
Abstract
As humans, our most essential and desirable goals involve social interactions, connectedness, and acceptance. However, social rejection or exclusion, perceived discrimination or humiliation, and loneliness can drastically impact our psychological well-being. Negative social behaviors like bullying and mobbing can be particularly damaging and highlight certain types of abusers. Effective interventions require a deep understanding of negative peer interactions’ functions, motivations, and dynamics. This chapter examines these dimensions through a cognitive paradigm lens and the classification and characteristics of specific self-defeating behavioral patterns in the Life Space Crisis Intervention (LSCI) Model. We delve into the underlying psychological structure of both parties in a bullying situation, the different types of bullying relationships and patterns of interaction, and the primary directions for intervention.
Keywords
- social interactions
- aggressive behaviors
- bullying
- cognitive paradigm
- LSCI method
1. Introduction
The goals of professional intervention in managing bullying relationships are to eliminate the bullying action and its effects and help those involved to learn appropriate behaviors. In order to achieve these objectives, it is crucial to have a thorough comprehension of the dynamics involved in bullying. Since bullying is such a complex social relation, there are different levels of analysis of existing data and different paths of action. This chapter analyzes bullying on different levels. We consider it worthwhile to analyze bullying on four levels: descriptive, diagnostic, predictive, and prescriptive.
At a descriptive level, we focus on the genesis of aggressive behavior, its neurophysiologic roots, functions, and variations. Professionals must understand that all behaviors, even aggressive behavior such as bullying, serve a purpose and fulfill specific needs. It is crucial to acknowledge the needs of the aggressive child and work toward finding positive ways to fulfill them. Utilizing a descriptive approach enables practitioners to identify and describe the behavior and its underlying functions.
It is crucial to deeply understand aggressive behavior and its functions and identify possible behavioral patterns in aggressive children (diagnostic level). The cognitive paradigm and Life Space Crisis Intervention (LSCI) techniques utilize conceptual models to understand aggressive behavior and conflict cycles, which help practitioners interpret behaviors and choose appropriate interventions.
Predictive analysis is employed when we make assumptions about the child’s response to a specific intervention. Based on the prognostic level, we could build a hypothesis about how our intervention will model the behavior. It is important to remember that every model is merely an estimation of reality and that behavior involves a vast number of variables. Therefore, it is necessary to conduct interventions through experimentation. Usually, we test our assumptions by analyzing data and utilizing preexisting models.
In guiding our practice through case analysis, we rely on the prognostic level and data-driven approaches for successful interventions. It is essential to observe the transfer of newly acquired knowledge and skills to similar situations, as well as the restructuring of cognitive schemes, to determine the effectiveness of an intervention.
We need models, not recipes! The models are based on relevant, significant scientific theories/knowledge and empirically validated strategies and practices.
A profound, in-depth understanding of theories, scientific knowledge, and their logical explanatory and intervention models favor insights into problem-solving and sustain informed, justifiable, flexible, and efficient interventions.
Initial training and continuous professionalization should develop this assessment and diagnostic knowledge and skills, compulsory for informed, independent, autonomous, insightful, inspired, and flexible educational specialists.
2. The descriptive level: human behavior
Throughout our lives, each of us displays a wide range of emotional and behavioral reactions collectively known as human behavior. This subject is essential to many fields of study, including neurophysiology, psychology, sociology, and philosophy. Researchers in these areas have conducted extensive studies, observations, and experiments to develop theories about the factors that influence human behavior, the various stages of its development, and the different types of behaviors that we exhibit.
Understanding the reasons and motives behind the emergence and development of various behaviors is crucial, and there are several reasons why. First, this helps us identify the critical factors and circumstances that reinforce or eliminate a particular behavior. Second, by observing and deciphering behavioral patterns, we can gain insights into the human mind, including thoughts, emotions, attitudes, and values.
Behaviors are sorted into normal/abnormal, rational/irrational, accepted/unaccepted, and appropriate/inappropriate based on different criteria and perspectives. Although these categories are historically, culturally, and socially dependent, they remain relevant in education, rehabilitation, and psychotherapy. We employ these behavioral classifications as criteria in the diagnostic process and interventions.
Human behavior is complex and can take various forms, such as impulsive, automatic, emotional, controlled, rational, and mature. Developmental psychologist Perry [1] explains that these behaviors depend on the nervous system’s development level. The nervous system is structured hierarchically. Lower structures like the subcortical, limbic, midbrain, brainstem, and autonomic systems generate diverse reactions, from reflexive responses in newborns to abstract reasoning in adolescents and young adults. This neurosequential approach to therapy highlights the significance of evaluating a child’s developmental age, including their physical, emotional, social, cognitive, and behavioral levels. As a result, educational and therapeutic expectations and activities can be tailored accordingly [1].
