
Abstract
The authors analyze basic bioethical issues, with application in neurorehabilitation clinical practice. We consider traditions of Bulgarian schools of Physical and Rehabilitation Medicine, Physiotherapy and Ergotherapy, related to bioethics. Physical and rehabilitation medicine investigates the effects of the application of natural and preformed physical modalities on the human organism. Neurorehabilitation is an interdisciplinary field - between neurology, neurosurgery and physical medicine. Many principles of the Declaration on bioethics and patients’ rights are obligatory in the rehabilitation practice, e.g.: human dignity and human rights, autonomy, consent, equality and equity, non-discrimination and non-stigmatization (for patients with disabilities). Several bioethical topics are important for neurorehabilitation: human research, neuro-ethics, pain management, assisted suicide, euthanasia. We present an analysis of bioethical problems of a clinical case from our neurorehabilitation practice.
Keywords
- bioethics
- rehabilitation
- neurorehabilitation
- patient’s rights
- informed consent
- education
1. Introduction
Physical and rehabilitation medicine investigates the effects of the application of natural and preformed physical modalities on the human organism. Neurorehabilitation is an interdisciplinary field - between neurology, neurosurgery and physical medicine. Many principles of Bioethics are obligatory in our rehabilitation and neurorehabilitation practice: human dignity and human rights, autonomy, consent, equality and equity, non-discrimination and non-stigmatization (for patients with disabilities). Several bioethical topics are important for neurorehabilitation: human research, neuro-ethics, pain management, assisted suicide, euthanasia.
2. Rehabilitation, physical medicine, neurorehabilitation
Rehabilitation is a functional therapy, based on a correct functional analysis. Rehabilitation is important element of the treatment of acute and chronic patients and is realized in departments and clinics of hospitals for active care or for long-term care. The rehabilitation process is done by a multi-disciplinary and multi-professional team (medical doctors, nurses, physiotherapists, occupational therapists, psychologists, etc.).
Neurorehabilitation (NR) is an interdisciplinary field - between neurology, neurosurgery and physical medicine.
The rehabilitation is the use of all means for reduction of the impact of disabling and handicapping conditions, and for social integration of the persons with disabilities.
The World Report on Disability of the World Health Organization and World Bank [1] defines the goals of rehabilitation, emphasizing on function: “prevention and slowing the rate of loss of function; improvement, restoration or compensation of lost function; maintenance of current function”. Contemporary rehabilitation applies a holistic approach to the patient, based on the International Classification, disability and Health (ICF) [2] and on clinical principles (Figure 1).
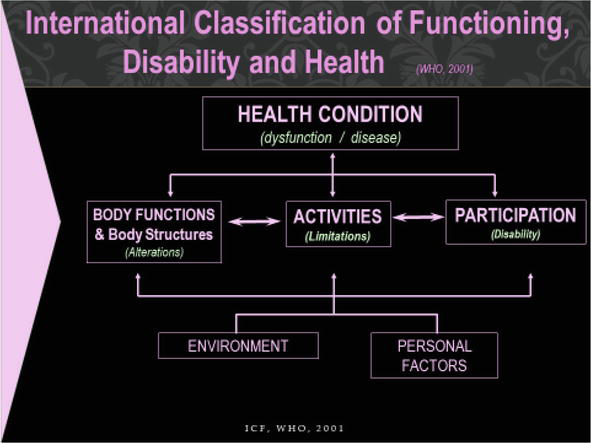
Figure 1.
ICF.
The rehabilitation process begins with a detailed functional assessment; on this base we formulate the (individual) rehabilitation goals, and we define the rehabilitation program, with evaluation of individual outcomes.
The “Rehabilitation team” includes several medical specialists and health professionals, including the patient and his/her proxy (Figure 2).
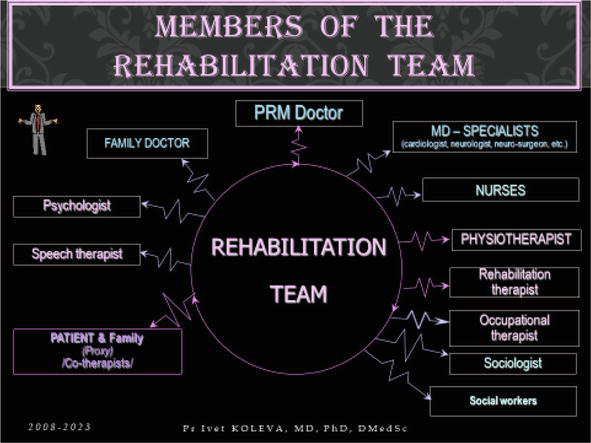
Figure 2.
Members of the rehabilitation team.
According the Definition, formulated by the Council of the European Union of Medical Specialists - UEMS [3]: “The medical act encompasses all the professional action, e.g. scientific, teaching, training and educational, clinical and medico-technical steps, performed to promote health and functioning, prevent diseases, provide diagnostic or therapeutic and rehabilitative care to patients, individuals, groups or communities in the framework of the respect of ethical and deontological value. It is the responsibility of, and must always be performed by a registered medical doctor or under his or her direct supervision and/or prescription.”
According the White Book of the specialty Physical and Rehabilitation Medicine (PRM) and the corresponding definition of the UEMS – PRM Section and Board [4]: PRM is an „independent medical specialty, oriented to the promotion of physical and cognitive functioning, activities (including environment), participation (including quality of life) and changes in personal factors and environment. It is thus responsible for the prevention, diagnosis, treatments and rehabilitation management of people with disabling medical conditions and co-morbidity across all ages.”
PRM is a “Medicine of Functioning”, focusing on the improvement of individual and social functioning of every patient [5]; so, the application ICF is crucial.
