
Abstract
Ocular hypertension (OHT) is characterized by elevated intraocular pressure (IOP), without any visible optic nerve damage or visual field loss. The mean normal intraocular pressure is 15 mm Hg, and the mean intraocular pressure in patients with untreated glaucoma is 18 mm Hg. However, simply having ocular hypertension does not necessarily lead to the development of glaucoma, instead, it is deemed a considerable risk factor. An example is a person with thick corneas who may have no glaucomatous damage with an IOP of 24 mm Hg. Thus, early detection and management of OHT and corneal pachymetry are imperative to help detect higher risk patients with thinner corneas with ocular hypertension or glaucoma early. The Laroche Glaucoma calculator is an effective inexpensive method to detect patients with glaucoma, glaucoma suspects, and ocular hypertensive with a higher risk of thinner corneas and older age. With respect to the physiology of ocular hypertension, the anterior chamber angle anatomy serves a crucial role in the regulation of IOP. Gonioscopy is an important technique for examining the angle structures, which provides essential information regarding the status of the trabecular meshwork and how this can affect aqueous outflow. This chapter will further explore the anatomy and physiology of the anterior chamber angle, specific principles, techniques, and interpretation of gonioscopy, the significance of early detection as well as the management of OHT.
Keywords
- ocular hypertension
- intraocular pressure
- glaucoma development
- risk factors
- gonioscopy
1. Introduction
Ocular hypertension is a condition that is specified by an increase in intraocular pressure without any visible optic nerve damage or visual field loss [1, 2, 3, 4, 5]. The prevalence of ocular hypertension is approximately 2.7–3.8% in the general population and the incidence increases with the onset of age [6]. Ocular hypertension may not always prevail in development but it is appraised as a significant risk factor regarding the progression of glaucoma [7].
2. Anatomy and physiology of anterior chamber angle and aqueous outflow
2.1 Components of the anterior chamber angle
The anterior chamber angle is the region where the cornea, iris, and sclera meet, and subsequently the aqueous humor drains from the eye. This angle is composed of multiple structures such as the trabecular meshwork, Sclemm’s canal, iris, ciliary body, and scleral spur. Primarily the trabecular meshwork regulates the outflow of aqueous humor from the eye [8]. Specifically, the Schlemm’s canal is characterized as the principal pathway for aqueous humor. The ciliary body produces aqueous humor and the iris controls the size of the pupil; as the iris regulates the amount of light entering the eye. While the scleral spur is a bony ridge that anchors the ciliary body and trabecular meshwork [8].
2.2 Role of the trabecular meshwork in aqueous humor outflow
The trabecular meshwork (TM) (Figure 1) is the most essential part of the anterior chamber angle as it regulates aqueous humor outflow. It is a specialized tissue located at the anterior portion of the angle that is responsible for the majority of the resistance to aqueous humor outflow. The TM contains a meshwork of collagen fibers and endothelial cells that function to filter the aqueous humor before it flows into Schlemm’s canal [8, 9]. Essentially, Schlemm’s canal is a circular canal located around the circumference of the cornea that behaves as a collector channel for the aqueous humor to drain into the episcleral venous system [9].
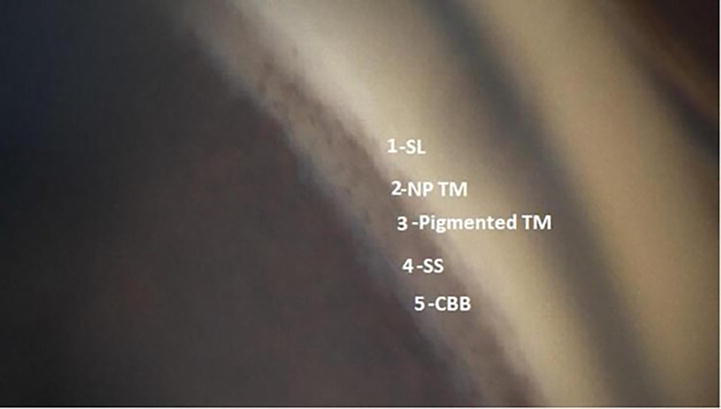
Figure 1.
Normal trabecular meshwork, 1-Schwalbe’s Line, 1-Nonpigmented Trabecular Meshwork, 3-Pigmented Trabecular Meshwork, 4-Scleral spur, 5- Ciliary Body Band (Nidek GS1 Gonioscope).
The aqueous humor is generated by the ciliary body and flows through the posterior chamber into the anterior chamber, where it circulates and nourishes the cornea as well as the lens [8]. The aqueous humor must perpetually flow out of the eye to maintain a stable IOP. The TM is imperative in regulating the outflow of aqueous humor. Aqueous humor outflow happens through the mechanism of two different pathways; the trabecular meshwork pathway and the uveoscleral pathway [10]. Essentially, the trabecular meshwork pathway is responsible for approximately 75% of aqueous humor outflow and is mostly regulated by the TM [11].