The maturity of neurological structures plays a crucial role in children’s emotional self-regulation and behavioral self-control. However, external factors like the child’s environment and life experiences influence these abilities through social learning, modeling, and altering neurological structures and functions.
The situation’s characteristics can significantly influence impulsive and automatic behavioral responses. In the face of perceived danger or threat, the body instinctively reacts with fight, flight, or freeze responses. These reactions have specific objectives, such as avoiding or escaping, seeking attention, asserting power, or seeking vengeance.
2.1 Aggressive behaviors: determinants, types, and functions
Human aggression and aggressive reactions are multifaceted [2], involving genetic and hereditary factors, predispositions, or acquired, learned responses to specific events. The explanatory theories on aggression range from extreme positions. The biological approach searches for evidence of genetic predispositions for aggression. The environmentalist approach presents crucial environmental factors predisposing to aggressive reactions.
According to the behavioral model proposed by Nietzel, Hasemann, and Lynam [3], four factors can contribute to developing aggressive behavior across an individual’s lifespan. These factors include distal triggers of violence, early signs of a predisposition to violence during childhood, aggravating factors like traumatic events or stressful life experiences, and specific variables that can sustain aggressive behavior.
Bandura’s social learning theory [4, 5] suggests that external reinforcement and internal factors, like emotions and thoughts, influence human behavior, such as aggression. Bandura highlights the importance of motivation in shaping and maintaining behavior. Meanwhile, Stoff and Cairns [6] take a developmental psychobiological approach to understanding aggression, examining both top-down and bottom-up factors contributing to such behavior.
At every stage of life, specific factors affect the likelihood of aggressive behavior. There are various types of aggressive behaviors with specific motivations and meanings. As humans develop biologically and neurologically during childhood and adolescence, their aggressive reactions undergo significant changes, primarily due to developments and changes in brain structure and function [1]. Environmental conditions, life events, personal beliefs, and personality also play a crucial role in shaping an individual’s response to aggression [7]. Economic, psychological, and environmental stressors can further impact an individual’s behavior [8, 9].
According to research cited in Tremblay et al. [10], childhood aggression can take various forms. These forms include instrumental aggression (aimed at obtaining or retrieving an object or situation), teasing aggression (which lacks a specific goal), defensive aggression (a reaction to an attack), and game aggression (stemming from rough-and-tumble play). Categorizing aggression is crucial for understanding the genetic, biological, and social factors influencing aggressive behavior. This understanding can help improve educational and therapeutic approaches.
2.2 Functions of the aggressive behaviors
Every behavior, including aggression, serves a purpose to fulfill a need. According to Maslow’s theory of human needs [11], needs are arranged hierarchically, beginning with physiological needs and advancing to safety needs, love and belonging, self-esteem, self-actualization, and self-transcendence. This theory highlights the significance of meeting fundamental needs before pursuing higher ones, such as self-actualization and self-transcendence.
According to Max-Neef [12], the human needs for development should be viewed as a comprehensive and interconnected system, with no fixed order of importance, except for the essential need for subsistence. To establish a Human Scale Development, Max-Neef categorized human needs into two groups: existential (being, having, doing, and interacting) and axiological (subsistence, protection, affection, understanding, participation, creation, leisure, identity, and freedom). This matrix can be utilized for diagnostic purposes, planning, assessment, and evaluation.
The Circle of Courage [13] presents a practical framework for comprehending human needs and their significance in fostering resilient and successful individuals. This model, derived from the medicine wheel of North American tribal communities, symbolizes balance and harmony. It emphasizes the critical requirements for positive human development, namely belonging, mastery, independence, and generosity, which are essential after fulfilling basic needs such as food, water, and shelter. Psychologically, these needs translate to attachment, achievement, autonomy, and altruism.
Numerous theories [14, 15, 16, 17] suggest that all human behaviors, whether reasonable or unreasonable, appropriate or inappropriate, are motivated by the need to fulfill an objective and satisfy a need. Every human behavior serves a crucial purpose, sometimes even vital to the individual. In the context of education, intervention, or therapy, it is unhelpful and inefficient to impede or reject the function of any behavior. Instead, we should strive to promote socially accepted, appropriate, and suitable ways of action.
According to Adler [14], as social beings, humans have an inherent need for acceptance and belonging, which drives their behavior toward achieving social approval. Dreikurs [15] believes all human behaviors are motivated by fulfilling significant needs, such as attention-seeking, power-seeking, revenge-seeking, and failure-avoiding. Building on Adler’s work, Nelsen [16] identifies four primary goals of students: seeking attention, gaining power, seeking revenge for a perceived injustice, or avoiding failure.
2.3 Bullying—a special kind of aggression
Bullying is aggressive, harmful behavior that involves intentional and repetitive actions in which an individual who holds a position of power targets someone who is (perceived) less powerful [18]. An essential characteristic of this type of aggression is the imbalance of power on which it is based. Bullying perpetration describes aggression against someone [19, 20], while peer victimization refers to the subject of aggressive or abusive behavior.