Ultimately, we observe an increasing number of chronic patients with invalidating conditions (predominantly of the nervous, motor and cardio-vascular systems). In NR clinical practice, we have patients with diseases of the central and peripheral nervous system (SNC and PNS). From the SNC conditions, we have patients with: post-stroke hemiparesis, multiple sclerosis, Parkinsonism; brain tumors and cerebral aneurysm (after neurosurgical intervention); traumatic brain injury and traumatic spinal cord injury (with quadriplegia or paraplegia); rare diseases (e.g. Amyotrophic Lateral Sclerosis, Barre-Lieou syndrome). From the group of PNS conditions, we have patients with: cervico-brachial plexopathy and lumbo-sacral radiculopathy, discal hernia (before and after neurosurgery); diabetic polyneuropathy; traumatic injury of peripheral nerves (with radial or peroneal or tibial paresis); Bell’s palsy; neuro-muscular diseases (e.g. Duchenne muscular dystrophy), etc. All these persons have somato-sensory, motor and/or cognitive dysfunctions and deficits; including: deficits in voluntary movements and postural adaptation, problems of the motor planning and coordination, functional ability and autonomy in activities in daily living (ADL) (Figure 3). Therefore, our patients need complex rehabilitation programs, with emphasis on functional recovery and amelioration of the autonomy in everyday life. In this process, we use different natural and preformed physical modalities. In clinical rehabilitation practice, we apply a holistic and patient-centered approach [4].

Figure 3.
Frequent dysfunctions and deficits in NR clinical practice.
The diagnosis in PRM is a combination of the medical diagnosis, based on the International Classification of Diseases (ICD), and a specific functional evaluation, based on the International Classification of Functioning, Disability and Health (ICF). Interventions in PRM are programed by the PRM physicians and are provided by the members of the rehabilitation team. We apply medicines, physical therapy, ergotherapy (occupational therapy), procedures with different natural and preformed physical factors, patient education. The principle of this complex program or rehabilitation “puzzle’ is presented in Figure 4.
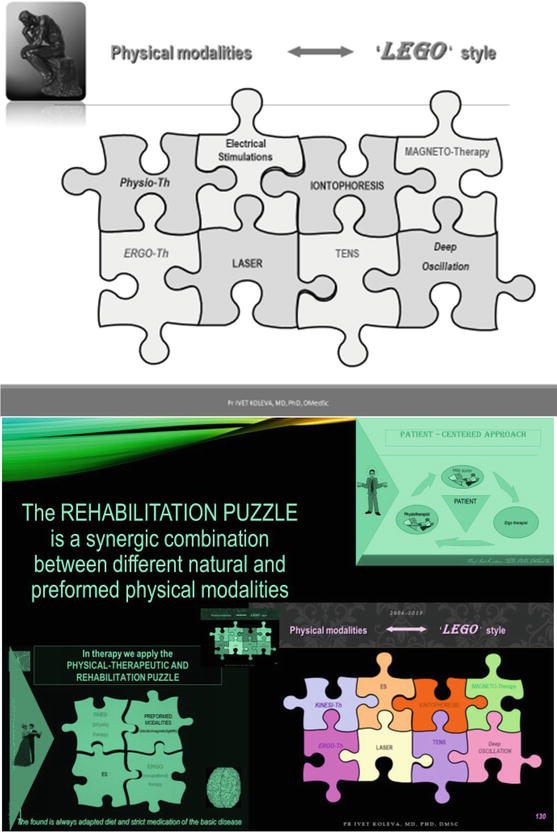
Figure 4.
The “rehabilitation puzzle”, applied in PRM practice.
Results of PRM interventions currently show reduction of impairments in body functions and activity limitations, influence on participation restrictions, and also reduction in costs, as well as decrease in mortality for certain groups of patients.
The goal of PRM is physical prevention, treatment by physical factors, and rehabilitation of physical or psychical dysfunction.
The medical doctors – PRM specialists are engaged in the clinical management of neurological and neurosurgical, rheumatological and traumatological, cardiological and cardio-surgical patients.
The Neurorehabilitation (NR) algorithm includes detailed functional assessment (based on ICD and ICF) and a therapeutic program of physical factors (movement, activities, mineral waters, electric currents, etc.). The “rehabilitation puzzle” (Figures 4 and 5) is a synergic combination of various physical modalities:
Natural physical factors: water (mineral baths), air (air baths), sun (sun baths), exercises (active, passive, against gravity, contra resistance), massage (manual, vibration, etc.), manual therapy techniques (traction, mobilization, and manipulation); occupational therapy (work and activities);
Pre-formed physical modalities: electric currents (low, middle and high frequency currents), electro-static field (deep oscillation); light (infrared, visible and ultra-violet light beams; Laser), magnetic field, ultra-sound, etc.).
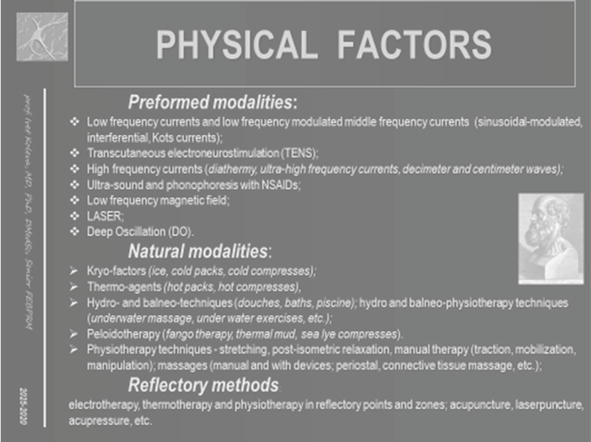
Figure 5.
Physical modalities (physical factors).
Physical and rehabilitation medicine investigates the effects of the application of natural and preformed physical modalities on the human organism.
The common NR-algorithm includes one or two pre-formed physical modalities (electrotherapy, magnetotherapy, phototherapy, ultrasound therapy), one thermo- or cryo-agent, two or three physiotherapeutic and ergotherapeutic procedures (including analytic exercises, post-isometric relaxation, stretching techniques, massage, training in activities of daily living, etc.).
