondary prevention occurs through AC screening. Screening plays a major role in the early detection and prevention of AC and allows the timely diagnosis of precancerous lesions and early AC, thus enabling prompt intervention and treatment [5].
The first screening test, usually done through anal cytology, allows for the identification of high-risk patients. According to those results, patients with abnormal cytology are proposed to do a high-resolution anoscopy (HRA), which is the gold standard for the diagnosis and management of high-grade squamous intraepithelial lesions (HSIL) [6, 7].
This step-up approach allows for balanced resource management, limiting the number of patients that are submitted to a costly and time-consuming intervention and allowing for the monitoring of a higher number of patients.
The impact of AC screening was clearly demonstrated by the ANal Cancer/HSIL Outcomes Research (ANCHOR) trial, where patients living with HIV with anal HSIL were randomly assigned to receive treatment or active monitoring with HRA every 6 months. The primary endpoint was to evaluate the SCCA progression, and the study had to be terminated early due to a clear increase in SCCA in the monitoring group [5]. However, there is still some lack of information and guidelines on how to perform those screening programs.
Through this chapter, we intend to provide a practice-oriented and up-to-date review of the importance of AC screening with a brief description of the current guidelines published by several societies about AC screening programs. It reinforces who is most at risk and how screening should be performed. Finally, we describe the various treatment options for anal dysplasia, from topical therapies to surgical options.
AC is a relatively rare neoplasia with a worldwide incidence of 50,865 new cases per year, according to GLOBOCAN 2020. However, its incidence is rising worldwide, and it is estimated that in the USA alone, the number of new cases per year doubled from 2001 to 2015. This can be partially justified by STIs, including HPV infection, and the longer overall survival of people living with HIV [8].
The incidence of SCCA is not homogenously distributed throughout the population. There are some groups of individuals presenting with a higher risk of developing AC. HIV-infected patients, MSM, women with HPV-related gynecologic lesions, or solid-organ transplant recipients present a much higher incidence of SCCA and so represent a particularly important subset of individuals when referring to AC screening [9].
The highest risk group has been consistently demonstrated in different studies to be the group of patients that combined HIV infection and MSM, showing a synergistic effect between these two risk factors [9].
Before the HIV epidemic, it was estimated that the rate of AC MSM was as high as 37 cases per 100,000 individuals [10]. This incidence was comparable to the rate of cervical cancer in women before the introduction of cervical Papanicolaou smear screening. In HIV-positive MSM, the incidence of AC has been estimated to be roughly double that of HIV-negative MSM [11].
Moreover, compared to other cancers commonly found in HIV-positive individuals, such as Kaposi sarcoma and non-Hodgkin lymphoma, the occurrence of AC has not decreased with the advancement of potent antiretroviral therapy. As a matter of fact, a study demonstrated that the incidence of AC in males aged 40 to 64 years more than quadrupled from the pre-HIV era to the present era, despite the availability of effective antiretroviral therapy. Rates rose especially dramatically for San Francisco men ages 40 to 64, from 3.7 cases per 100,000 in 1973-1978 to 8.6 cases per 100,000 in 1984-1990 and 20.6 cases per 100,000 in 1996-1999 [12].
Other immunosuppressive conditions such as solid-organ transplant recipients or some patients with autoimmune diseases may have a similar effect, mainly due to a higher HPV replication [9].
Less is known about the epidemiology and natural history of SCCA in patients with inflammatory bowel disease. A systematic review that included 11 studies from 1940 to 2005 revealed that the incidence of SCCA was 0.02 per 1000 patient-years in patients with Crohn’s disease and 0.009 per 1000 patient-years in patients with ulcerative colitis, similar to that of the general population [13]. The majority of the cases were diagnosed in the context of long-standing Crohn’s disease (>10 years) and underlying chronic perianal disease. Indeed, patients with chronic perianal Crohn’s disease may be at increased risk of developing SCCA [14]. However, studies are scarce and have conflicting results [15].
3. Current guideline recommendations for AC screening
The level of evidence on the different guidelines addressing this issue is generally low, with some of the statements resulting from expert opinions without clear data supporting them. However, some general rules are common to the different organizations that issued guidelines on the topic.
The low prevalence of AC in the general population is low and so, no organization recommends a global screening program outside the scope of high-risk populations.
Therefore, the screening programs are restricted to high-risk groups such as people living with AIDS (PLW), MSM, and women with genital HPV-related lesions. There is not enough evidence to include immunocompromised patients without other risk factors in the screening program, so no organization recommends routine screening of those patients.
Most guidelines do not specify the screening starting age, except the guidelines issued by the New York State Department of Health AIDS Institute (NYSDHAI) on March 2020 that stated that screening should start annually at 35 years old in every HIV-positive patient and before that, only in the presence of anal signs or symptoms [16]. In Table 1, the authors resumed the latest and most important guidelines about AC screening.
Society
Title
Year
Patient populations
Screening methodology
Age
American Society of Colon & Rectal Surgeons (ASCRS) [17]
Anal cytology: Considered in high-risk patients with or without HPV testing
Not defined
American Society of Transplantation Infectious Diseases Community of Practice (ASTIDCP) [18]
“Human papillomavirus infection in solid-organ transplant recipients: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice”
2019
Solid-organ transplant recipients if there is a history of receptive anal intercourse or cervical dysplasia.
Anal cytology:
If normal repeat for 1-3 years
If abnormal, perform HRA
Not defined
AIDS Study Group (GeSIDA) of the Spanish Society of Infectious Diseases and Clinical Microbiology [19]
“Executive summary of the GeSIDA consensus document on control and monitoring of HIV-infected patients”
Anal symptoms inquiry; Anal examination and digital anorectal examination (DARE) in every PLWH; Anal cytology in high-risk patients HRA if abnormal cytology
NA
HIV Medicine Association of the Infectious Diseases Society of America (HIVMA/IDSA) [20]
“Primary Care Guidance for Persons With Human Immunodeficiency Virus: 2020 Update by the HIV Medicine Association of the Infectious Diseases Society of America”
2020
PLWH; PLWH + risk factors: Receptive anal intercourse Abnormal Pap test Genital wards
Cytology in high-risk patients HRA if abnormal cytology
NA
New York State Department of Health AIDS Institute. (NYSDHAI) [16]
“Screening for Anal Dysplasia and Cancer in Adults With HIV”
2020
PLWH
AC screening in every patient - > Decision on cytology, patient based; HRA if abnormal cytology
≥35 years old
Table 1.
Guidelines recommendations regarding AC screening.