2.3 Factors that affect angle structures and obstruction of aqueous outflow
The regulation of intraocular eye pressure is an intricate process that involves the production and drainage of aqueous humor. The trabecular meshwork plays a vital role in the outflow of aqueous humor, and any obstruction or dysfunction of this structure can lead to an increase in IOP. A multitude of factors can affect the angle structures and outflow, including age, genetics, increased lens thickness, inflammation, trauma, medications, and systemic diseases [2]. The most common cause of outflow obstruction is the increased thickness of the lens in the eye. This compresses Schlemm’s canal. The enlarged lens also leads to narrowing of the angle and increased iridozonular-iris rubbing, pigment liberation, and pigment obstruction of the trabecular meshwork (Figure 2) [12]. Cataract surgery expands the Schlemm’s canal and is associated with the lowering of intraocular pressure [13]. Microinvasive glaucoma surgery bypasses the obstructed trabecular meshwork further lowering intraocular pressure [14].
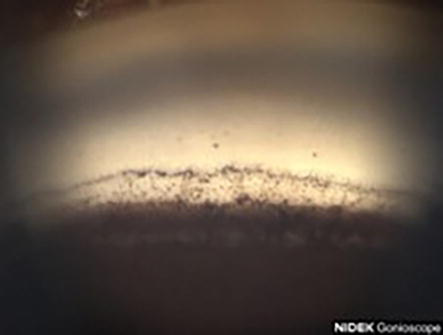
Figure 2.
Heavy pigmentation of inferior angle on (Nidek GS1 Gonioscope).
3. Gonioscopy: technique and interpretation
3.1 Principles and technique of gonioscopy
Primarily, gonioscopy is a technique for examining the angle structure using a specialized lens. The procedure involves placing the gonioscope lens on the cornea to visualize the angle structures. The technique of gonioscopy involves an array of steps, first, there is patient preparation which is done before performing the gonioscopy, to adequately explain the procedure to the patient and to receive informed consent [15]. Furthermore, the eye is numbed with topical anesthetic drops to minimize any discomfort during the examination. Subsequently, the gonioscope lens is decided upon as there are multiple lenses available including Goldmann, Sussman, and Zeiss Lenses. This is selected based on the patient’s anatomy, the examiner’s preference as well as the level of detail required [16].
Then a coupling agent, typically a viscous gel or fluid is applied to the cornea to guarantee an appropriate amount of contact between the gonioscope lens and the corneal surface. As this enables optimal visualization of the anterior chamber angle structures of the eye. Furthermore, a gonioscope lens is placed accordingly, specifically on the cornea, securing that the entirety of the anterior chamber angle is visible through the lens. Throughout this process, the examiner may adjust as he or she sees fit [17].
This allows viewing of the angle by overcoming the total internal reflection at the cornea-air interface. A four-mirror lens is best to be able to perform indentation gonioscopy to see if there is an appositional vs. synechial closure of the angle. Indentation gonioscopy cannot be performed with a three-mirror gonioscope lens. The angle is graded according to the amount of visible trabecular meshwork and the extent of the angle opening. The grading system ranges from 0 to 4, with 0 indicating a closed angle and 4 which is characterized by a wide-open angle. The trabecular meshwork, Schlemm’s canal, iris processes, and angle recesses are further evaluated. Assessment of these structures provides information regarding the angle width, presence of peripheral anterior synechiae, neovascularization as well as any pathological changes [18].
3.2 Interpretation of gonioscopic findings
Gonioscopy supplies beneficial information regarding the status of the trabecular meshwork and the degree of obstruction or dysfunction. The findings can help in the diagnosis and management of OHT and glaucoma. Anyone with an IOP of 18 mm Hg or higher should have a gonioscopy performed. For example, a narrow or closed angle can indicate a higher risk for angle-closure glaucoma, which requires prompt treatment to prevent vision loss. Heavier pigmentation in the inferior angle compared to the superior angle can be a sign of pigment liberation from lens iris rubbing contributing to elevated eye pressure [19].
3.3 Common pitfalls and challenges in gonioscopy
Ultimately, gonioscopy is a technique that requires expertise, however, some quite several pitfalls and challenges impact the accuracy as well as the reliability of the examination. This ranges from characteristics such as patient factors, technician factors, variability in angle structures, and the learning curve regarding the examiner. In regard to patient factors, many patients encounter challenges maintaining steady fixation throughout the procedure, thus leading to suboptimal visualization. Furthermore, small palpebral fissures, deep-set eyes, or substantial cornea edema can decrease the probability of attaining proper contact between the goniscope lens and the cornea [20].
Additionally, the physician’s incorrectly applying the coupling agent or improperly positioning the gonioscope lens diminished the quality of the gonioscopic view. Hence the physician’s proficiency in the technique plays a vital role in obtaining reliable and accurate results. Moreover, the variances in angle structures can primarily be attributed to age, race, and pathological conditions. Thus, acknowledging these variations and differentiating them from pathological changes proves to be difficult [18]. Lastly, examiners typically experience a learning curve concerning the gonioscopy findings, hence properly grading the angle necessitates experience as well as familiarity with different angle configurations [21].
4. Importance of gonioscopy and angle assessment in ocular hypertension
4.1 Role of gonioscopy in diagnosis and monitoring of ocular hypertension
Gonioscopy is pivotal in regarding the diagnosis and monitoring of ocular hypertension. Gonioscopic photos can be taken to educate patients about the findings of narrowing of the angle or increased pigmentation that may need to be addressed with an intervention. Medical therapy is often started to lower intraocular pressure. Currently, earlier cataract surgery and micro-invasive glaucoma surgery can lower intraocular pressure and reduce medication burden. Subsequently, cataract surgery has been noted to decrease the prevalence of angle closure [22].