3. Ethics, bioethics, and neurorehabilitation
3.1 Ethics and bioethics
Ethics is based on morality, answering the “classical” questions: what is right or wrong, what is just or unjust. The Code of Ethics includes: integrity, objectivity, honesty, moral values, responsibility, professional competence, confidentiality, professional behavior [6].
Bioethics is a expansion of the principal idea of the Hippocratic Oath “Primum non nocere” (the concept of “First Do Not Harm”) for all medical doctors and health professionals. According to definitions, bioethics is the “study of ethical issues arising from advances in biology and medicine” [7, 8]. It is also moral discernment in medical policy and practice. Bioethics is a field of study and professional practice, based on ethical principles. It includes the study of values (“ordinary ethics”) in relation to various medical and biological scientific fields [6, 7]. Bioethics derives from the Greek words bios (life) and ethos (behavior, moral nature). In 1926, Fritz Jahr applied this noun in an article about a “bioethical imperative” concerning the routine of usage of animals and plants in scientific research. In 1970, the American biochemist Van Rensselaer Potter applied the term and founded the global ethics.
Every medical doctor or health professional estimates the patients’ rights. In bioethics, we consider rights as the basic normative rules according to ethical theory. In rehabilitation practice, patients’ rights include rights related to treatment and safety, access to care and choice of care, participation in decision-making process, seek for a second opinion, compassionate palliative care and end-of-life care. For example, the right to appropriate medical care; right to informed consent; right to access information and medical record; right to privacy and confidentiality; right of choice of the physician and hospital; right to refuse diagnostics and treatment, right to decline participation in research; right to social contacts.
The Universal Declaration on bioethics and human rights [8], adopted by the General conference of UNESCO (in 2005), formulated the principles of bioethics (Figure 6). From the list of 15 principles, the most important for the NR practice remain: human dignity and human rights, benefit and harm, autonomy and individual responsibility; consent, privacy and confidentiality; equality, justice and equity; non-discrimination and non-stigmatization. Some patients in psychiatric, pediatric or geriatric rehabilitation, are persons without the capacity to consent, and for them the principle of respect for human vulnerability and personal integrity is essential. The principles of social responsibility and sharing of benefits are applied in many rehabilitation patients.
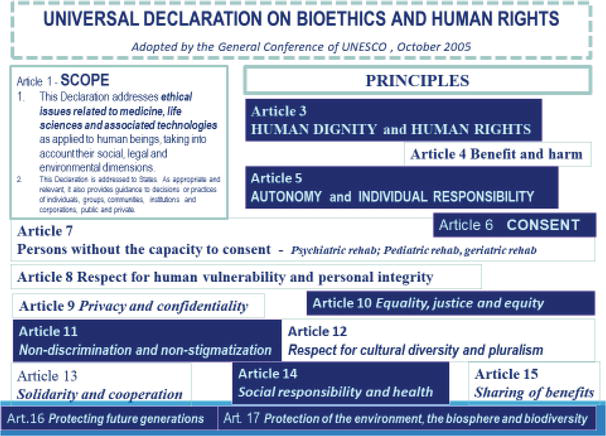
Figure 6.
Universal declaration on bioethics and human rights, 2005.
The list of topics concerning bioethics [9, 10, 11] covers many areas of medicine and health care (Figure 7). For NR- practice, the most important are: Human research, Neuroethics, Disability, Pain management, Assisted suicide and Euthanasia.
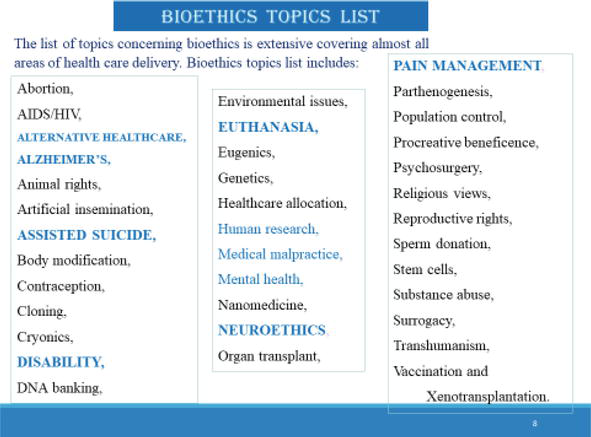
Figure 7.
Bioethics topics list.
3.2 Medical ethics
Medical ethics is the application of moral values in medicine and healthcare.
In the field of medical ethics, we note the central locus of the Declaration of Geneva, adopted by the Second General Assembly of the World Medical Association in 1948, last revised in 2017 [12]. This Declaration includes the physicians’ pledge upon honor for dedication “to the service of humanity”, and is known as the “Modern Hippocratic Oath”.
The World Medical Association (WMA) has established the International Code of Medical Ethics [13], adopted by the General Assembly of WMA in London in 1949, last revision in 2022. The Code states professional duties of medical doctors: principles of the physicians’ behavior and conduct, promotion of patient’s health and well-being, competent and qualitative care of patients in clinical practice. The Code states too principles of the physicians’ comportment to colleagues, to health professionals, to students, and to society. The Code is applied everywhere: in medical centers and in hospitals (emergency, acute departments, rehabilitation wards).
Common ethical principles, valid for every field of medicine, include: honesty, accuracy of actions, morality, equality, respect for rights, autonomy, integrity and adherence to the law, confidentiality, authenticity, responsibility, transparency [14].
These basic ethical principles are developed in the Ethics Manual of the American College of Physicians (ACP), first published in 1984 [15, 16]. The last (seventh) edition of 2018 introduced various new and expanded sections on some modern themes, as follows: Electronic communications, Telemedicine ethics, On-line professionalism, Internet and social media research. The Manual facilitates the decision-making in some cases presenting ethical dilemmas [17].