AC—anal cancer; HPV—human papillomavirus; HIV—human immunodeficiency virus; HPV—human papillomavirus; HIV—human immunodeficiency virus; NA—Not applicable; PLWH—People living with HIV.
Also, the screening method varies between societies (Table 1), but most state that visual inspection and digital anorectal examination (DARE) should be done yearly, and cytology should also be performed in centers with HRA availability.
In case of abnormal pathological results, patients should undergo HRA and biopsy if possible, and visible lesions should be managed accordingly.
Many risk factors for anal squamous intraepithelial lesions and AC are described, such as sexual behavior, HIV, and iatrogenic immunosuppression. Table 2 provides an overview of the patient populations that are most vulnerable to developing AC.
AC incidence in women vs. men: 2.52 versus 1.26 per 100,000 people
Table 2.
Risk factors and the estimated risk or IR of developing AC according to each group.
CD—Crohn’s disease; HIV—human immunodeficiency virus; IR—incidence rates; MSMLWH—Male sex male who are living with HIV; MLWH—males living with HIV; RR—relative risk; SLE—systemic lupus erythematosus; SIL—squamous intraepithelial lesions; UC—ulcerative colitis.
The screening benefit and risk ratio for detecting anal HSIL has not been established for any of the groups listed in this table. However, recently the ANCHOR trial, as previously described, strongly supports the importance of screening and early identification of HSIL in high-risk individuals [5].
4.1 People living with HIV (PLWHIV)
It is not clear whether HIV infection itself has a direct effect on the development of AC or if this is mediated through HPV infection. However, the incidence of dysplastic lesions and AC is higher in males living with HIV (MLWH), particularly MSM who are living with HIV. It has also been demonstrated that PLWHIV has a higher risk of progression from low-grade squamous intraepithelial lesions (LSIL) to HSIL and AC [9]. It is also important to emphasize that the incidence of HPV infection and HPV-associated preinvasive and invasive malignancy is higher in PLWH, regardless of sexual practice [26]. Moreover, a meta-analysis that included a total of 53 studies showed that the prevalence of both high-risk anal HPV subtypes and AC was significantly higher among MSMLWH as compared with MSM without HIV [3].
4.2 MSM
There have been multiple studies showing a high prevalence of anal HSIL in MSM, both with and without HIV. In fact, MSM are considered at increased risk of developing AC compared with males who do not have sex with men. Moreover, the number of sexual partners and a history of anal-receptive intercourse are associated with anal SIL in this population [18].
4.3 HPV-related gynecological diseases
Women with HPV-related gynecological precancerous lesions or cancer are those in which HPV plays a significant role in the pathophysiology. This group includes cervical cancer, which is nearly entirely dependent on HPV infection, and vaginal and vulvar cancer, which are related to HPV infection in about 78 and 24.9% of cases, respectively, along with the corresponding precancerous lesions [21]. Women with a history of HPV-related disease have a significantly increased risk of anal intraepithelial neoplasia (AIN) and AC. Survivors of vulvar cancer have the highest risk of developing AC, followed by vaginal survivors and cervical cancer survivors. In light of this information, it is evident that patients who have received treatment for HPV-related diseases should be closely monitored to prevent the occurrence of another HPV-related illness [27].
4.4 HPV infection
The most commonly diagnosed sexually transmitted infection in the USA is HPV infection, and there is a close link between HPV infections, particularly patients infected with high oncogenic strains, such as HPV 16 and 18, and the development of genital and AC. Epidemiologic studies link more than 90% of squamous cell carcinoma cases to HPV infection, and their presence is higher in patients with concomitant HIV infection [9]. Therefore, it is not surprising that there is a strong correlation between the presence of anal squamous intraepithelial lesions and the prevalence of anal HPV infection. Studies have shown that as the severity of anal SIL increase, the prevalence of HPV also increases. Specifically, HPV type 16 is strongly associated with high-grade SIL and invasive AC [28].
However, it is important to highlight that HPV infection is necessary but insufficient for the development of squamous intraepithelial lesions, including HSIL. Moreover, not all cases of anal HPV infection, including those with high-risk (hr)-HPV types, result in anal squamous intraepithelial lesions [29]. Therefore, a full understanding of the factors that dictate the development of HSIL in the presence of hr-HPV infection remains elusive.
4.5 Genital warts
A longitudinal cohort study of 6515 PLWHIV concluded that a previous history of anogenital warts is associated with a higher risk of developing AC. After adjusting for covariates, the odds of developing AC were 12.79 (95% CI, 6.19-26.45; P < .001) times higher in individuals with a history of anogenital warts compared with individuals without a history of anogenital warts [22]. Moreover, it seems that the presence of perianal warts is a suitable risk marker for anal HPV 16 detection and anal dysplasia [30].
4.6 Iatrogenic immunosuppression
Solid-organ transplant recipients: Other causes of chronic immunosuppression, such as solid-organ transplantation, also may be associated with the development of high-grade SIL and invasive AC. For example, among renal transplant recipients, the risk of anogenital cancer has been associated with persistent HPV infection [31, 32].
Other immunocompromised individuals without HIV infection: Autoimmune diseases such as inflammatory bowel disease and systemic lupus erythematosus seem to be a risk factor for AC, probably due to chronic glucocorticoid therapy [21].
4.7 Smoking
It increases the risk of developing AC. In fact, several case–control studies demonstrated a statistically significant risk of AC in smokers, especially current smokers [33]. In one series, cigarette smoking was associated with a significantly increased risk of AC. Moreover, cigarette smoking is highly associated with cervical neoplasia and is thought to act as a cocarcinogen for anogenital squamous cell carcinoma [34].
4.8 Gender
AC incidence is the highest in women compared to men and is rising more rapidly in women compared to men (28.6 versus 13.5%, respectively), considering data from England between 2013 and 2017 [25]. Moreover, females are more likely to present late with advanced cancers, taking into consideration data from the Surveillance, Epidemiology and End Results Program (SEER) demonstrated that women are more likely to present with advanced staging, receive radiotherapy, and die of AC [35].
5. Screening techniques: from anal cytology to HRA
Anal HSIL is typically a not palpable lesion; therefore, it is unlikely to be diagnosed or suspected on routine DARE. The AC screening programs have relied on cytology as the initial screening examination. In the presence of an abnormal cytology result (e.g., LSIL, atypical squamous cells of undetermined significance (ASCUS) or HSIL), the anal canal and perianal area should be observed with HRA in order to identify areas of potential HSIL that should be confirmed by biopsy. These precancerous lesions could be properly treated to prevent AC.
It is crucial to note that screening should only be offered to at-risk populations if there is local expertise in interpreting screening results and if there is a referral system in place for HRA with biopsy, as well as access to ablative treatments and follow-up care.