Allowing oneself to be bullied is a form of passive acceptance, whereas bullying involves aggressive behavior to achieve one’s goals. Passive and aggressive predispositions have genetic determinants, being connected with a person’s temperament. However, they are also learned through cultural values, societal norms, gender role expectations, family dynamics, and parenting styles. Assertiveness is a learned approach to communication, conflict resolution, and goal attainment that emphasizes balance [21].
There are different types of bullying perpetration: physical, verbal, or relational [22], either direct (overt) or indirect (covert) aggression [23], or, more recently, online bullying by using electronic means (cyberbullying, cyber harassment) [24, 25].
Frequently, the most common presupposition is that the bullies/perpetrators come from adverse life experiences (neglect and abuse), with a difficult upbringing in hostile or rejecting family environments, resulting in poorly developed self-concept, negative, self-denigrating beliefs, and negative beliefs and attitudes about others. Inflicted prosocial skills and possibly underdeveloped communication and problem-solving skills negatively impact the ability to interact and communicate efficiently with the surrounding environments [26]. Some explanatory theories connect bullying perpetration with insecure attachment [27], learned aggressiveness [28, 29], or weak social bonds [30].
Bullying perpetrators do not seem to have low self-esteem [31], except for female perpetrators [32, 33]. However, some findings suggest that bullying perpetrators usually have lower self-esteem than children without behavioral problems [34]. Positive correlations were found between low self-esteem and peer victimization [35].
These characteristics and variables explain most children’s aggressive predispositions and actions, but not all bullying actions. Bullying is based on unbalanced power between the abuser and the victim. One or more unflattering or undesired traits of the victim become the subject and the motive for the repetitive, intentional attack. Bullying relies on discrimination. This explains, in part, the attitudes and actions of the rest of the crowd: the followers and henchmen, the supportive and the passive audience.
The bully gains popularity, support, admiration, and power when the witness agrees and allies with him or chooses not to intervene.
Many factors contribute to aggressive behavior in children, but not all cases of bullying can be explained by these variables. Bullying occurs when the perpetrator and victim have an unequal power dynamic. The bully repeatedly targets their victim based on one or more undesirable traits. Discrimination plays a role in bullying, and this can influence the attitudes and actions of bystanders. The bully gains social status and power when others support or fail to intervene in their behavior.
Research indicates that boys’ physical aggression is more prevalent [36, 37], whereas girls tend to engage in relational aggression [38]. Verbal aggression, on the other hand, appears to be equally used by both genders [39].
Bullying increases progressively during childhood, peaks in early adolescence, and declines in late adolescence [40]. However, this abusive pattern of behavior might continue into adulthood (abusive couple relationships, bullying and mobbing at the workplace).
Fluck [41] sustains that the taxonomies of the bullying phenomenon are essential for two reasons: the rationale for operationalizing the construct and the building of a solid foundation for further, more elaborated research on the matter. We want to add a third important reason for the relevance and necessity of the bullying taxonomies: the intervention. Only conceptualizing, identifying, and clarifying the motives and the functions of the aggressive behavior/bullying (especially from the abuser’s point of view) permits the identification of efficient arguments for change (both mindset through cognitive restructuring and, subsequently, behavioral modification through contingencies’ manipulations), and maintains the determinations to adhere to new, alternative, and socially acceptable ways of attaining the objectives/satisfying the functions of the initial behaviors [42].
3. The diagnostic level: conceptual models of aggressive behaviors
3.1 The cognitive model
Cognitive theories focus on the mental processes that enable us to perceive, name, categorize, and understand our world and assist us in problem-solving.
The basic principle in cognitive psychology is that people react differently, emotionally and behaviorally, to the events they go through due to their cognitive schemas (a hierarchical structure of core beliefs, rules, assumptions, and attitudes). These cognitive schemas develop progressively during childhood and adolescence, are structured and influenced by internalized cultural norms and values and each person’s life experiences. We are the survivors of our life history.
According to the cognitive paradigm [7, 43], an uncertain or stressful situation activates a particular system of beliefs, leading to a specific behavioral reaction. The perceived stimuli are then evaluated by assessing and interpreting the situation, resulting in an automatic thought or cognition. This thought generates an emotional state that triggers physiological reactions, leading to a specific behavioral response (Figure 1).