The Manual comments the basic ethical principles [17]: beneficence and non-maleficence, respect for patient’s autonomy, and justice. Various other ethical issues are discussed: professionalism of the medical doctor, communication between the physician and the patient; confidentiality; requirements for the medical record (paper or electronic); informed decision-making and consent. Special attention is paid to some “difficult” situations, as: health-care system catastrophes (infections, natural disasters, terrorist attacks); or cases of provided medical care to persons, proxy to the physician (with preexisting close nonprofessional relationship, or a reporting relationship), or VIPs; palliative care and end-of-life (incl. do-not-resuscitate order, euthanasia); cases of sexual involvement between physician and former patients; gifts from patients or industry; solid organ transplantation; etc.
Specific situations are explained, e.g. electronic communications and euthanasia.
Electronic communications are permitted in an established patient-physician relationship and they can be applied only with patient consent. A telemedicine encounter must begin with steps for creation of a connection, as during an in-person visit.
Most medical organizations do not support physician-assisted suicide and euthanasia. Ten American states and the District of Columbia have legalized the practice of physician-assisted suicide in USA [18]. The situation in Europe is similar: some countries accept (as Switzerland, Spain, Belgium, Netherlands); others do not agree with the physician-assisted suicide. This type of Death at Dignitas is for the moment not entirely accepted.
3.3 Bioethical principles in neurorehabilitation
Bioethical principles, important for NR, are: beneficence and non-maleficence (work for people’s welfare and reduction of harm: personal, social, organizational); fidelity and responsibility (and professional transparency); justice (equal access to medical care, without discrimination and biases) [14].
Many principles of the Universal Declaration on Bioethics and Human rights of UNESCO are obligatory in rehabilitation practice: human dignity and human rights, autonomy and individual responsibility, informed consent, equality and equity, non-discrimination and non-stigmatization (for patients with disabilities), social responsibility [8].
From the list of bioethical topics, the most important issues for NR are: human research, neuro-ethics, pain management, assisted suicide, euthanasia.
Many patients in NR-clinical practice have reduced autonomy and disability; they require assistive technologies, home adaptations, and complex pain management. In terminal cases, we have ethical problems and dilemmas (especially informed consent and the right to euthanasia).
Important bioethical aspects are the connections between the patient and the NR team; and the interactions between different members of the multi-professional multi-disciplinary NR team.
As in every hospital, the Informed consent is an obligatory rule in NR departments and clinics. Informed consent is the processus of instruction of the patient (by the health provider) about the benefits, risks and alternatives of the diagnostic or therapeutic procedures. In case of emergency or incompetence of the patient (in pediatric and geriatric rehabilitation, or in case of altered conscience), the informed consent is by the patient’s proxy.
Actually, in NR we apply largely Information and Communication Technologies (ICT): robotic rehabilitation with virtual reality; grasp and gait training with Exoskeletons, systems Tyro-motion and Lokomat, etc. Computer-based NR is very expensive, and this states the problem of equal access of all patients to contemporaneous (including ICT-based) methods for diagnostics and treatment.
3.4 Patients’ rights in neurorehabilitation
The Declaration of Lisbon (1981, last revision in 2015) defines the basic patient’s rights [19]: right to medical care of good quality, right to freedom of choice, right to self-determination, right to information, right to confidentiality, right to health education, right to dignity, right to religious assistance.
Every physician must always act in the patient’s best interest, even in cases of unconscious or legally incompetent patient (altered brain functioning or loss of consciousness, consequence of traumatic brain injury, concussion or psychiatric condition). In this situation, the medical doctor necessitates the decision of the patient’s official representative. Diagnostic or therapeutic procedures against the patient’s will can be realized only in exceptional cases, in compliance to the principles of medical ethics.
In a previous publication [20], we analyzed the opinion on ethical issues of academic staffs, rehabilitation staffs and patients from acute and long-term rehabilitation departments. Our results demonstrated the close relationship between the PRM-clinical practice and many principles of the Universal Declaration on Bioethics and some typical bioethical topics, especially human research, neuroethics, pain management, euthanasia. From the Declaration on Bioethics and Human Rights of UNESCO (2005) the most important for NR are: human dignity and human rights, autonomy; informed consent, persons without the capacity to consent (psychiatric rehabilitation; pediatric rehabilitation, geriatric rehabilitation); equality and equity; non-discrimination and non-stigmatization (for patients with disability). For the
A collective of several academics of Canadian Universities (McGill University, McMaster University, Montreal University, Ottawa University) investigated the problem of
Ghostal et al. [23] discuss problems of
We observed some parallels between concerns of our patients and staff of geriatric rehabilitation department and opinions of
3.5 Bioethical issues in elderly patients in neurorehabilitation
In October 2022 in Berlin, Germany, the World Medical Association accepted a Declaration on Discrimination against elderly individuals within healthcare settings [25]. The Declaration of Berlin recommends to eliminate all forms of discrimination due to health and age. The need for a holistic approach in elderly is discussed. The Declaration commends to medical doctors include to provide healthcare of scientific and human quality according to good medical practice to all patients, without any discrimination.
3.6 Bioethical issues in the field of research in neurorehabilitation
The basic principles of the Ethics of Research are explained in the “Belmont Report: Ethical Principles and Guidelines for Research Involving Human Subjects” [26]. These three principles are valid in rehabilitation and neurorehabilitation: respect for persons, beneficence and non-maleficence and justice. The first principle of Respect for persons includes the requirement to recognize autonomy of patients and the obligation to defend persons with reduced autonomy. The second principle of beneficence and non-maleficence is based on the Hippocratic aphorism of “First, do not harm” and includes the responsibility to assure the well-being of patients. The third principle of Justice assure the equal attitude to all patients. Practical applications of these principles include the Informed consent, the assessment of risks and benefits, and the selection of subjects for investigations.
Research in NR are suborned to the 10 principles for investigation, formulated in the Nuremberg Code [27], with special consideration to the voluntary informed consent of every participant.