4.2 Importance of angle assessment in predicting risk of glaucoma
Primarily, angle assessment through gonioscopy is necessary for predicting the risk of developing glaucoma in individuals with ocular hypertension. Previous research studies have indicated that narrow-angle or angle-closure configurations are associated with a higher risk of glaucoma development [23]. Patients with narrow angles require close monitoring and may be candidates for preventive treatment, such as laser peripheral iridotomy to prevent angle closure and consequent glaucomatous damage. Recently cataract surgery has been shown to be more effective than laser iridotomy in angle closure patients and this should be offered earlier to patients [24].
4.3 Relationship between angle status and response to treatment
The angle status of the patient has repercussions for the response to glaucoma treatment for patients with ocular hypertension. Studies in the past have demonstrated that angle status can influence the effectiveness of certain treatment modalities, such as medications or surgical interventions [25]. For example, for patients with open-angle configurations, medical therapy with topical glaucoma medications targeting the trabecular meshwork or uveoscleral outflow pathways prove to be more effective in diminishing intraocular pressure. These patients are also eligible for selective laser trabeculoplasty. Contrastingly, patients with synechial angle closure are not eligible for laser trabeculoplasty and may be less responsive to topical medications. They may need goniosynechialysis or trabeculectomy to migitigate angle obstruction and acquire sufficient intraocular pressure control [26].
5. Risk factors affecting angle structures and outflow
5.1 Age, race, and gender
Primarily, a multitude of risk factors can affect the angle structures and outflow in the eye. Age is an essential determinator as the anatomical and physiological changes that transpire with aging can implicate the angle. As individuals increase with age, the trabecular meshwork becomes reduced efficiency in draining the aqueous humor, provoking an increased risk for ocular hypertension and glaucoma. The size of the trabecular meshwork also decreases with age [27].
Race is another risk factor that has a profound impact, as several studies have demonstrated that specific racial groups, particularly those of African descent have a higher prevalence of narrow angles and angle-closure glaucoma. In comparison to patients of European descent which have an elevated risk of open-angle glaucoma. These differences demonstrated between patients of different races emphasize the influence that race has on predicting the risk of glaucoma. Black patients in the United States, Caribbean, and Africa have decreased access to healthcare and often present with more advanced glaucoma [28]. Additionally, individuals with more melinated skin also have brown irises with higher pigment density. In patients with glaucoma there is greater depigmentation of posterior pigment epithelium of the iris that can lead to obstruction of the trabecular meshwork [29]. This can be picked up on gonioscopy.
Furthermore, sex plays a crucial role in the angle structures and outflow. Previous studies indicated that hormonal differences between male and female individuals contribute to variations in the risk of developing glaucoma, however, the exact pathophysiology is not fully understood [30]. For example, many women are put at a higher risk of developing primary angle-closure glaucoma after menopause due to significant hormonal changes [30].
5.2 Systemic and ocular conditions
Specific systemic and ocular conditions can impact the angle structures and outflow, thereby enhancing the possibility of ocular hypertension and glaucoma. For example, systemic conditions such as diabetes and hypertension can affect the blood vessel in the eye, including those in the angle [31]. As well as conditions that cause inflammation, for instance, uveitis or pseudoexfoliation syndrome. These conditions can impair the angle and subsequently compromise the aqueous humor outflow [32]. Additionally, ocular conditions such as high myopia and patients that have had previous eye surgeries, particularly cataract surgery. Moreover, in regards to high myopia, the elongated shape of the eyeball can potentially cause mechanical changes in the angle, consequently resulting in increased resistance to aqueous outflow [33]. Other ophthalmic surgical procedures, mostly those involving the lens can alter the anatomical configuration of the anterior chamber and affect the angle [34].
5.3 Medications and lifestyle factors
Multiple medications can have a substantial effect on the angle structures and outflow dynamics. For example, medications that dilate the pupil can further narrow the angle and increase the risk of angle-closure glaucoma in susceptible individuals [35]. This is comparable to other systemic medications such as topiramate, which are used for migraines or epilepsy and have been associated with angle-closure glaucoma [36].
Furthermore lifestyle factors, particularly, smoking and excessive alcohol consumption can contribute to changes in the angle structures and outflow. Particularly, smoking has been associated with increased lens thickness, cataracts intraocular pressure, and a higher incidence of developing glaucoma [37]. Alcohol consumption, mostly heavy drinking can comprise the blood flow to the optic nerve and negatively impact the drainage of aqueous humor [38]. However, these factors are characterized as potential risk factors for angle structures and outflow but individual susceptibility can vary.
6. Clinical management of ocular hypertension
6.1 Importance of regular monitoring and risk stratification
Close observation and assessment of ocular hypertension are essential for promptly identifying the etiology and potential interventions to prevent vision impairments. The Laroche glaucoma calculator helps to identify patients who may be at increased risk based not only on IOP but also age and central corneal thickness [4]. Thus, the clinical management of ocular hypertension upholds the beliefs of preventative medicine and involves regular monitoring and risk stratification to ascertain patients with an elevated risk of developing glaucoma [39]. This typically includes periodic comprehensive eye examinations, measurement of intraocular pressure, assessment of the optic nerve, and evaluation of visual fields. Subsequently, risk stratification aids in recognizing individuals at a higher risk and prioritizing the management and follow-up of those patients [39].