5.1 Anal cytology
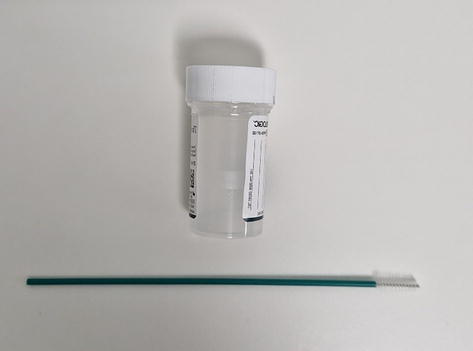
This procedure involves the insertion of a swab in the anal canal (without direct visualization), allowing the collection of epithelial cells from the lower rectum, squamocolumnar transformation zone, and anal canal. It is typically done using a moistened polyester fiber swab (Figure 1), which is preferred over a cotton swab because it releases the collected cells more easily and has a plastic shaft that does not break during the procedure. In fact, it is not advisable to use cotton swabs with marked or wooden sticks because they may fracture.
Figure 1.
Polyester fiber swab and transport medium.
After insertion of the swab, the cloth is removed with sideways force, employing a rotating movement to obtain samples from all sides of the anal canal, and then, the material is transferred to a liquid transport medium (ethanol or processed using a liquid cytology technique) to be analyzed.
To obtain the maximum number of cells and preserve their original appearance, anal cytology sampling should be conducted before DARE or anoscopy.
The cytological changes are reported using the Bethesda nomenclature, as negative for squamous intraepithelial lesions (NILM), atypical squamous cells of undetermined significance (ASCUS), low-grade SIL (LSIL), atypical squamous cells cannot exclude high-grade SIL (ASC-H), and high-grade SIL (HSIL) [36].
Although clinician-collected samples are the standard practice, self-collected anal cytology may be an option to increase patient compliance and reduce the cost of screening. However, a study performed to compare these two procedures concluded that the sensitivity of cytology to detect AIN is higher for clinician-collected versus self-collected specimens [37].
A recent systematic review and meta-analysis that included a total of 18 studies described the performance of anal cytology (any abnormality as a threshold) to detect HSIL, in PLWH, with a sensitivity of 82% and specificity of 45% [38]. The positive predictive value was 36%, and the negative predictive value was 87%. These results align with previous studies that consider any cytologic abnormality, including ASCUS, as a referral threshold for HRA [38]. However, limited resources prevent HRA from being performed on all at-risk individuals. Therefore, cytology helps to prioritize those who would benefit most from HRA, starting with individuals with HSIL and then those with LSIL.
5.2 High-resolution anoscopy
It should be performed after an abnormal anal cytology screening test to visualize the anal and perianal regions using a colposcope (Figure 2). Compared with cervical colposcopy, HRA presents several additional challenges such as uneven topography, obscuring of lesions due to hemorrhoids, folds or presence of stools, or lesions being located at the base of folds and anal glands. Therefore, a long learning curve is typically required before becoming fully competent in this technique [39].
Figure 2.
Colposcope: High-resolution mobile microscope.
HRA is usually performed without previous bowel preparation in the left lateral position (fetal position); however, other positions are acceptable as well. After the insertion of an anoscope, a systematic inspection of the squamocolumnar junction, the anal canal, and the perianal skin with no staining should be performed.
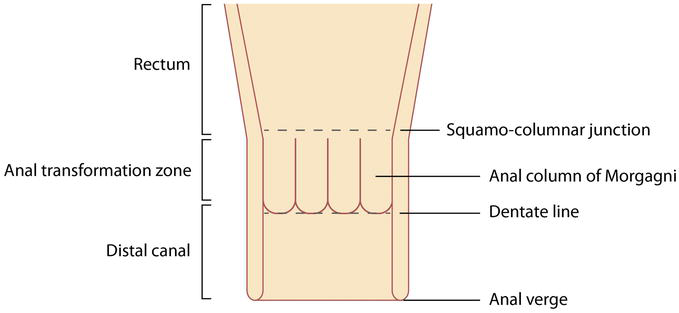
Figure 3 illustrates that the anal canal is divided into distal/proximal regions: distal rectum, squamocolumnar junction, dentate line, mid-canal, distal canal, and anal verge. The perianal skin should also be visualized by gentle retraction of the buttocks and is considered the area that extends 5 cm laterally from the anal margin [40].
Figure 3.
Basic anatomy of the ana canal.
Subsequently, in order to aid detection of lesions that represent the source of abnormal cells on cytology screening a 4 × 4 gauze swab with acetic acid (3 or 5%) and Lugol iodine solutions should be applied. The anal verge is viewed with 10× magnification, but most of the visualization of the anal canal is done under 16× magnification. Specific areas of interest can be observed under 25× magnification for better characterization [40].
The anoscopic changes most often associated with HSIL include acetowhite change (acetic acid produces a white appearance in areas of abnormal transitional epithelium) on flat/slightly raised or thickened epithelium, with or without abnormal blood vessels (mosaic pattern/punctuation). Regarding Lugol iodine staining, lesions considered highly suspicious for HSIL do not take up Lugol stain.
After the HRA technique, a detailed report should be performed describing all highly suspicious lesions observed and those that were submitted to macrobiopsy. Lesions must be described concerning localization that must be independent of the position of the patient. The use of “o’clock” terminology should be avoided wherever possible as it depends on the patient’s position (left lateral, prone, or lithotomy position). Therefore, the correct description must include the following topographies: anterior, posterior, left/right lateral, or left/right anterior/posterior. Lesion location can additionally be recorded in the anal canal concerning its proximal/distal extent as at/near the squamocolumnar junction, mid-canal, distal canal, and perianal area. Lesions should also be described considering contour, margins, acetic acid-induced whitening, Lugol’s staining, epithelial pattern, and vascular pattern (mosaic pattern, punctation, warty vessels, and atypical) [40].
5.3 Molecular diagnostics
Despite the potential of molecular diagnostic tests like hr-HPV DNA detection, HPV E6/E7 mRNA analysis, and P16INK4a and Ki-67 immunostaining, their superiority over anal cytology in diagnosing anal HSIL has not been proven in the most studied risk groups (MSM and MSMLWH). Thus, their use is not recommended in these populations. However, these tests may be more effective in other at-risk groups with a lower prevalence of anal hr-HPV. In such cases, a significant number of individuals would test negative for hr-HPV and would not require further evaluation.