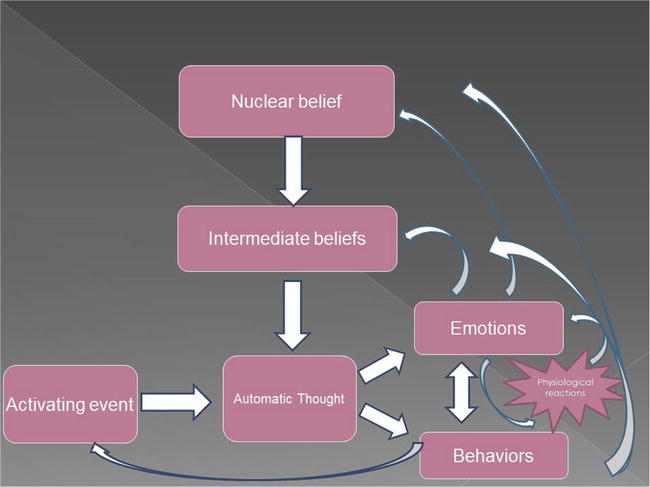
Figure 1.
The cognitive model of reaction to an activating event.
Our beliefs (core, intermediate, and, hence, subsequent automatic thoughts) are formed through our childhood and adolescent experiences. These beliefs help us assess and categorize situations and react accordingly, allowing us to adapt to our environment.
However, certain circumstances exist where an individual’s core beliefs, which are the most fundamental, can become irrational, rigid, and overgeneralized. These circumstances may include unique neurophysiological structures and functions, challenging upbringing conditions, or extreme and traumatic experiences. The structuration of these beliefs can involve cognitive distortions, resulting in inflexible and rigid emotional and behavioral responses to activating events. Consequently, such rigid ways of interpreting and thinking about life events can lead to undesirable behavioral patterns.
It is crucial to recognize how individuals perceive and interpret specific actions or events (known as automatic thoughts), as they can reveal fundamental beliefs, rules, assumptions, and attitudes that influence emotional and behavioral responses.
These cognitive schemes constitute a personal lens and perceptive prism of events. The particular perception generates a personal interpretation of the meaning of the perceived events (automatic thought); this interpretation depends on the emotional and behavioral reactions of the person.
Our cognitive schemes shape how we see and understand the world around us. They act like a lens through which we interpret events and generate automatic thoughts. This interpretation results from our unique personal perception, and the meaning assumed from what we perceive influences our emotional and behavioral reactions.
Emotional and behavioral issues are often caused by cognitive inflexibility and poorly structured irrational beliefs resulting from cognitive distortions.
Erikson [44] extends this approach and considers behavioral and emotional problems as the expression of identity crises, of inadequate solutions/responses to a series of existential dilemmas.
Jones [9] presents a theory of child development, marked by turning points and demands experienced by the child as developmental anxieties. She believes five general types of developmental anxieties involve complex interpersonal and intrapersonal processes from birth through adolescence. Themes of these developmental anxieties are abandonment, inadequacy, guilt, conflict, and personal identity. Identifying children’s developmental anxieties provides a more explicit framework for understanding their behavioral responses in borderline, stressful situations [9].
Personal experiences causing stress can significantly impact the formation, structure, and function of various structures within the central nervous system. Trauma and abuse, in particular, can be sources of harmful stress.
When an individual experiences toxic stress, whether acute or continuous, it can result in the survival brain (which includes the hypothalamus and amygdala) being in a perpetual state of activation. This can cause the emotional brain to overwork, triggering the body’s stress reactions of fight, flight, or freeze. As a result, the person develops a hyperalert pattern of brain functioning and body reaction, constantly perceiving the world as threatening and dangerous.
The particular modality in which an individual’s beliefs are organized may significantly affect their responses in particular situations. In interrelations and communication, both parties (person 1 and person 2) come with personal systems of beliefs, values, rules, and attitudes. Person 1’s behavior (the manifest and visible part of his or her thought-emotion-behavior path) becomes an activating event for the communication partner (Figure 2). The reaction (response) of the receiving partner (person 2) will depend on his mindset (system of beliefs).
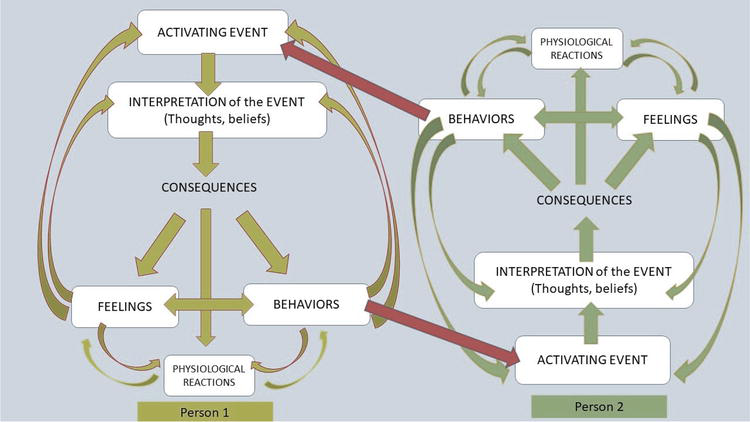
Figure 2.
A cognitive model of communication.
When beliefs become irrational and inflexible, it can lead to the formation of dysfunctional perspectives. This creates a rigid pattern of emotional and behavioral reactions that are difficult to adapt to different contexts, situations, or people/relationships. This inflexibility can harm an individual’s ability to adapt and function socially.