6.2 Treatment options and goals
The main objective in managing ocular hypertension is to prevent or delay the onset of glaucoma and the associated vision loss. Treatment decisions are dependent on the level of intraocular pressure, risk factor, and the presence of structural or functional changes that are diagnostic of glaucoma. Early cataract surgery and lower intraocular pressure and reduce the need for medications [40]. In patients who have developed mild to moderate glaucoma, early cataract surgery and microinvasive glaucoma surgery can lower intraocular pressure and reduce medication burden (Figure 3) [41]. Other treatment options include topical therapy and laser procedures, for example, selective laser trabeculoplasty of surgical interventions such as glaucoma filtering surgery.
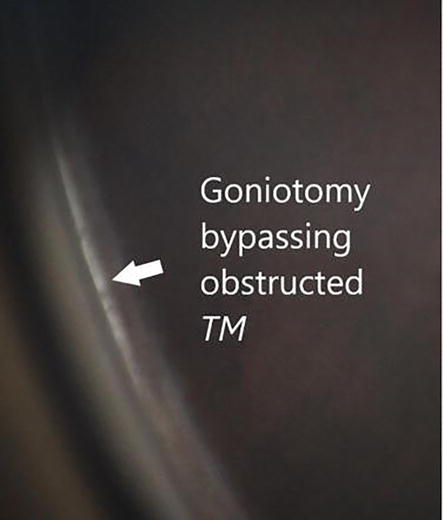
Figure 3.
Goniotomy performed at the time of cataract surgery with Sinskey hook bypassing obstructed trabecular meshwork at the time of cataract surgery.
However, the main objective of treatment is to reduce intraocular pressure to a level that diminishes the risk of glaucoma progression. The target intraocular pressure is specific to the patient as it is dependent on individual risk factors such as the extent of optic nerve damage, the patient’s baseline intraocular pressure, and the other risk factors [39]. Clinicians approach lowering the intraocular pressure by decreasing aqueous humor production or increasing its outflow. Ultimately, the treatment plan is individualized to the patient considering medication compliance and potential adverse complications.
6.3 Role of gonioscopy in treatment decision making
Gionoscopy proves to be an essential contribution to the treatment plan in patients with ocular hypertension. As it aids in the assessment of the angle structures and provides beneficial insights regarding the status of the trabecular meshwork and the presence of angle abnormalities or pathology. In addition, it assists the clinician in determining a prognosis. For example, if gonioscopy discloses a narrow or closed angle it may suggest a higher risk of angle-closure glaucoma, which requires immediate intervention to prevent permanent vision loss. Heavy pigment in the angle due to pigment liberation from the thickened lens rubbing against the posterior iris may have one consider earlier cataract surgery and micro-invasive glaucoma surgery [41]. Furthermore, gonioscopy helps to identify specific angle abnormalities such as peripheral anterior synechiae or neovascularization which may have implications for treatment planning. The presence of neovascularization of the angle may require pan-retinal laser, anti-VEGF treatment and a glaucoma tube shunt [42].
Thereby, by providing detailed information about the angle structures, gonioscopy aids in individualizing treatment strategies and monitoring the response to treatment [43]. Clinicians can target specific angle abnormalities and optimize the management of ocular hypertension.
In summary, gonioscopy is pivotal in this process by providing valuable information about the angle structures and influencing treatment choices [43]. Thus by incorporating gonioscopy findings into the management plan, clinicians can optimize the care for patients and reduce the risk of glaucoma progression.
7. Future directions and challenges
7.1 Emerging technologies in angle assessment and imaging
The field of angle assessment is continuously evolving, undergoing advancements in imaging and the new emergence of technologies offers fruitful advancements in the diagnosis and management of ocular conditions [44]. The main objective of these new advancements in technology provide more detailed and comprehensive information concerning the anterior chamber angle, resulting in improved accuracy and precision in the evaluation of angle structures and outflow [45].
Moreover, the emerging technologies in angle assessment such as anterior segment optical coherence tomography provide the opportunity for high-resolution imaging of the anterior segment, which supplies detailed cross-sectional images of the angle structures [45]. This non-invasive imaging technique has the capacity to strengthen the evaluation of the trabecular meshwork, iris configuration, and angle dimensions, contributing beneficial observations for diagnosis and treatment planning [45].
An alternative sphere of advancement is the expansion of novel imaging modalities, including swept-source OCT and ultrasound biomicroscopy [46]. These techniques permit clinicians to visualize and analyze angle structures with improved depth penetration and resolution, facilitating complete analysis of the anterior chamber angle [45].
7.2 Addressing disparities in access to care and screening
Although advancements in technology demonstrate prospects for enhancing angle assessment, thus it is imperative to address disparities in access to care and screening [47]. Disparities in healthcare access, mostly amongst underserved populations, can postpone diagnosis and cause improper ocular conditions which include ocular hypertension and glaucoma [48, 49]. Thereby, community outreach programs, education campaigns, and collaborations between healthcare providers and community organizations aid in improving access to care and promoting early detection and intervention [50]. It is important for the industry to invest in media that often has a greater reach to higher-risk populations, more specifically Black patients as they disportiontely experience decreased access to care. It is also important to train more Black ophthalmologists and optometrists globally to meet the needs of Black communities around the world [51].