Considering the limitations of anal cytology, there has been significant interest in using molecular techniques to identify anal HSIL. Testing for hr-HPV subtypes has been extensively researched; however, it does not seem to improve HSIL detection and should not replace anal cytology as a standard screening test for HIV-infected MSM [41]. Moreover, a meta-analysis published in 2019 showed that hr-HPV DNA detection had poor specificity and positive predictive value, making it unsuitable for triage [38]. Recently, Chiao EY et al. demonstrated that 2 hr-HPV tests (Aptima and Hybrid Capture 2 method) showed similar sensitivity to abnormal anal cytology in predicting anal HSIL in females with HIV [42].
Besides not being included in AC screening techniques, it is important to highlight the value of patient education. Healthcare providers should educate high-risk individuals about the signs and symptoms of AC, emphasizing the importance of reporting any abnormalities promptly. Common symptoms may include anal bleeding, persistent anal itching, pain or pressure in the anal area, and changes in bowel habits.
6. Interpretation of screening results: how to manage a patient
Anal dysplasia screening has relied on cytology as the initial screening test. Cytology is reported, in order of increasing severity, as negative for squamous intraepithelial lesions, atypical squamous cells of undetermined significance (ASCUS), low-grade squamous intraepithelial lesions (LSIL), and high-grade squamous intraepithelial lesions (HSIL).
Anal cytology has a sensitivity of 70% for the detection of squamous intraepithelial lesions or the presence of any abnormality [43]. However, it has a low specificity (34%) for HSIL prediction in a subsequent biopsy, meaning it cannot determine that the lesion will not be high-grade on histology. Indeed, a cytologic diagnosis of ASCUS and LSIL may have a significant risk (60 to 91%) of anal high-grade dysplasia at biopsy [44].
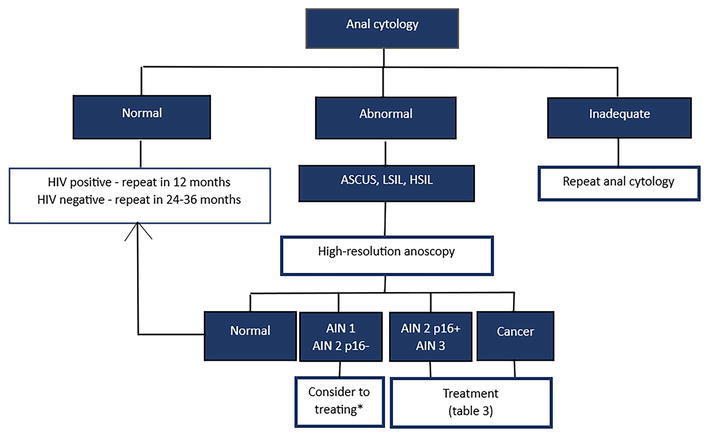
Therefore, an abnormal anal cytology screening test should be followed by an HRA for a diagnostic biopsy [16]. The grading of anal intraepithelial neoplasia (AIN) can only be performed by histopathological examination. AIN I and AIN II refer to nuclear abnormalities confined to the lower one-third and lower two-thirds of the epithelium, respectively, and these lesions are considered to be low-grade dysplasia. AIN III is full-thickness involvement of the epithelium and represents high-grade dysplasia or carcinoma in situ. Treatment should be started according to the results obtained (vide infra). On the other hand, abnormal anal cytology test results without abnormal histology should prompt repeat cytologic testing (Figure 4).
Figure 4.
Algorithm for anal dysplasia screening. HIV—Human immunodeficiency virus, ASCUS—Atypical squamous cells of undetermined significance, LSIL—Low-grade squamous intraepithelial lesions, HSIL—High-grade squamous intraepithelial lesions, AIN—Anal intraepithelial neoplasia. *if the patient has symptoms (burning, itching, bleeding) or anxiety about the conservative strategy.
It is also important to note that screened individuals with normal anal cytology should repeat anal cytology at regular intervals: annually in HIV-positive patients and less frequently in HIV-negative individuals [45].
The optimal management of AIN is difficult to determine as data on the relative efficacy of different treatment agents are limited. The decision to treat and the form of treatment also depend on the size of the lesion, the location of the lesion and the goals of treatment.
Usually, low-grade dysplasia (AIN I and AIN II p16-negative) is managed expectantly with regular follow-up [46, 47]. This conservative approach is based on the overall low rate of disease progression to invasive cancer and the increased morbidity associated with local excision. Recommendations on surveillance strategies are discordant, ranging from a 6-monthly physical examination to an annual anoscopy with biopsy [48]. Nevertheless, if the patient has symptoms (burning, itching, bleeding) or anxiety about the conservative strategy, treatment may be performed. On the other hand, when high-grade lesions are identified (AIN 2 p16-positive and AIN 3), treatment is indicated due to a higher risk of progression for cancer.
Treatment aims to minimize symptoms and prevent the development of AC [49]. It may include immunomodulation therapies, ablative therapies, or surgical excision, which should be performed by a clinician with expertise in managing anal dysplasia (Table 3).
Advantages
Disadvantages
Topical therapies
Imiquimod (5%) cream
Topical treatment self-applied by patient
Off-label use Limited data
5-fluorouracil (5%) cream
Topical treatment self-applied by patient
Off-label use
Topical trichloroacetic acid
Safe during pregnancy
Off-label use Repeated office visits Useful only for small lesions or nonbulky disease
Ablative therapies
Electrocautery/hyfrecation
Less serious side effects compared with topical treatments
High recurrence rate
Infrared coagulation
Effective procedure
More serious adverse side effects High rates of persistent HSIL and metachronous lesions
Argon plasma coagulation
Effective and safe procedure
High recurrence rate Equipment cost
Radiofrequency ablation
Lower rates of recurrence
Limited data
Cryotherapy
Mild side effects
High recurrence rate
Surgery
Treatment choice for carcinoma in situ
Risk of anal stenosis More morbidity associated
Table 3.
Treatment of anal squamous intraepithelial lesions.
7.1 Immunomodulation therapies
Topical therapies are commonly used off-label to treat HSIL. Although there are many potential side effects of local therapies, most are very well tolerated, with only minimal symptoms experienced by the patient.
Imiquimod, 5% cream, is an immune modulator that has pro-inflammatory, antitumor, and antiviral activity through several subcellular mechanisms [50]. There are limited reports describing the efficacy of imiquimod for the treatment of anal HSIL. Nevertheless, patient-applied imiquimod appears to have efficacy against anal HSIL and is available by prescription [51]. In fact, it has been advocated by the majority of guidelines [46, 52, 53].