Understanding that this condition does not simply disappear as the child ages is essential. Their irrational beliefs and dysfunctional view of reality can persist into adulthood, potentially leading to disharmonious personality structures that have a pervasive impact on their life.
3.2 The conceptual model of the conflict—LSCI
The Life Space Crisis Intervention (LSCI) is an advanced therapeutic method that combines multiple theories, such as psychoanalytic, behavioral, cognitive, and practical, to identify repeating behavioral patterns in young individuals that hinder their personal development. This approach relies on theoretical and empirical data. It utilizes the Conflict Cycle model as its primary tool to illustrate how conflict communication is triggered and maintained, leading to a crisis [8, 9].
The Conflict Cycle sheds light on how the responses of others, such as adults and peers, can play a role in the escalation of conflicts (Figure 3). As in the cognitive model, one’s behavior is an event perceived and interpreted by the dialog partner according to his system of beliefs. The reaction will depend on this interpretation. When the reaction is immature and impulsive, mirroring the other’s aggressive behaviors, for example (anger generates counter-anger and aggression fuels counter-aggression), the conflictual communication evolves from an activating event to a critical incident. Eventually, it might escalate into a crisis (Figure 3). Reacting to negative actions rationally can help individuals regulate their emotions and impulses. This may result in less tension, displaying appropriate behavior and eventually putting an end to confrontational exchanges.
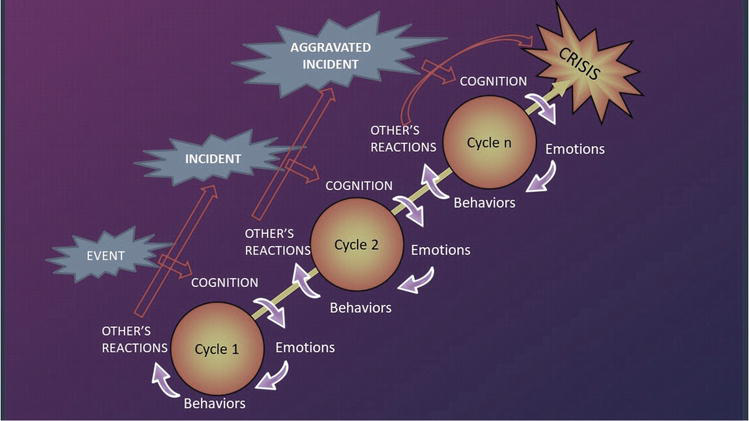
Figure 3.
The escalation of conflictual communication (the LSCI model).
Research has shown that uncontrolled emotions, particularly anger, can elicit a similar response in others, resulting in a cycle of aggression and retaliation [8]. This can escalate into a crisis as tension builds up [9]. This model can be applied in different environments, such as homes, schools, or workplaces, to identify the underlying problem and provide effective conflict resolution strategies.
The Reality Check Intervention is intended for children who may tend to misinterpret situations, be socially isolated, or make excuses to justify their actions. This program aims to provide a realistic perspective on life and help children overcome their challenges. These children may present symptoms of autism spectrum disorders, social (pragmatic) communication disorders, Attention Deficit/Hyperactivity Disorder (ADHD), low social and communication skills, and impulsivity.
The Red Flag Intervention concept illustrates how humans often use displacement as a defense mechanism. This means that when children experience distress, anger, pain, or frustration, they may discharge them toward someone who is not the actual cause of their feelings. The person who becomes the target of the outburst may be unrelated to past experiences and perceived as less threatening and available in a more secure context. This behavior can offer perpetrator relief, catharsis, and stress release, with fewer negative consequences. The main manifestations of these children are impulsivity and pain-based behaviors.
The Benign Confrontation Intervention is designed for children who have egocentric tendencies and believe they have the right to say or do anything to defend themselves or prove their superiority. They may often justify their actions and blame others, feeling emotionally detached from the victim and dismissing the impact of their behavior [9]. These behavior characteristics evoke behavioral disorders (oppositional defiant disorder and conduct disorder) and might develop into an antisocial personality disorder.
The Regulate and Restore Intervention is designed for children presenting self-abusive behaviors and self-denigrating comments. Usually, as victims of emotional, physical, and sexual abuse, they are overwhelmed by feelings of shame, unworthiness, inadequacy, and guilt and tend to have significant difficulties regulating their emotions and controlling their behaviors. The symptoms suggest emotional disorders, such as anxiety and depression, and bipolar personality disorders, converging to borderline personality disorders.
The New Tools Intervention is used for children presenting reduced (social) skills. They usually appear to have good intentions but lack the appropriate, socially accepted behaviors to pursue them. Usually, children with intellectual impairment, socio-emotional and communication immaturity, ADHD, autism spectrum disorders, and social (pragmatic) communication disorders access this inefficient behavioral pattern.