Remote screening programs, teleophthalmology, and digital health platforms can promote the early identification of patients at risk, granting time-efficient referrals for additional assessment and supervision [52]. Through the implementation of remote monitoring clinicians can monitor a patients intraocular pressure levels which allows for early detection of increases that can predispose patients to the onset of glaucoma [52].
7.3 Research priorities
Furthermore, determining research priorities is vital to propel advancements in the fields of gonioscopy and angle assessment. Numerous research priorities need to be addressed which include validation and standardization of grading systems, longitudinal studies, predictive models, cost-effectiveness analysis, patient-centered outcomes and quality-of-life measures [53]. Essentially, there is a demand for standardized and validated grading systems for evaluating the angle structures through gonioscopy. Consensus on terminology, definitions, and grading criteria will improve the consistency and conformity of findings across different studies [54]. Additionally, long-term studies are necessary to deepen comprehension between angle status, progression of ocular hypertension, and the development of glaucoma. Predictive models that incorporate multiple elements contributing to the risk factors can help identify individuals who are the most likely to benefit from early intervention [55].
Furthermore, assessing the cost-effectiveness of different screening and management strategies is essential for resource allocation and decision-making [56]. Examining the economic impact of implementing new technologies and interventions can help navigate healthcare policies and ensure the efficient allocation of healthcare resources [57]. Research should propel investigations regarding the development of patient-centered interventions and support systems. By confronting these research priorities, the field can make significant strides in optimizing the accuracy and effectiveness of angle assessment, mitigating differences in access to care, and improving patient outcomes in ocular hypertension and glaucoma management.
8. Conclusion
In conclusion, gonioscopy and angle assessment are imperative in managing ocular hypertension, a substantial risk factor for glaucoma and vision loss. Thus, comprehending the anterior chamber angle anatomy and physiology provides insights into outflow mechanisms and factors implicating angle structures. Gonioscopy provides visualizing and grading of the angle, assisting in diagnosis, monitoring, and treatment decisions. Risk factors including age, race, gender, and systemic conditions influence angle structures. Thus, consistent surveillance and treatment prioritize focusing on reducing intraocular pressure and preserving optic nerve health. Developing technologies and addressing disparities in care improve evaluation and access.
In summary, gonioscopy and angle assessment are imperative concerning ocular hypertension management. Gonioscopy assists with identifying the diagnosis and monitoring of ocular hypertension. This contributes sufficient information for the risk prediction of glaucoma and impacts treatment decisions [43]. With the incorporation of gonioscopy into the assessment of patients with ocular hypertension clinicians can obtain vital insights into the angling status, which permits appropriate risk stratification and personalized treatment approaches [15].
Conflict of interest statement
Dr. Laroche is a speaker for Sight Science, Johnson and Johnson, Nidek, and receives research support from Alcon. The information presented in this chapter is based on scientific evidence, medical knowledge, and professional experience without any financial or personal relationships that could potentially bias the content or influence the interpretation of the information provided. The main goal is to supply accurate, reliable, and unbiased information for the benefit of readers and the advancement of medical knowledge in the field of ocular hypertension and angle assessment.
References
- 1.
Tielsch JM, Katz J, Singh K, Quigley HA, Gottsch JD, Javitt J, et al. A population-based evaluation of glaucoma screening: The Baltimore eye survey. American Journal of Epidemiology. 1991; 134 (10):1102-1110. DOI: 10.1093/oxfordjournals.aje.a116013 - 2.
Kass MA, Hart WM Jr, Gordon M, Miller JP. Risk factors favoring the development of glaucomatous visual field loss in ocular hypertension. Survey of Ophthalmology. 1980; 25 (3):155-162. DOI: 10.1016/0039-6257(80)90092-2 - 3.
Abah ER, Mahmud-Ajeigbe AF, Sharief S, Chinda D, Jiya PY, Bob-Egbe O. Central corneal thickness and intraocular pressure of adult Nigerians: An assessment of Zaria community. West African Journal of Medicine. 2018; 35 (3):158-161 - 4.
Laroche D, Rickford K, Mike EV, Hunter L, Ede E, Ng C, et al. A novel, low-cost glaucoma calculator to identify glaucoma patients and stratify management. Journal of Ophthalmology. 2022; 2022 :5288726. DOI: 10.1155/2022/5288726 - 5.
Lei XW, Wei P, Li XL, Yang K, Lei JZ. Changes of structures of anterior chamber angle in rabbit chronic high intraocular pressure model. Zhonghua Yan Ke Za Zhi. 2009; 45 (10):892-897 Chinese - 6.
Saboo US, Amparo F, Shikari H, Dana R. Prevalence of ocular hypertension and glaucoma in patients with chronic ocular graft-versus-host disease. Graefe's Archive for Clinical and Experimental Ophthalmology. 2016; 254 (5):923-928. DOI: 10.1007/s00417-016-3312-3. Epub 2016 Mar 12 - 7.