Topical 5-fluorouracil cream is a pyrimidine analog, which inhibits DNA synthesis through the inhibition of the enzyme thymidylate synthase in neoplastic tissue. The most commonly used concentration for the treatment of anal HSIL is 5%. It causes erythema and edema followed by erosion, ulceration, and necrosis. It has been shown to preferentially treat neoplasms with only an inflammatory response on adjacent healthy skin. In addition, 5-fluorouracil has shown a good initial clinical response in the treatment of HSIL (59%), but recurrence may occur in up to 50% [54].
Topical trichloroacetic acid is caustic and corrodes the skin and mucous membranes. It treats HSIL by denaturing and precipitating proteins, resulting in tissue destruction [55]. Trichloroacetic acid is provider-applied in the office setting and has the advantage over other topical treatments of not requiring patient adherence other than repeated office visits for treatments. Four or five applications are typically needed to completely treat the lesion, usually spaced 3-4 weeks apart. Topical application of trichloroacetic acid is generally well tolerated but can occasionally be painful. It is the only topical treatment that is safe to use in pregnancy. However, trichloroacetic acid is unlikely to be effective in treating extensive or bulky diseases.
7.2 Ablative therapies
Ablative therapies include electrocautery/hyfrecation, argon plasma coagulation, infrared coagulation, cryotherapy, and radiofrequency ablation. Many of these therapies suffer from high recurrence rates, perhaps due to the persistence of HPV infection and because of the deep involvement of the perianal skin, which cannot be cleared by ablation.
Electrocautery is currently the treatment of choice for intra-anal HSIL in many centers. In an open-label randomized trial, Richel and colleagues showed that 58% of patients with AIN treated with electrocautery achieved a complete or partial response [56]. Indeed, electrocautery ablation of high-grade anal intraepithelial neoplasia is a safe office-based procedure. In addition, electrocautery was found to have less serious side effects, which were shorter in length in comparison with 5-fluorouracil cream and imiquimod. However, recurrence rates are substantial. For example, in a study of electrocautery in HIV-positive men, the recurrence rate was found to be 79% in 12 months, with an estimated recurrence risk approaching 100% by 50 months [57]. A separate study noted the following risk factors for persistent HSIL following hyfrecation: multiple index lesions, HIV viremia, cigarette smoking, and the presence of HPV-16/18 DNA [58].
Argon plasma coagulation can also be used to treat anal HSIL. A pilot study showed that argon plasma coagulation is comparable to other treatment modalities in terms of efficacy and safety in anal HSIL [59]. However, it requires repeated treatment because of a high recurrence rate. Pain is the main side effect, which requires appropriate attention and analgesia to be given to the patient during the procedure and in the following week.
Treatment of anal HSIL with infrared coagulation consists of the direct application of a pulse of irradiation in the infrared range to the anal epithelium, which results in tissue destruction. Depth of destruction is controlled by the length of pulse and healing occurs with minimal scarring. Possible procedure-related complications include immediate and delayed bleeding and infection. Multiple studies have demonstrated the safety and efficacy of infrared coagulation in patients with HSIL. For example, an open-label, randomized, multisite clinical trial of human HIV-infected adults proved that infrared coagulation ablation of anal canal HSIL was more likely to result in complete or partial resolution than active monitoring alone (62 vs. 30% at 1 year, risk difference 32, 95% CI 13-48%) [60]. It is worth noting, however, the relatively high rates of persistent HSIL within the treatment group at 1 year and the high number of metachronous HSIL.
Cryotherapy is an old technique that consists of office-based-guided liquid nitrogen application using a spray gun. It is capable of clearing HSIL. In fact, treatment success rates are comparable with those reported for current treatment modalities [61]. Side effects are common but mostly mild, of which anal pain or tenderness and mild blood loss are reported most frequently. Similar to other ablative therapies, HSIL recurrences are frequent (68%).
Radiofrequency energy delivered via electrodes creates a very superficial injury to the mucosa. It was effective in a small study performed at a single center [62]. However, studies of larger numbers of patients in different centers need to be performed before this technique is widely adopted in the field.
7.3 Surgery
A local surgical approach may be appropriate for selected small lesions and for carcinoma in situ [46]. Localized or focal AIN is defined as <30% anal circumference involved, whereas extensive AIN involves more than 30% circumference. Localized or focal AIN can be simply excised with the resulting wound left to granulate or sutured as appropriate. AIN III lesions involving more than 30% of the anal margin or canal cannot be excised as the risk of severe anal stenosis is significant, but excision of the most symptomatic area is possible. The remaining areas can then be observed at regular follow-up intervals.
Most studies describe preoperative mapping before excision, but this does not preclude recurrence. Indeed, recurrence of AIN III after local excision may appear to be more likely when resection margins are incomplete, but recurrence may occur even after microscopically complete excision. It is also important to note that aggressive treatment such as wide local excision can result in significant morbidity and therefore conservative management has been favored.
7.4 Chemoradiotherapy
Radiotherapy with concurrent chemotherapy is the current standard of care for patients with localized squamous cell cancer of the anal canal. The British guidelines state that extensive AIN III and AIN II at the margin of invasive cancers treated by chemoradiation disappear, suggesting that this treatment may have a place in patients with extensive AIN but risks causing anal stenosis [46]. Nevertheless, there is currently no literature on its use in AIN.
7.5 Anal cancer
The management of AC is beyond the scope of this chapter. Treatment modalities for AC may include radiation therapy, chemotherapy, excision, or combined modalities. The recommendations on the management of AC include the ESMO Clinical Practice Guidelines [63] and the American Society of Colon and Rectal Surgeons Clinical Practice Guidelines [17].
7.6 Surveillance
Due to the high rates of recurrence and evolving anal squamous intraepithelial lesions, surveillance is required following initial treatment. The appropriate follow-up of these patients remains an active area of investigation. Some authors suggest a follow-up in 4-6 months, including a repeat biopsy of the treatment site if there is lesion persistence. Anal cytology may also be useful as an adjunctive test to confirm lesion clearance [16].
8. Emerging trends and future directions in AC screening
A significant barrier to establishing recommendations for AC screening is the lack of evidence showing that it can reduce AC-associated morbidity and mortality. There are also few trials evaluating the efficacy of current treatment modalities as well as potential side effects and complications. Cost-effectiveness studies are also needed to justify implementing screening programs.
Identifying individuals at the highest risk of developing AC is crucial for effective screening. Researchers are exploring various risk stratification models based on factors such as HPV status, HIV infection, sexual behaviors, and immune status. These models aim to optimize screening protocols by tailoring them to individuals with the greatest likelihood of developing AC. Targeted screening strategies have the potential to improve the efficiency and cost-effectiveness of screening programs.