The same principles are mentioned in the Seventh Edition of the Ethics Manual of the American College of Physicians (ACP), elaborated by the Ethics, Professionalism and Human Rights Committee (EPHRC) [17]. The first principle of respect for persons is transformed into respect for patient autonomy, explained as “duty to protect and foster a patient’s free, uncoerced choices”. The second principle of beneficence is divided into beneficence and non-maleficence. Beneficence is explained as “duty to promote good and act in the best interest of the patient”. The non-maleficence is described as “duty to do no harm to the patient”. The third principle of Justice is defined as “equitable distribution of the life-enhancing opportunities afforded by health care”.
The same Ethics Manual of the ACP postulates the requirement of a Decision from an Institutional Review Board (IRB) for every research. This step assures the protection of the human subjects, an acceptable benefit-risk ration, adequate informed consent process and confidentiality safety.
The Declaration of Helsinki of the World Medical Association clarifies the Ethical principles for medical research, involving human subjects [28]. The document is adopted by the WMA General Assembly in Helsinki in 1964 and is amended by next general assemblies, last one in 2013. According this Declaration the duty of medical doctors is to protect the life and health, to respect the dignity and integrity, to esteem the privacy, and confidentiality of personal information of research subjects. An analysis of risks, burdens and benefits is done. Special attention is paid to privacy and confidentiality, informed consent, use of placebo, etc.
3.7 Bioethics and education in neurorehabilitation
The title “doctor” comes from Latin: “
The World Federation for Medical Education (WFME) has elaborated on global standards for basic medical education (last update 2020) [29]. Standards for basic medical education include curriculum content and structure, organization, educational resources, requirements for the academic staff, process of admission of students. The education of future physicians is discussed in many publications [30].
In 2021, WFME published the “Standards for distributed and distance learning in medical education” [31]. Different forms of learning are debated: distance learning, distributed learning, online learning, e-learning, virtual learning, and flexible learning. The requirements for the design of a typical course is presented [31].
For a post-graduate course in neurorehabilitation (during long-life-learning of medical doctors – specialists and trainees in PRM, and of health professionals), we made a curriculum [32], including some principal educational modules, as follows: neuroanatomy, neurophysiology, modern methods of NR, etc. The theoretical part was done online, with power-point presentations, electronic books [33] and videos. The practical part must be face-to-face to the patients. In exceptional circumstances (COVID-pandemic), we used videos with case studies of real or virtual patients. The assessment of learners’ competences was done using tests (some of them – online) and a practical exam (face-to-face to a patient). The decision-making process is easier in case of traditional learning (with a patient). During the COVID-pandemic, we prepared and realized educational courses on the topics “Rehabilitation in SARS-CoV-2” [34] and “ICT-based Neurorehabilitation in Neuro-COVID” [35].
4. Case report with ethical dilemmas
4.1 Clinical case presentation
4.1.1 General case presentation
We present a patient, who is a 23-years-old male with inferior paraplegia, due to a cranio-cerebral and severe spinal cord traumatic injury. The trauma is a consequence of an occupational accident – fall from a height of about 15 meters, from a construction site.
4.1.2 Medical dimension
The patient had trauma of the head, chest, spine and pelvis. MRI-data of polyfragmentary fracture of the bodies of thoracic vertebral bodies Th7 and Th8, with bone fragments in the spinal cord and anatomic discontinuity in the thoracic myelon, fracture of the transversal processes of Th4-Th8 vertebrae. Diagnosed right hemothorax; pneumothorax, multiple fractures of the dorsal part of the 4th to the 7th right ribs, dorsally; fractures of the scapula and the right acetabulum.
During the first month, intensive care and resuscitation, ventilator support and neuro-surgical intervention were performed – decompression of the thoracic spinal cord, with subsequent transpedicular osteosynthesis (Figure 8). During the operation, a communication between the hemothorax and the thoracic spine was observed.
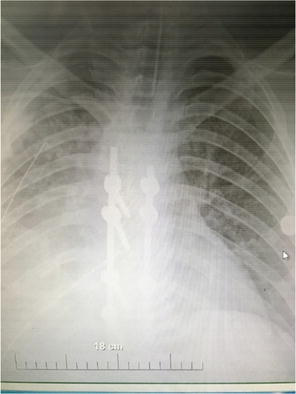
Figure 8.
Transpedicular stabilization of the thoracic spine.
On the admission at the Hospital for Long-term care and Rehabilitation – Department of Physical and Rehabilitation Medicine (PRM), we observed an inferior central paraplegia with complete anesthesia in lower extremities, with a sensory level Th11 on the right side and Th12 on the left side.
During the stay in the PRM-Department (for about 4 weeks), a verticalization was done; every day a NR-complex was conducted, including physiotherapy (analytic exercises, balance training), occupational therapy (ADL training, gait training with a walker, then with crutches), and preformed physical modalities (electrical stimulations for feet extensors; lasertherapy for an intergluteal decubital wound of grade 1–2).
4.1.2.1 Ethical problem 1
The in-patient rehabilitation is covered by the National insurance funds in our country only for a stay period of 7 to 10 days, the remaining days must be paid by the patient. However, the patient’s needs require at least 3 months of active rehabilitation in a hospital setting.
4.1.2.2 Ethical problem 2
A NR-course of 10 procedures of robotic neurorehabilitation is also offered; but this is a paid procedure (and quite expensive). The costs are high and not covered by the National insurance funds.
4.1.2.3 Ethical problem 3
It is a well-known fact, that the medical specialists and the health professionals have the duty to tell the truth to their patients. Access to information is an inalienable human right (and patient’s right, of course). However, the patient must be conditioned to realize and accept the truth. Often, in such situations, we observe the phenomenon of “difficult” or “delayed” acceptance of the “new” situation – paraplegia, in this case. The patient can pass through phases of: denial, realization, depression, despair, resignation.