Nislawati R, Taufik Fadillah Zainal A, Ismail A, Waspodo N, Kasim F, Gunawan AMAK. Role of hypertension as a risk factor for open-angle glaucoma: A systematic review and meta-analysis. BMJ Open Ophthalmology. 2021; 6 (1):e000798. DOI: 10.1136/bmjophth-2021-000798 - 8.
Hann CR, Bentley MD, Vercnocke A, Ritman EL, Fautsch MP. Imaging the aqueous humor outflow pathway in human eyes by three-dimensional micro-computed tomography (3D micro-CT). Experimental Eye Research. 2011; 92 (2):104-111. DOI: 10.1016/j.exer.2010.12.010. Epub 2010 Dec 25 - 9.
Avtar R, Srivastava R. Modelling aqueous humor outflow through trabecular meshwork. Applied Mathematics and Computation. 2007; 189 (1):734-745. DOI: 10.1016/j.amc.2006.11.109 - 10.
Tamm ER, Braunger BM, Fuchshofer R. Intraocular pressure and the mechanisms involved in resistance of the aqueous humor flow in the trabecular meshwork outflow pathways. Progress in Molecular Biology and Translational Science. 2015; 134 :301-314. DOI: 10.1016/bs.pmbts.2015.06.007. Epub 2015 Jul 9 - 11.
Goel M, Picciani RG, Lee RK, Bhattacharya SK. Aqueous humor dynamics: A review. Open Ophthalmology Journal. 2010; 4 :52-59. DOI: 10.2174/1874364101004010052 - 12.
Laroche D, Capellan P. The Aging Lens and Glaucoma in persons over 50: Why early cataract surgery/refractive lensectomy and microinvasive trabecular bypass can prevent blindness and cure elevated eye pressure. Journal of the National Medical Association. Aug 2021; 113 (4):471-473. DOI: 10.1016/j.jnma.2021.03.001. Epub 2021 Mar 27. PMID: 33781565 - 13.
Stamer WD, Braakman ST, Zhou EH, Ethier CR, Fredberg JJ, Overby DR, et al. Biomechanics of Schlemm's canal endothelium and intraocular pressure reduction. Progress in Retinal and Eye Research. 2015; 44 :86-98. DOI: 10.1016/j.preteyeres.2014.08.002. Epub 2014 Sep 16 - 14.
Saheb H, Ahmed II. Micro-invasive glaucoma surgery: Current perspectives and future directions. Current Opinion in Ophthalmology. 2012; 23 (2):96-104. DOI: 10.1097/ICU.0b013e32834ff1e7 - 15.
Narayanaswamy A, Vijaya L, Shantha B, Baskaran M, Sathidevi AV, Baluswamy S. Anterior chamber angle assessment using gonioscopy and ultrasound biomicroscopy. Japanese Journal of Ophthalmology. 2004; 48 (1):44-49. DOI: 10.1007/s10384-003-0004-4 - 16.
Barbero S. The Alvarez and Lohmann refractive lenses revisited. Optics Express. 2009; 17 (11):9376-9390. DOI: 10.1364/oe.17.009376 - 17.
Esporcatte BL, Vessani RM, Melo LA Jr, Yanagimori NS, Bufarah GH, Allemann N, et al. Diagnostic performance of optical coherence tomography and nonspecialist gonioscopy to detect angle closure. Journal of Current Glaucoma Practice. 2022; 16 (1):53-58. DOI: 10.5005/jp-journals-10078-1354 - 18.
Sadagopan KA, Periasamy P. A new lens-holder to facilitate slit-lamp bio-microscopic-aided fundus and gonioscopic examination. Oman Journal of Ophthalmology. 2021; 14 (2):115-116. DOI: 10.4103/ojo.ojo_383_20 - 19.
Laroche D, Rickford K, Sinon J, Brown A, Ng C, Sakkari S. Preventing blindness from glaucoma with patient education, the NIDEK GS-1 gonioscope, lensectomy and microinvasive glaucoma surgery. Journal of the National Medical Association. 2023; 115 (2):175-185. DOI: 10.1016/j.jnma.2023.01.014. Epub 2023 Feb 24 - 20.
Varadaraj V, Sengupta S, Palaniswamy K, Srinivasan K, Kader MA, Raman G, et al. Evaluation of angle closure as a risk factor for reduced corneal endothelial cell density. Journal of Glaucoma. 2017; 26 (6):566-570. DOI: 10.1097/IJG.0000000000000669 - 21.
Phu J, Wang H, Khuu SK, Zangerl B, Hennessy MP, Masselos K, et al. Anterior chamber angle evaluation using gonioscopy: Consistency and agreement between optometrists and ophthalmologists. Optometry and Vision Science. 2019; 96 (10):751-760. DOI: 10.1097/OPX.0000000000001432 - 22.
Hu CC, Lin HC, Chen CS, Kuo NW. Reduction in admissions of patients with acute primary angle closure occurring in conjunction with a rise in cataract surgery in Taiwan. Acta Ophthalmologica. 2008; 86 (4):440-445. DOI: 10.1111/j.1600-0420.2007.01066.x. Epub 2007 Nov 17 - 23.
Weinreb RN, Aung T, Medeiros FA. The pathophysiology and treatment of glaucoma: A review. Journal of the American Medical Association. 2014; 311 (18):1901-1911. DOI: 10.1001/jama.2014.3192 - 24.