Screening for HPV infection has gained considerable attention as a potential method for early detection and prevention of AC [64]. Current research focuses on optimizing HPV testing methods and developing new approaches such as self-sampling kits for individuals who may feel uncomfortable with traditional sampling techniques. These advancements aim to increase screening uptake and improve the accuracy of HPV detection, ultimately reducing the burden of AC.
Advancements in imaging technologies, such as optical coherence tomography and molecular imaging, are being explored for their potential role in AC screening [65, 66]. These techniques offer noninvasive and real-time visualization of the anal canal, enabling the detection of early-stage lesions. Additionally, the identification of specific biomarkers associated with AC may aid in risk assessment and screening [67]. Ongoing research focuses on identifying reliable biomarkers that can be detected through minimally invasive methods.
As AC is strongly linked to HPV infection, the widespread administration of HPV vaccines presents an opportunity for primary prevention [68]. While HPV vaccination has primarily been promoted for the prevention of cervical cancer, its potential impact on AC prevention is significant. By reducing the prevalence of high-risk HPV infections, widespread HPV vaccination has the potential to substantially decrease the incidence of AC, particularly among populations at higher risk. Integrating HPV vaccination efforts with AC screening programs can further enhance the effectiveness of prevention strategies. Vaccination can complement screening by reducing the number of high-risk HPV infections, thereby lowering the incidence of precancerous and cancerous lesions in the anal canal. This combination approach of vaccination and screening holds promise for a comprehensive approach to AC prevention.
Continued research and collaboration between healthcare professionals, researchers, and policymakers are crucial to ensure the successful implementation of these emerging trends and the reduction of the global burden of AC.
Anal dysplasia screening plays a crucial role in the early detection and prevention of AC, particularly in high-risk populations. Identification of precancerous lesions will probably allow for a reduction in the incidence and mortality associated with AC. Anal cytology and high-resolution anoscopy have emerged as valuable tools for early detection and screening of this type of cancer. These methods have shown promise in identifying precancerous lesions and can guide further management, including the use of ablative or surgical treatments.
The implementation of anal dysplasia screening programs requires not only increased awareness among healthcare providers and patients but also the development of standardized guidelines for screening and management. Additionally, addressing barriers such as stigma, discomfort, and lack of knowledge is essential in promoting wider acceptance and uptake of screening practices. Through collaborative efforts and a commitment to research, we can make significant progress in preventing and managing anal dysplasia, thereby improving the health outcomes of at-risk populations.
References
1.Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA: A Cancer Journal for Clinicians. 2023;73(1):17-48
2.Damgacioglu H, Lin YY, Ortiz AP, Wu CF, Shahmoradi Z, Shyu SS, et al. State variation in squamous cell carcinoma of the anus incidence and mortality, and association with HIV/AIDS and smoking in the United States. Journal of Clinical Oncology: Official Journal of the American Society of Clinical Oncology. 2023;41(6):1228-1238
3.Machalek DA, Poynten M, Jin F, Fairley CK, Farnsworth A, Garland SM, et al. Anal human papillomavirus infection and associated neoplastic lesions in men who have sex with men: A systematic review and meta-analysis. The Lancet Oncology. 2012;13(5):487-500
4.Silverberg MJ, Lau B, Achenbach CJ, Jing Y, Althoff KN, D’Souza G, et al. Cumulative incidence of cancer among persons with HIV in North America: A cohort study. Annals of Internal Medicine. 2015;163(7):507-518
5.Barroso LF, Stier EA, Hillman R, Palefsky J. Anal cancer screening and prevention: Summary of evidence reviewed for the 2021 centers for disease control and prevention sexually transmitted infection guidelines. Clinical Infectious Diseases: An Official Publication of the Infectious Diseases Society of America. 2022;74(Suppl_2):S179-SS92
6.Bean SM, Chhieng DC. Anal-rectal cytology: The other PAP test. Laboratory Medicine. 2010;41(3):168-171
7.Darragh TM, Colgan TJ, Thomas Cox J, Heller DS, Henry MR, Luff RD, et al. The lower Anogenital squamous terminology standardization project for HPV-associated lesions: Background and consensus recommendations from the College of American Pathologists and the American Society for Colposcopy and Cervical Pathology. International Journal of Gynecological Pathology: Official Journal of the International Society of Gynecological Pathologists. 2013;32(1):76-115
8.Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer Journal for Clinicians. 2021;71(3):209-249
9.Islami F, Ferlay J, Lortet-Tieulent J, Bray F, Jemal A. International trends in anal cancer incidence rates. International Journal of Epidemiology. 2017;46(3):924-938
10.Daling JR, Weiss NS, Klopfenstein LL, Cochran LE, Chow WH, Daifuku R. Correlates of homosexual behavior and the incidence of anal cancer. Journal of the American Medical Association. 1982;247(14):1988-1990
11.Melbye M, Coté TR, Kessler L, Gail M, Biggar RJ. High incidence of anal cancer among AIDS patients. The AIDS/cancer working group. Lancet (London, England). 1994;343(8898):636-639
12.Cress RD, Holly EA. Incidence of anal cancer in California: Increased incidence among men in San Francisco, 1973-1999. Preventive Medicine. 2003;36(5):555-560
13.Slesser AA, Bhangu A, Bower M, Goldin R, Tekkis PP. A systematic review of anal squamous cell carcinoma in inflammatory bowel disease. Surgical Oncology. 2013;22(4):230-237
14.Wisniewski A, Fléjou JF, Siproudhis L, Abramowitz L, Svrcek M, Beaugerie L. Anal neoplasia in inflammatory bowel disease: Classification proposal, epidemiology, carcinogenesis, and risk management perspectives. Journal of Crohn's & Colitis. 2017;11(8):1011-1018