The prognosis of our patient with standard treatment is “stabilization” of the inferior paraplegia and autonomy with a wheelchair. We explained the scenario to the patient’s parents (accompanying him at this moment). At the insistence of the mother and father, and with the advice of our neuropsychologist and after a psychiatric consultation, we delayed the communication of the full prognosis to the patient for about 2 weeks, as he still had some residual cognitive impairment and emotional instability due to the traumatic brain injury (TBI). The initial reaction of the patient to the accident imposed the necessity of consultation by a psychiatrist, systematic antidepressant therapy and psychotherapy.
There is no guarantee of the recovery of paraplegia in traumatic spinal cord injury (SCI). Partial reduction is possible and transformation into paraparesis, but only in case of active rehabilitation.
4.1.2.4 Ethical problem 4
In the context of modern communication channels, patients and his proxy have access to information for different types of “miraculous recovery”. Patient and his family asked us about the possibility of stem cells transplantation. We answered sincerely that some authors consider this operation effective, but without sufficient data, according to the requirements of the evidence-based medicine. In some clinics (but not in our country) this expensive operation is performed, but without guarantees. In cases of professionally performed operation, no negative effects are expected. The final decision is ultimately up to the patient and the family.
4.1.3 Nursing dimension
At the beginning of the stay, the patient presented subfebrility, due to urinary tract infection. Many measures were initiated: catheter replacement, catheter flushes, antibiotic treatment for about 10 days, with periodical sterile urine investigations.
Due to the persistent bed rest, a decubital wound was developed. Many decubitus prevention measures were placed: anti-decubital mattress, back skin inspections, wound dressings.
On several occasions, sedatives and analgesics had to be given.
The patient was accompanied by family members (his mother and father took turns to accompany him). No volunteer assistance was needed.
4.1.4 Functional assessment and neurorehabilitation dimension
We realized some measures for prevention of the consequences of the prolonged bed rest: position treatment (gradual lifting of the upper trunk), passive exercises for lower extremities, including ‘muscle pumps’ (ankle flexion and extension), balance training in a sitting position. In the complex NR program we included elements of physiotherapy, massage, ergotherapy (occupational therapy), preformed physical modalities (electrical stimulations, laser).
4.2 Patient’s views. Social dimension. Organizational dimension
The ethical principle of justice must be respected.
The dignity of the patient and his rights must be esteemed.
4.2.1 Patient’s opinions and social dimension
The patient accepted the prognosis (inferior paraparesis or paraplegia), but for him this partial or complete loss of mobility in lower limbs is a problem. Until the trauma, he was physically active. His profession is based on physical activity – he is master-builder. In the future, he must do a professional re-orientation and choose a profession not requiring physical load and possible in a sitting position.
Until the moment of the accident, the patient does not belong to a religious community. At the moment of his transfer to the rehabilitation clinic, the life of the patient is no longer in danger. There is no need for a priest.
The consequences of the trauma are quite serious – both in terms of social and professional engagement, and in terms of remuneration.
We counseled the patient and his parents to seek a professional advice from a lawyer, specialist in labor law, as this was an accident at work. Financial security is important both to carry out the rehabilitation process and to ensure a minimal standard of life in the future.
During the stay at the rehabilitation ward, his girlfriend visited the patient once (no marriage, no children).
The effects of the cranial and spinal cord trauma are difficult for every person to overcome. However, they are especially difficult for a young person, living outside the capital.
4.2.2 Organizational dimension
The bioethical principle of equality, justice and fairness must be respected.
All patient’s rights are esteemed: right to quality health services; right to sufficient information with the view of informed consent and decisions concerning the future treatment and rehabilitation; right to access any medical information; right to confidentiality; right to personal dignity; right to self-determination.
4.3 Patient’s autonomy. Informed consent
The ethical principle of respect for autonomy is respected. During his stay, the patient was informed in details about his condition and prognosis. Every diagnostic and therapeutic method was explained explicitly to the patient, with existing options to accept or to deny the respective procedure. We need the signed informed consent of the patient at the entry, and before every diagnostic or therapeutic procedure.
In rehabilitation, the active participation of the patient and his family is very important. We stimulated the patient’s personal responsibility. The members of the family are treated as co-therapists.
4.4 Responsibility of medical specialists and health professionals
The patient received the exact medications in the right doses, the exact rehabilitation procedures – at precisely defined dosages.
During the daily visits and the weekly main visit, the opinions of the individual members of the medical team (neurologist, PRM-doctor, urologist, etc.) were commented on, as well as the opinions of different health professionals (nurses, physiotherapists, occupational therapists). Practically, the patient and his parents participated as listeners during these discussions, and also as active members of the rehabilitation team. We believe that such discussions should take place with the majority of patients. All medical specialists and health professionals treat confidential information responsibly (with confidentiality).
Rehabilitation patients need a care from an extended multi-professional and multi-disciplinary rehabilitation team, including: doctors – specialists (in Neurology, Orthopedics and Traumatology, Cardiology, Urology, Pulmology, Rheumatology, Psychiatry, etc.); nurses; therapists (physiotherapists, occupational therapists), neuro-psychologist, clinical psychologist; social worker; jurist.
4.5 Decision-making. Special circumstances
4.5.1 Decision-making
In practice, on the admission to a hospital for long-term care and rehabilitation, the patient is informed about the necessary diagnostic and therapeutic techniques. The signature of an informed consent is obligatory at the entry and before any procedure. In case of patient’s incompetence, suggested by a neuro-psychologist and diagnosed by a physician – specialist in psychiatry, the decision can be made by the patient’s proxy (in this case –his parents).
On the issue of stem cell transplantation, we informed the patient and relatives of the possible risks of surgery. The patient and his family have to decide. The medical and paramedical staff must respect their decision and choice. We are obliged to provide all available medical information – for and against.
4.5.2 Special conditions
During the first two weeks of his hospital stay, our patient had some cognitive dysfunctions and psycho-emotional lability. Therefore, we decided to consider his parents’ request and the psychologist’s advice to delay the full communication of the prospects to the patient. We informed on time the mother and father of the prognosis, in 2 weeks – we described the “full truth” to the patient. The emotional reaction of the patient was development of a depressive state (suggested by our psychologist and diagnosed by a psychiatrist). In this situation we were obliged to include anti-depressive medication and psychotherapeutic course.