Azuara-Blanco A, Burr J, Ramsay C, Cooper D, Foster PJ, Friedman DS, et al. Effectiveness of early lens extraction for the treatment of primary angle-closure glaucoma (EAGLE): A randomised controlled trial. Lancet. 2016; 388 (10052):1389-1397. DOI: 10.1016/S0140-6736(16)30956-4 - 25.
Burr J, Azuara-Blanco A, Avenell A, Tuulonen A. Medical versus surgical interventions for open angle glaucoma. Cochrane Database of Systematic Reviews. 2012;(9):CD004399. DOI: 10.1002/14651858.CD004399.pub3 - 26.
Harasymowycz PJ, Papamatheakis DG, Ahmed I, Assalian A, Lesk M, Al-Zafiri Y, et al. Phacoemulsification and goniosynechialysis in the management of unresponsive primary angle closure. Journal of Glaucoma. 2005; 14 (3):186-189. DOI: 10.1097/01.ijg.0000159131.38828.85 - 27.
Chen Z, Sun J, Li M, Liu S, Chen L, Jing S, et al. Effect of age on the morphologies of the human Schlemm's canal and trabecular meshwork measured with swept-source optical coherence tomography. Eye (London, England). 2018; 32 (10):1621-1628. DOI: 10.1038/s41433-018-0148-6. Epub 2018 Jun 19 - 28.
Olawoye O, Kizor-Akaraiwe N, Pons J, Sarimiye T, Washaya J, Hughes S, et al. Clinical characteristics and stage at presentation of glaucoma patients in Sub-Saharan Africa. Journal of Glaucoma. 2022; 31 (9):717-723. DOI: 10.1097/IJG.0000000000002068. Epub 2022 Jun 27 - 29.
Bashkatov A, Genina E, Koblova E, Tuchin V. Estimation of melanin content in iris of human eye. Saratov Journal of Medical Scientific Research. 2008; 5688 :302-311. DOI: 10.1117/12.593651 - 30.
Tehrani S. Gender difference in the pathophysiology and treatment of glaucoma. Current Eye Research. 2015; 40 (2):191-200. DOI: 10.3109/02713683.2014.968935. Epub 2014 Oct 6 - 31.
Shoshani Y, Harris A, Shoja MM, Arieli Y, Ehrlich R, Primus S, et al. Impaired ocular blood flow regulation in patients with open-angle glaucoma and diabetes. Clinical & Experimental Ophthalmology. 2012; 40 (7):697-705. DOI: 10.1111/j.1442-9071.2012.02778 - 32.
Yanagi M, Kawasaki R, Wang JJ, Wong TY, Crowston J, Kiuchi Y. Vascular risk factors in glaucoma: A review. Clinical & Experimental Ophthalmology. 2011; 39 (3):252-258. DOI: 10.1111/j.1442-9071.2010.02455 - 33.
Bontzos G, Plainis S, Papadaki E, Giannakopoulou T, Detorakis E. Mechanical optic neuropathy in high myopia. Clinical and Experimental Optometry. 2018; 101 (4):613-615. DOI: 10.1111/cxo.12548 - 34.
Yamaguchi T, Negishi K, Yuki K, Saiki M, Nishimura R, Kawaguchi N, et al. Alterations in the anterior chamber angle after implantation of iris-fixated phakic intraocular lenses. Journal of Cataract & Refractive Surgery. 2008; 34 (8):1300-1305. DOI: 10.1016/j.jcrs.2008.04.033 - 35.
Lachkar Y, Bouassida W. Drug-induced acute angle closure glaucoma. Current Opinion in Ophthalmology. 2007; 18 (2):129-133. DOI: 10.1097/ICU.0b013e32808738d5 - 36.
Quagliato LB, Barella K, Abreu Neto JM, Quagliato EMAB. Topiramate-associated acute, bilateral, angle-closure glaucoma: Case report. Arquivos Brasileiros de Oftalmologia. 2013; 76 (1):48-49. DOI: 10.1590/S0004-27492013000100014 - 37.
Wang D, Huang Y, Huang C, et al. Association analysis of cigarette smoking with onset of primary open-angle glaucoma and glaucoma-related biometric parameters. BMC Ophthalmology. 2012; 12 :59. DOI: 10.1186/1471-2415-12-59 - 38.
Braunger BM, Fuchshofer R, Tamm ER. The aqueous humor outflow pathways in glaucoma: A unifying concept of disease mechanisms and causative treatment. European Journal of Pharmaceutics and Biopharmaceutics. 2015; 95 :173-181. DOI: 10.1016/j.ejpb.2015.04.029 - 39.
Maier PC, Funk J, Schwarzer G, Antes G, Falck-Ytter YT. Treatment of ocular hypertension and open angle glaucoma: Meta-analysis of randomised controlled trials. BMJ. 2005; 331 (7509):134. DOI: 10.1136/bmj.38506.594977.E0. Epub 2005 Jul 1 - 40.
Mansberger SL, Gardiner SK, Gordon M, Kass M, Ramulu P, Ocular Hypertension Treatment Study Group. Cataract surgery lowers intraocular pressure and medication use in the medication group of the ocular hypertension treatment study. American Journal of Ophthalmology. 2022; 236 :53-62. DOI: 10.1016/j.ajo.2021.07.008. Epub 2021 Jul 17 - 41.