15.Frisch M, Johansen C. Anal carcinoma in inflammatory bowel disease. British Journal of Cancer. 2000;83(1):89-90
16.Hirsch BE, McGowan JP, Fine SM, Vail R, Merrick ST, Radix A, et al. New York State Department of Health AIDS institute clinical guidelines. In: Screening for Anal Dysplasia and Cancer in Adults with HIV [Internet]. Baltimore (MD): Johns Hopkins University; 2022 Aug 9
17.Stewart DB, Gaertner WB, Glasgow SC, Herzig DO, Feingold D, Steele SR. The American Society of Colon and Rectal Surgeons clinical practice guidelines for anal squamous cell cancers (revised 2018). Diseases of the Colon and Rectum. 2018;61(7):755-774
18.Chin-Hong PV, Reid GE. Human papillomavirus infection in solid organ transplant recipients: Guidelines from the American Society of Transplantation infectious diseases community of practice. Clinical Transplantation. 2019;33(9):e13590
19.AIDS Study Group (GeSIDA) of the Spanish Society of Infectious Diseases and Clinical Microbiology. Executive summary of the GeSIDA consensus document on control and monitoring of HIV-infected patients. Enfermedades Infecciosas Microbiologia Clinica (English ed). 2019;37(7):467-475
20.Thompson MA, Horberg MA, Agwu AL, Colasanti JA, Jain MK, Short WR, et al. Primary care guidance for persons with human immunodeficiency virus: 2020 update by the HIV medicine association of the infectious diseases society of America. Clinical infectious Diseases: An Official Publication of the Infectious Diseases Society of America. 2021;73(11):e3572-ee605
21.Clifford GM, Georges D, Shiels MS, Engels EA, Albuquerque A, Poynten IM, et al. A meta-analysis of anal cancer incidence by risk group: Toward a unified anal cancer risk scale. International Journal of Cancer. 2021;148(1):38-47
22.Arnold JD, Byrne ME, Monroe AK, Abbott SE. The risk of anal carcinoma after anogenital warts in adults living with HIV. JAMA Dermatology. 2021;157(3):283-289
23.Holly EA, Whittemore AS, Aston DA, Ahn DK, Nickoloff BJ, Kristiansen JJ. Anal cancer incidence: Genital warts, anal fissure or fistula, hemorrhoids, and smoking. Journal of the National Cancer Institute. 1989;81(22):1726-1731
24.Deshmukh AA, Suk R, Shiels MS, Sonawane K, Nyitray AG, Liu Y, et al. Recent trends in squamous cell carcinoma of the anus incidence and mortality in the United States, 2001-2015. Journal of the National Cancer Institute. 2020;112(8):829-838
25.Brogden DRL, Kontovounisios C, Mandalia S, Tekkis P, Mills SC. The role of demographics, social deprivation and ethnicity on anal squamous cell carcinoma incidence in England. Journal of Clinical Medicine. 2021;10(16):3621
26.Critchlow CW, Surawicz CM, Holmes KK, Kuypers J, Daling JR, Hawes SE, et al. Prospective study of high grade anal squamous intraepithelial neoplasia in a cohort of homosexual men: Influence of HIV infection, immunosuppression and human papillomavirus infection. AIDS (London, England). 1995;9(11):1255-1262
27.Brzeziński M, Stukan M. Anal cancer and anal intraepithelial neoplasia risk among patients treated for HPV-related Gynecological diseases—A systematic. Review. 2023;12(13):4216
28.Lin C, Franceschi S, Clifford GM. Human papillomavirus types from infection to cancer in the anus, according to sex and HIV status: A systematic review and meta-analysis. The Lancet Infectious Diseases. 2018;18(2):198-206
29.Wilkin TJ, Chen H, Cespedes MS, Leon-Cruz JT, Godfrey C, Chiao EY, et al. A randomized, placebo-controlled trial of the quadrivalent human papillomavirus vaccine in human immunodeficiency virus-infected adults aged 27 years or older: AIDS clinical trials group protocol A5298. Clinical Infectious Diseases: An Official Publication of the Infectious Diseases Society of America. 2018;67(9):1339-1346
30.Cerejeira A, Cunha S, Coelho R, Macedo G, Barkoudah E, Azevedo F, et al. Perianal warts as a risk marker for anal high-risk-human papillomavirus (HPV) detection and HPV-associated diseases. Journal of the European Academy of Dermatology and Venereology: JEADV. 2020;34(11):2613-2619
31.Albuquerque A, Stirrup O, Nathan M, Clifford GM. Burden of anal squamous cell carcinoma, squamous intraepithelial lesions and HPV16 infection in solid organ transplant recipients: A systematic review and meta-analysis. American Journal of Transplantation: Official Journal of the American Society of Transplantation and the American Society of Transplant Surgeons. 2020;20(12):3520-3528
32.Larsen HK, Hædersdal M, Thomsen LT, Hertzum-Larsen R, Lok TT, Bonde J, et al. Risk of anal high-grade squamous intraepithelial lesions among renal transplant recipients compared with immunocompetent controls. Clinical infectious Diseases: An Official publication of the Infectious Diseases Society of America. 2021;73(1):21-29
33.Tseng HF, Morgenstern H, Mack TM, Peters RK. Risk factors for anal cancer: Results of a population-based case-control study. Cancer Causes & Control: CCC. 2003;14(9):837-846
34.Daling JR, Sherman KJ, Hislop TG, Maden C, Mandelson MT, Beckmann AM, et al. Cigarette smoking and the risk of anogenital cancer. American Journal of Epidemiology. 1992;135(2):180-189
35.Celie KB, Jackson C, Agrawal S, Dodhia C, Guzman C, Kaufman T, et al. Socioeconomic and gender disparities in anal cancer diagnosis and treatment. Surgical Oncology. 2017;26(2):212-217
36.Wilbur DC, Nayar R. Bethesda 2014: Improving on a paradigm shift. Cytopathology: Official Journal of the British Society for Clinical Cytology. 2015;26(6):339-342
37.Chin-Hong PV, Berry JM, Cheng SC, Catania JA, Da Costa M, Darragh TM, et al. Comparison of patient- and clinician-collected anal cytology samples to screen for human papillomavirus-associated anal intraepithelial neoplasia in men who have sex with men. Annals of Internal Medicine. 2008;149(5):300-306
38.Dias Gonçalves Lima F, Viset JD, Leeflang MMG, Limpens J, Prins JM, de Vries HJC. The accuracy of anal swab-based tests to detect high-grade anal intraepithelial neoplasia in HIV-infected patients: A systematic review and meta-analysis. Open forum. Infectious Diseases. 2019;6(5):ofz191
39.Palefsky JM. Practising high-resolution anoscopy. Sexual Health. 2012;9(6):580-586
40.Hillman RJ, Cuming T, Darragh T, Nathan M, Berry-Lawthorn M, Goldstone S, et al. 2016 IANS international guidelines for practice standards in the detection of anal cancer precursors. Journal of Lower Genital Tract Disease. 2016;20(4):283-291