4.6 Right to modern therapeutic methods
Every patient has the right to be treated with contemporaneous methods. The problem is that some modern procedures are very expensive and they are not covered by the National health insurance funds. Therefore, the patient must pay for this.
Finally, we find the possibility to obtain thе necessary funds from a benevolent organization and this young man received the full possibility to receive robotic rehabilitation, using neurorobots - the device Lokomat of Hocoma (Figure 9).
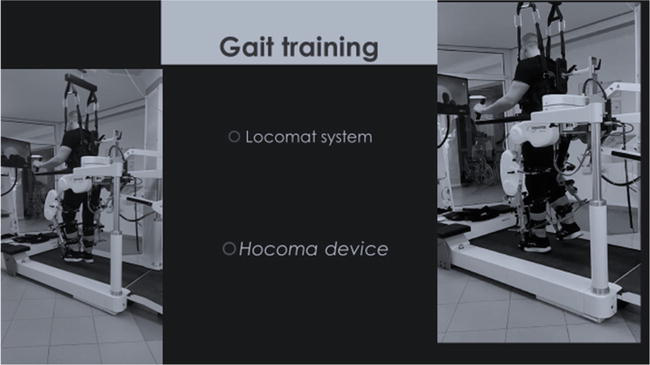
Figure 9.
Robotic neurorehabilitation.
4.7 Prevention of complications
The possible complications in quadriplegia and paraplegia due to TBI and SCI include: deep vein thrombosis, pulmonary thromboembolism, urinary infections, decubital wounds, muscle and joint contractures, arterial hypotonia and orthostatic hypotension, etc.
We made periodical observations and tests, for diagnostic of the early stages of possible complications.
4.8 Right to assistive technologies and to home adaptations
The patient needs assistive technologies and home adaptations, due to the prognosis – spastic paraplegia or paraparesis. The necessary technical aids in this case are: wheelchair, crutches, eventually – canes (Figure 10). The minimum home adaptations include: wheelchair ramp, adaptations in the bathroom and in toilet (Figure 11).

Figure 10.
Technical aids.

Figure 11.
Home adaptations.
Part of these technical aids and home adaptations can be assured by the social security funds.
5. Conclusion
Bioethics is an important link between rehabilitation and human values.
Bioethics principles are important element in the everyday clinical practice of neurorehabilitation.
Every member of the multi-professional and multi-disciplinary rehabilitation team must be informed about his duty to consider bioethical laws and patients’ rights.
List of acronyms and abbreviations
American College of Physicians | |
Activities of daily living | |
Corona virus disease | |
Ethics, Professionalism and Human Rights Committee | |
International Classification of Diseases | |
International Classification of Functioning, Disability and Health | |
Information and Communication Technologies | |
Magnetic Resonance Imagery | |
Neurorehabilitation | |
Physical and rehabilitation medicine | |
Spinal Cord Injury | |
Traumatic Brain Injury | |
Union of European Medical Specialists | |
World Health Organization | |
World Federation for Medical Education | |
World Medical Association |
References
- 1.
World Health Organization. World Report on Disability. [Internet]. Available from: https://www.who.int/publications-detail/world-report-on-disability [Accessed: May 15, 2012] - 2.
World Health Organization. International Classification of Functioning, Disability and Health: ICF. Geneva: WHO; 2001 - 3.
European Union of Medical Specialists. European Definition of Medical Act. Meeting in Munich [Internet]. 2005. Available from: http://www.uems-slm.org/uems/index.php?id=26 [Accessed: May 15, 2012] - 4.
Gutenbrunner C, Ward AB, Chamberlain MA. White book on physical and rehabilitation medicine (PRM) in Europe. Produced by the section of PRM, Union Européenne des médecins spécialistes (UEMS), European board of PRM and académie Européenne de médecine de réadaptation in conjunction with European society for PRM. Produced 2006. Journal of Rehabilitation Medicine. 2007; 39 :1-48. DOI: 10.2340/16501977-0028 - 5.
European Physical and Rehabilitation Medicine Bodies Alliance. White Book on Physical and Rehabilitation Medicine (PRM) in Europe. Chapter 7. The clinical field of competence: PRM in practice. European Journal of Physics Rehabilitation Medicine. 2018; 54 (2):230-260. DOI: 10.23736/S1973-9087.18.05151-1 - 6.
Ten Have H. Global Bioethics: An Introduction. London: Routledge; 2016 - 7.
Engelhardt TH, editor. Global Bioethics: The Collapse of Consensus. Salem: M&M Scrivener Press; 2006 - 8.
UNESCO. Bioethics. E-book. Sofia: UNESCO; 2018. p. 70 - 9.
Mitchell CB, Pellegrino E, Elshtain JB, Kilner J, Rae S. Biotechnology and the Human Good. Washington, DC: Georgetown University Press; 2007 - 10.
Bennett B, editor. Health, Rights, and Globalisation. Surrey, UK: Ashgate; 2006 - 11.
Cherry M, Peppin JF. Regional Perspectives in Bioethics. Annals of Bioethics. Lisse, The Netherlands: Swets & Zuietlinger; 2003 - 12.
World Medical Association. Declaration of Geneva [Internet]. Available from: www.wma.net/what-we-do/medical-ethics/declaration-of-geneva/ [Accessed: May 05, 2023] - 13.
World Medical Association. WMA international code of medical ethics [Internet]. Available from: www.wma.net/what-we-do/medical-ethics/ [Accessed: May 05, 2023] - 14.
World Medical Association. Medical Ethics Manual. 3rd edition 2015 [Internet]. Available from: www.wma.net/wp-content/uploads/2016/11/Ethics_manual_3rd_Nov2015_en.pdf [Accessed: May 05, 2023] - 15.