The final intervention, the Peer Manipulation Intervention, aims to expose problematic, unbalanced peer relations, either in false friendship (the manipulator and manipulated pairs) or in the form of set-up (the manipulator provoking a well-known impulsive and aggressive colleague). These dysfunctional relationships might occur due to the unhealthy and unfortunate meeting between children with externalized disorders (conduct disorder, oppositional defiant disorder) and children with internalized disorders (anxiety, depression, and bipolar personality disorder).
All these self-defeating behavioral patterns might determine, in particular situations, aggressive reactions, but their goals, cognitions, and emotions are quite different.
These patterns of self-defeating behaviors are interchangeable: a victim might become a bully, and a bully might find himself a victim in other circumstances and contexts. Bully behavior, like any other behavior, can be modeled and learned.
Prone to bully behaviors are children who appreciate the efficiency of this behavior in gaining and satisfying personal needs (attention/admiration/status, power, or revenge), and begin to justify it and detach emotionally from the victim.
The motives of followers reside in fear of association with the victim (when they could suffer the same treatment) or in need for appreciation and higher status (given to them if associated with the “popular” guy/girl or through reconnaissance of this popular guy if they obey him).
Based on the unequal power relationship assumption, bullying intentionally manipulates and exploits a victim’s feelings and actions. While other patterns of inappropriate behavior might be explained mainly through specific cognitive or emotional determinants, bullying is based on social interaction and the need for one bully to control and push the emotional buttons of the victim to control his behavior.
In LSCI, the most illustrative pattern of bullying is Peer Manipulation. That is because bullying is based on an unequal power relationship. Peer Manipulation can take several forms. One of them is false friendship or frenemies.
In this pattern, we have a vulnerable child seeking appreciation and validation and a manipulative peer willing to fulfill those needs as long as the child acts as a puppet for him. In this unequal relationship, the manipulator persuades the vulnerable peer to misbehave. The manipulator’s power resides in the victim’s desperate need for affiliation and friendship, poor self-concept and self-confidence, fear of losing “the friend,” and possible prestige and protection offered by this association. Usually, the manipulation act remains undetected and unreported, as the vulnerable child is trapped in this relationship and willing to pay for not losing it. The intervention should focus on clarifying the characteristics of a true friend, exposing the imbalance in the relationship, and developing the vulnerable child’s assertiveness.
Another form of peer manipulation is The Set Up, a pattern that involves a vulnerable emotional child and a brilliant and passive-aggressive manipulator. The set-up works as the manipulator creates scenarios that reinforce the vulnerabilities of his peer and then triggers violent action by constantly pushing him to act. The bully has the satisfaction of manipulating the victim’s emotions and actions. In this scenario, the aim is to teach the vulnerable child how to identify when his emotions are played and to learn to control his reactions.
Finally, the most aggressive pattern of peer manipulation is The Mastermind. This pattern is based on a power play in which the aggressive child manipulates others to demonstrate that he can do it for fun and his satisfaction. In this case, the intervention aims are common with benign confrontations and are addressed to the bully. We must build a secure relationship, openly confront the behaviors, and explore alternatives.
Although the sympathy and preoccupation go quickly and somehow naturally to the victim and the immediate interventions are addressed to her, we should stress the necessity of equally approaching the bully. First, just criticizing and punishing the misbehaviors of the bully do not change his mindset, beliefs, and attitudes. Thus, no fundamental, profound, sustainable behavioral and attitudinal changes will exist. More, these punishment-based interventions might confirm some irrational beliefs and reinforce misbehaviors. Second, the irrational beliefs sustaining misbehaviors might be rooted in personal pain and grief that must be acknowledged and addressed therapeutically.
4. The prescriptive and prognostic levels: implications for intervention
The cognitive paradigm works on the cognition-emotion-behavior model, explaining the differences in human reactions to the same stimuli through the differences in the cognitive system of beliefs. When considering modifying unhelpful behavioral patterns and strategies, an essential technique is cognitive restructuring. This means we must identify the underlying core beliefs and their potential cognitive distortions and expose, confront, and test them using cognitive techniques or behavioral experiments. Therapeutic intervention could also focus on behavioral modification (through contingencies manipulations) or emotion regulation. Any modification of one of these terms of the equation (thought, emotion, behavior) will trigger a change in the other two.
Our actions and behaviors are driven by the need to achieve our goals. Acknowledging these needs and prioritizing their fulfillment, especially as they play a significant role in our personal growth, is essential. It is crucial to identify their underlying motivations to understand their behaviors better and make effective interventions. Aggressive behavior, for instance, is a means of achieving a goal and should be addressed by educators and therapists by replacing it with more socially acceptable alternatives. Behaviors serve different functions, some of which are adaptive, reflective of our past experiences, and help us navigate different situations.