Laroche D, Oseni J, Nkrumah G, Ng C. Clear lensectomy with Hydrus stent in black and afro-Latino patients: A 1-year retrospective study. Journal of Ophthalmology. 2022; 2022 :8011745. DOI: 10.1155/2022/8011745 - 42.
Senthil S, Dada T, Das T, Kaushik S, Puthuran GV, Philip R, et al. Neovascular glaucoma—A review. Indian Journal of Ophthalmology. 2021; 69 (3):525-534. DOI: 10.4103/ijo.IJO_1591_20 - 43.
Baskaran M, Perera SA, Nongpiur ME, Tun TA, Park J, Kumar RS, et al. Angle assessment by EyeCam, goniophotography, and gonioscopy. Journal of Glaucoma. 2012; 21 (7):493-497. DOI: 10.1097/IJG.0b013e3182183362 - 44.
Weinreb RN, Moghimi S. Advances in ocular imaging. Asia-Pacific Journal of Ophthalmology. 2019; 8 (2):97-98. DOI: 10.22608/APO.201984 - 45.
Shinoj VK, Hong XJ, Murukeshan VM, Baskaran M, Tin A. Progress in anterior chamber angle imaging for glaucoma risk prediction - A review on clinical equipment, practice and research. Medical Engineering & Physics. 2016; 38 (12):1383-1391. DOI: 10.1016/j.medengphy.2016.09.014. Epub 2016 Oct 24 - 46.
Mao Y, Flueraru C, Chang S, Popescu DP, Sowa MG. Imaging of biomedical turbid tissue using catheter swept-source optical coherence tomography. In: 2010 IEEE International Workshop on Medical Measurements and Applications, Ottawa, ON, Canada. 2010. pp. 151-157. DOI: 10.1109/MEMEA.2010.5480212. Available from: https:// ieeexplore.ieee.org/document/5480212 - 47.
Piyasena MMPN, Murthy GVS, Yip JLY, Gilbert C, Zuurmond M, Peto T, et al. Systematic review on barriers and enablers for access to diabetic retinopathy screening services in different income settings. PLoS One. 2019; 14 (4):e0198979. DOI: 10.1371/journal.pone.0198979 - 48.
Wu AM, Shen LQ. Racial disparities affecting black patients in glaucoma diagnosis and management. Seminars in Ophthalmology. 2023; 38 (1):65-75. DOI: 10.1080/08820538.2022.2152702. Epub 2022 Dec 1 - 49.
Altangerel U, Nallamshetty HS, Uhler T, Fontanarosa J, Steinmann WC, Almodin JM, et al. Knowledge about glaucoma and barriers to follow-up care in a community glaucoma screening program. Canadian Journal of Ophthalmology. 2009; 44 (1):66-69. DOI: 10.3129/i08-175 - 50.
Meade CD, Menard J, Martinez D, Calvo A. Impacting health disparities through community outreach: Utilizing the CLEAN look (culture, literacy, education, assessment, and networking). Cancer Control. 2007; 14 (1):70-77. DOI: 10.1177/107327480701400110 - 51.
Nelson R. Telemedicine and telehealth: The potential to improve rural access to care. AJN, American Journal of Nursing. 2017; 117 (6):17-18. DOI: 10.1097/01.NAJ.0000520244.60138.1c - 52.
Nangalia V, Prytherch DR, Smith GB. Health technology assessment review: Remote monitoring of vital signs--current status and future challenges. Critical Care. 2010; 14 (5):233. DOI: 10.1186/cc9208. Epub 2010 Sep 24 - 53.
Dy SM, Herr K, Bernacki RE, Kamal AH, Walling AM, Ersek M, et al. Methodological research priorities in palliative care and hospice quality measurement. Journal of Pain and Symptom Management. 2016; 51 (2):155-162. DOI: 10.1016/j.jpainsymman.2015.10.019. Epub 2015 Nov 17 - 54.
Desmond T, Tran V, Maharaj M, Carnt N, White A. Diagnostic accuracy of AS-OCT vs gonioscopy for detecting angle closure: A systematic review and meta-analysis. Graefe's Archive for Clinical and Experimental Ophthalmology. 2022; 260 (1):1-23. DOI: 10.1007/s00417-021-05271-4. Epub 2021 Jul 5. Erratum in: Graefe's Archive for Clinical and Experimental Ophthalmology. 2021 Sep 28 - 55.
Thompson SG, Higgins JP. Treating individuals 4: Can meta-analysis help target interventions at individuals most likely to benefit? Lancet. 2005; 365 (9456):341-346. DOI: 10.1016/S0140-6736(05)17790-3 - 56.
Guindo LA, Wagner M, Baltussen R, Rindress D, van Til J, Kind P, et al. From efficacy to equity: Literature review of decision criteria for resource allocation and healthcare decisionmaking. Cost Effectiveness and Resource Allocation. 2012; 10 (1):9. DOI: 10.1186/1478-7547-10-9 - 57.
Hoomans T, Severens JL. Economic evaluation of implementation strategies in health care. Implementation Science. 2014; 9 :168. DOI: 10.1186/s13012-014-0168-y