41.Burgos J, Hernández-Losa J, Landolfi S, Guelar A, Dinares M, Villar J, et al. The role of oncogenic human papillomavirus determination for diagnosis of high-grade anal intraepithelial neoplasia in HIV-infected MSM. AIDS (London, England). 2017;31(16):2227-2233
42.Chiao EY, Lensing SY, Wiley DJ, Deshmukh AA, Lee J, Darragh TM, et al. Screening strategies for the detection of anal high-grade squamous intraepithelial lesions in women living with HIV. AIDS (London, England). 2020;34(15):2249-2258
43.Nathan M, Singh N, Garrett N, Hickey N, Prevost T, Sheaff M. Performance of anal cytology in a clinical setting when measured against histology and high-resolution anoscopy findings. AIDS (London, England). 2010;24(3):373-379
44.Darragh TM, Winkler B. Anal cancer and cervical cancer screening: Key differences. Cancer Cytopathology. 2011;119(1):5-19
45.Smyczek P, Singh AE, Romanowski B. Anal intraepithelial neoplasia: Review and recommendations for screening and management. International Journal of STD & AIDS. 2013;24(11):843-851
46.Scholefield JH, Harris D, Radcliffe A. Guidelines for management of anal intraepithelial neoplasia. Colorectal Disease: The Official Journal of the Association of Coloproctology of Great Britain and Ireland. 2011;13(Suppl 1):3-10
47.Svidler López L, La Rosa L. Human papilloma virus infection and anal squamous intraepithelial lesions. Clinics in Colon and Rectal Surgery. 2019;32(5):347-357
48.Alam NN, White DA, Narang SK, Daniels IR, Smart NJ. Systematic review of guidelines for the assessment and management of high-grade anal intraepithelial neoplasia (AIN II/III). Colorectal Disease: The Official Journal of the Association of Coloproctology of Great Britain and Ireland. 2016;18(2):135-146
49.Palefsky JM, Lee JY, Jay N, Goldstone SE, Darragh TM, Dunlevy HA, et al. Treatment of anal high-grade squamous intraepithelial lesions to prevent anal cancer. The New England Journal of Medicine. 2022;386(24):2273-2282
50.Gkegkes ID, Iavazzo C, Stamatiadis AP. Intra-anal use of imiquimod: What is the clinical evidence? International Journal of STD & AIDS. 2019;30(10):1018-1024
51.Kreuter A, Hochdorfer B, Stücker M, Altmeyer P, Weiland U, Conant MA, et al. Treatment of anal intraepithelial neoplasia in patients with acquired HIV with imiquimod 5% cream. Journal of the American Academy of Dermatology. 2004;50(6):980-981
52.Steele SR, Varma MG, Melton GB, Ross HM, Rafferty JF, Buie WD. Practice parameters for anal squamous neoplasms. Diseases of the Colon and Rectum. 2012;55(7):735-749
53.Giani I, Mistrangelo M, Fucini C. The treatment of squamous anal carcinoma: Guidelines of the Italian Society of Colo-Rectal Surgery. Techniques in Coloproctology. 2013;17(2):171-179
54.Richel O, Wieland U, de Vries HJ, Brockmeyer NH, van Noesel C, Potthoff A, et al. Topical 5-fluorouracil treatment of anal intraepithelial neoplasia in human immunodeficiency virus-positive men. The British Journal of Dermatology. 2010;163(6):1301-1307
55.Megill C, Wilkin T. Topical therapies for the treatment of anal high-grade squamous intraepithelial lesions. Seminars in Colon & Rectal Surgery. 2017;28(2):86-90
56.Richel O, de Vries HJ, van Noesel CJ, Dijkgraaf MG, Prins JM. Comparison of imiquimod, topical fluorouracil, and electrocautery for the treatment of anal intraepithelial neoplasia in HIV-positive men who have sex with men: An open-label, randomised controlled trial. The Lancet Oncology. 2013;14(4):346-353
57.Chang GJ, Berry JM, Jay N, Palefsky JM, Welton ML. Surgical treatment of high-grade anal squamous intraepithelial lesions: A prospective study. Diseases of the Colon and Rectum. 2002;45(4):453-458
58.Gaisa MM, Liu Y, Deshmukh AA, Stone KL, Sigel KM. Electrocautery ablation of anal high-grade squamous intraepithelial lesions: Effectiveness and key factors associated with outcomes. Cancer. 2020;126(7):1470-1479
59.de Pokomandy A, Rouleau D, Lalonde R, Beauvais C, de Castro C, Coutlée F. Argon plasma coagulation treatment of anal high-grade squamous intraepithelial lesions in men who have sex with men living with HIV: Results of a 2-year prospective pilot study. HIV Medicine. 2018;19(2):81-89
60.Goldstone SE, Lensing SY, Stier EA, Darragh T, Lee JY, van Zante A, et al. A randomized clinical trial of infrared coagulation ablation versus active monitoring of intra-anal high-grade dysplasia in adults with human immunodeficiency virus infection: An AIDS malignancy consortium trial. Clinical Infectious Diseases: An Official Publication of the Infectious Diseases Society of America. 2019;68(7):1204-1212
61.Siegenbeek van Heukelom ML, Gosens KCM, Prins JM, de Vries HJC. Cryotherapy for intra- and perianal high-grade squamous intraepithelial lesions in HIV-positive men who have sex with men. American Journal of Clinical Dermatology. 2018;19(1):127-132
62.Goldstone RN, Hasan SR, Drury S, Darragh TM, van Zante A, Goldstone SE. A trial of radiofrequency ablation for anal intraepithelial neoplasia. International Journal of Colorectal Disease. 2017;32(3):357-365
63.Rao S, Guren MG, Khan K, Brown G, Renehan AG, Steigen SE, et al. Anal cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up(☆). Annals of Oncology: Official Journal of the European Society for Medical Oncology. 2021;32(9):1087-1100
64.Clarke MA, Wentzensen N. Strategies for screening and early detection of anal cancers: A narrative and systematic review and meta-analysis of cytology, HPV testing, and other biomarkers. Cancer Cytopathology. 2018;126(7):447-460
65.Zeng Y, Xu S, Chapman WC Jr, Li S, Alipour Z, Abdelal H, et al. Real-time colorectal cancer diagnosis using PR-OCT with deep learning. Theranostics. 2020;10(6):2587-2596
66.Sekhar H, Kochhar R, Carrington B, Kaye T, Tolan D, Saunders MP, et al. Three-dimensional (3D) magnetic resonance volume assessment and loco-regional failure in anal cancer: Early evaluation case-control study. BMC Cancer. 2020;20(1):1165
67.Mathias-Machado MC, Peixoto RD, Moniz CMV, Jácome AA. Biomarkers in anal cancer: Current status in diagnosis, disease progression and therapeutic strategies. Biomedicine. 2022;10(8):2029
68.Berry J, Glasgow SC. Vaccinations for anal squamous cancer: Current and emerging therapies. Clinics in Colon and Rectal Surgery. 2018;31(6):321-327
Written By
Isabel Garrido, João Afonso, Rosa Coelho and Guilherme Macedo
Submitted: 16 July 2023Reviewed: 23 July 2023Published: 28 September 2023