When someone experiences emotional and behavioral disorders, their undesirable behaviors may be a way to cope with their feelings and maintain a sense of predictability and control over situations. These behaviors serve as experiments to test their beliefs and fulfill them. Engaging in these actions, children may provoke unpleasant events to confirm their expectations of adverse outcomes. Unfortunately, this cycle reinforces harmful behaviors and confirms irrational beliefs.
We begin helping the student by challenging their expectations. We can distinguish between different diagnoses by accurately identifying the purpose of their negative behavior in the diagnostic process. For example, aggressive behavior may stem from fear, shame, inadequacy, anger, or pride [17]. The cause of aggression can be attributed to a specific way of perceiving things, personal beliefs, and emotional responses. Through assessment, we can determine the triggers and outcomes of the behavior and establish its intended purpose. The assessment result should provide a clear description of the behavior’s characteristics.
In education or therapy, relying solely on observable behavior characteristics for intervention methods can be ineffective or even detrimental. It could reinforce negative behaviors, intensify negative emotions, and confirm irrational beliefs, leading to a self-fulfilling prophecy. The LSCI theory suggests that unprepared adults may react to disruptive behavior with inappropriate emotional and behavioral responses, such as counter-anger and retaliation, leading to a cycle of conflict.
According to Brendtro [9] and Tobias & Chapanar [45], a successful intervention should uncover the underlying purpose of behavior and address the hidden needs rather than just reacting to the problematic behavior itself.
The LSCI method offers six intervention strategies that address self-destructive behaviors frequently seen in school and family environments. These behaviors could be a sign of emotional or behavioral disorders, both internalized and externalized, and are customized to suit specific emotional and behavioral reactions to stressful circumstances. It is a comprehensive approach to helping individuals overcome such patterns [9].
Being a crisis-designed strategy, the LSCI method begins with the de-escalation stage. This stage (Drain off) responds to the emotional outburst/meltdown demands when the emotional brain (hypothalamus and amygdala) overwrites the rational brain (neocortex), and intense emotions control the reactions. The objective of this stage is to offer time and space for the person to calm down gradually as the stress hormones dissipate and the cortex regains control, expressed through restored rational thinking and superior psychological processing (e.g., language). In this stage, we allow the children to relieve stress and drain off the powerful emotions that hinder their irrational approach to the situation. Our goal is the de-escalation of emotion, creating a supportive relationship in a safe environment.
The following two diagnostic stages of the LSCI, like in the cognitive paradigm intervention, clarify the client’s perspective and recollection of the event, identify the personal perceptive, thinking, and emotional and behavioral reactions (the Timeline stage), identify the main self-defeating behavioral pattern, and differentiate between transitory/circumstantial or habitual (patterns) responses (the Central Problem stage).
The second stage also helps to clarify the specific triggers, maintaining factors, and aggravating factors of the target behavior. We need to understand the event from the child’s perspective. In this step, we encourage the child to express his understanding of the situation in a structured mode, allowing us to draw a timeline of events. Our goal in this stage is to understand the event from the child’s point of view. By assessing the student’s perception of the event, their feelings, and their reaction before, during, and after the event, we can identify the function of the behavior.
The third stage of the diagnostic phase (the Central Issue stage) concludes the diagnostic phase of the intervention. At this point, we try to identify the central issue: the specific pattern of self-defeating behavior. Although most behaviors could usually be framed in one of the six patterns described earlier in this chapter, there are always particularities of the situation and specific traits we must consider. We can make assumptions about the appropriate intervention and possible outcomes based on the identified patterns. The final goal is to assess whether the behavior fits a specific pattern and decide what intervention to employ.
The three diagnostic stages aim to facilitate an insightful understanding of the problem by the client, acknowledging the pattern used in coping with stressful content (the Insight stage), a guided process of finding new solving solutions (the New Tools stage), and implementation of these solutions in life space contexts (the Transfer of Learning stage).
The intervention phase has three stages: Insight stage, New Tools, and Transfer of Learning stage.
The Insight stage is the core of the intervention, as we try to help the children to gain a new understanding of the event and his/her behavior, including the consequences. This step is crucial for a successful intervention because it is the base for the child’s intrinsic motivation for relevant and sustainable behavioral change, as he primarily acknowledges its benefits for himself. Our goal for this step is to guide the child into understanding the self-defeating effects of his current behavior and how the suggested change could improve his function and probability of success.
The New Tools stage is a learning process of new, acceptable, and efficient ways to respond positively to future stressful events. We aim to guide the child in a problem-solving approach to identify, practice, apply, and assess alternative reactions. This step promotes communication and social abilities’ development.
The Transfer of Learning stage advocates and supports the attempts to implement and practice the newly achieved skills in similar future situations. Our goal is to prepare the children to return to their ecological environment and to assist them in practicing and improving the new, socially accepted, and efficient solving strategies.