American College of Physicians Ethics Manual. Part 1: History; the patient; other physicians. American College of Physicians. Annals of Internal Medicine. 1989; 111 :245-252 - 16.
American College of Physicians Ethics Manual. Part 2: The physician and society; research; life-sustaining treatment; other issues. American College of Physicians. Annals of Internal Medicine. 1989; 111 :327-335 - 17.
Sulmasy LS, Bledsoe TA, for the ACP Ethics, Professionalism and Human Rights Committee. American College of Physicians Ethics Manual. Seventh edition. Annals of Internal Medicine. 15 Jan 2019; 170 (2_Suppl):S1-S32. DOI: 10.7326/M18-2160. PMID: 30641552 - 18.
Sulmasy LS, Mueller PS for the Ethics, Professionalism and Human Rights Committee of the American College of Physicians. Ethics and the legalization of physician-assisted suicide: An American college of physicians position paper. Annals of Internal Medicine. 2017; 167 (8):576-578. DOI: 10.7326/M17-0938 - 19.
World Medical Association. WMA Declaration of Lisbon on the rights of the patient [Internet]. 1981. Available from: www.wma.net [Accessed: May 05, 2023] - 20.
Koleva I, Yoshinov B, Gerenova J, Dimitrov T, Traykovska A, Yoshinov RR. Bioethics and Physical medicine: From the heritage of Asclepius and Hippocrates to the contemporary rehabilitation clinical practice. In: Current Innovations in Medicine and Medical Science. Vol. 7. London: BPI; 2022. pp. 42-66. DOI: 10.9734/bpi/cimms/v7/8594F - 21.
Blackburn E, Durocher E, Feldman D, Hudon A, Laliberté M, Mazer B, et al. Supporting, promoting, respecting and advocating: A scoping study of rehabilitation professionals’ responses to patient autonomy. Canadian Journal of Bioethics. 2018; 1 :22-34. DOI: 10.7202/1058249ar - 22.
Uddin T, Shakoor MA, Rathore FA, Sakel M. Ethical issues and dilemmas in spinal cord injury rehabilitation in the developing world: A mixed-method study. Spinal Cord. 2022; 5 :1-6 - 23.
Ghoshal A, Salins N, Damani A, Chowdhury J, Chitre A, Muckaden MA, et al. To tell or not to tell: Exploring the preferences and attitudes of patients and family caregivers on disclosure of a cancer-related diagnosis and prognosis. Journal of Global Oncology. 2019; 5 :1-12. DOI: 10.1200/JGO.19.00132 - 24.
Chaturvedi SK. Ethical dilemmas in palliative care in traditional developing societies, with special reference to the Indian setting. Journal of Medical Ethics. 2008; 34 (8):611-615. DOI: 10.1136/jme.2006.018887 - 25.
World Medical Association. WMA Declaration of Berlin on Discrimination against Elderly Individuals within Healthcare Settings [Internet]. 2022. Available from: www.wma.net [Accessed: May 05, 2023] - 26.
Department of Health, Education, and Welfare. Office of the Secretary: Protection of Human Subjects. Belmont Report: Ethical principles and guidelines for the protection of human subjects of research. Report of the National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research. Agency: Department of Health, Education, and Welfare. Action: Notice of Report for Public Comment. Federal Register. 1979; 44 (76):23192-23197 - 27.
Katz J. The Nuremberg code and the Nuremberg trial: A reappraisal. Journal of the American Medical Association. 1996; 276 (20):1662-1666. DOI: 10.1001/jama.1996.03540200048030 - 28.
World Medical Association. Declaration of Helsinki. Ethical principles for medical research involving human subjects [Internet]. 2013. Available from: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ [Accessed: March 09, 2018] - 29.
World Federation for Medical Education. Global Standards for Quality Improvement: Basic Medical Education. The 2020 revision [Internet]. Available from: www.wfme.org [Accessed: May 15, 2023] - 30.
Grant J. Principles of contextual curriculum design. Chapter 5. In: Swanwick T, Forrest K, O’Brien BC, editors. Understanding Medical Education. Evidence, Theory and Practice. Third ed. Oxford: Wiley Blackwell; 2019. pp. 71-88 - 31.
World Federation for Medical Education. Standards for distributed and distance learning in medical education [Internet]. 2021. pp. 1-48. Available from: www.wfme.org [Accessed: May 17, 2023] - 32.
Koleva I, Hadjiyanev A, Yoshinov B. Electronic learning using an e-book in neurorehabilitation and neuroergotherapy for medical specialists and health professionals, members of the multi-disciplinary neurorehabilitation team. In: 14th International Technology, Education and Development Conference, Valencia, Spain, 2-4 March, 2020. INTED2020 Proceedings. Valencia: IATED; 2020. pp. 6488-6494. DOI: 10.21125/inted.2020. ISBN: 978-84-09-17939-8. ISSN: 2340-1079 - 33.
Koleva I, Yoshinov B, Yoshinov R. Bases of Neurorehabilitation: E-book. Sofia: SIMEL; 2020. pp. 1-584 - 34.
Koleva I, Yoshinov B, Yoshinov R. Rehabilitation in SARSCoV2: Structuration of an educational module and evaluation of students’ competences and satisfaction. In: 14th Annual International Conference of Education, Research and Innovation. Online Conference. 8-9 November, 2021. ICERI2021 Proceedings. IATED; 2021.pp. 3266-3274. DOI: 10.21125/iceri.2021. ISBN: 978-84-09-34549-6. ISSN: 2340-1095 - 35.
Yoshinov R, Yoshinov B, Koleva IB. Introduction of electronic learning in the educational module “ICT-based neurorehabilitation of Neuro-COVID” with clinical cases. In: 17th International Technology, Education and Development Conference, Valencia, Spain, 6-8 March, 2023. INTED2023 Proceedings of Conference. Valencia: IATED; 2023. pp. 2158-2165. DOI: 10.21125/inted.2023. ISBN: 978-84-09-49026-4. ISSN: 2340-1079