The LSCIs follow the steps mentioned above in specific ways according to specific behavioral patterns. The first three steps (the diagnostic phase) are identical, but the other three are tailored to each type of identified behavioral pattern.
5. Conclusions
Understanding the function of a person’s behavior is vital for the assessment, diagnosis, and intervention process. It helps to identify how he or she copes with threatening or stressful situations. When conceptualizing an undesirable behavior, it is essential to consider its antecedents, triggers, description, and consequences. This conceptualization should come from an unbiased interview with the client and be refined with additional information. Ultimately, the evaluation should aim to identify the function and goal of the behavior—what purpose does it serve? Even if two behaviors appear similar, their functions may be entirely different.
It is crucial to identify the function of a person’s behavior to correctly diagnose and distinguish between different disorders or patterns of self-defeating behavior with similar symptoms. The intervention decisions and techniques should be based on a thorough assessment, or they may be ineffective or harmful, making inappropriate behavior worse. Understanding the behavior’s purpose will also help select the most effective therapeutic approach and technique. Intervention strategies and techniques should acknowledge the behavior’s identified function and focus on teaching alternative, socially acceptable behaviors that fulfill that function. Therefore, a successful intervention should be tailored to the individual’s circumstances and needs at every stage, from conceptualization to strategy selection.
References
- 1.
Perry B. Applying principles of neurodevelopment to clinical work with maltreated and traumatized children. The neurosequential model of therapeutics. In: Webb B, editor. Working with Youth in Child Welfare. New York: The Guilford Press; 2006 - 2.
Ramirez J. Human Aggression—A Multifaceted Phenomenon. Madrid: UCM Centreur; 2003 - 3.
Nietzel M, Hasemann D, Lynam, D. Behavioral perspective on violent behavior. In: Van Hasselt V, Hersen M. editors. Handbook of Psychological Approaches with Violent Offenders: Contemporary Strategies and Issues. New York: Kluwer Academic/Plenum Press; 1999. - 4.
Bandura A. Social Learning Theory. Englewood Cliffs: Prentice-Hall; 1977 - 5.
Bandura A. Social Foundations of Thought and Action: A Social-Cognitive Theory. Englewood Cliffs: Prentice-Hall; 1986 - 6.
Stoff D, Susman E. Developmental Psychobiology of Aggression. Cambridge: Cambridge University Press; 2005 - 7.
Cognitive BJ, Therapy B. Basics and Beyond. New York: The Guilford Press; 2011 - 8.
Long N, Fecser F, Morse W, Newman R, Long J. Conflict in the Classroom. Austin: Pro-Ed; 2014 - 9.
Long N, Wood M, Fecser F, Whitson S. Taking with Students in Conflict. Life Space Crisis Intervention. Austin: PRO.ED, Inc.; 2021 - 10.
Tremblay R, Hartup W, Archer J. Developmental Origins of Aggression. New York: The Guilford Press; 2005 - 11.
Maslow A. Motivation and Personality. New York: Harper; 1954 - 12.
Max-Neef M. Human scale development. In: Conception, Application and Further Reflections. New York: The Apex Press; 1991 - 13.
Brendtro L, Brokenleg M, Van Bockern S. The circle of courage and positive psychology. Reclaiming Children and Youth. 2005; 14 (3):130-136 - 14.
Adler A. What Life Should Mean to You. New York: Capricorn; 1958 - 15.
Dreikurs R, Loren G. A New Approach to Discipline: Logical Consequences. New York: Hawthorn Books; 1968 - 16.
Nelsen J, Lott L, Glenn S. Positive Discipline in the Classroom. 3rd ed. Rocklin: Prirna Publishing; 2000 - 17.
Darjan I, Predescu M, Tomita M. Functions of aggressive behaviors – Implications for intervention. Journal of Psychological and Educational Research. 2017; 25 (1):74-91 - 18.
Olweus D. Bullying among schoolchildren: Intervention and prevention. In: Peters R, McMahon R, Quinsey P, editors. Aggression and Violence Throughout the Life Span. Newbury Park: Sage; 1992. pp. 100-125 - 19.
Chen J, Wei H. The impact of school violence on self-esteem and depression among Taiwanese junior high school students. Social Indicators Research. 2011; 100 :479-498 - 20.
Gendron B, Williams R, Guerra G. An analysis of bullying among students within schools: Estimating the effects of individual normative beliefs, self-esteem, and school climate. Journal of School Violence. 2011; 10 :150-164 - 21.
Dârjan I, Negru M, Ilie D. Self-esteem – The decisive difference between bullying and assertiveness in adolescence? Journal of Educational Sciences. 2020, 2020; 1 (41):19-34. DOI: 10.35923/JES.2020.1.02 - 22.
Crick N, Bigbee M. Relational and overt forms of peer victimization: A multi-informant approach. Journal of Consulting and Clinical Psychology. 1998; 66 :337-347 - 23.
Drennan J, Brown R, Mort S. Phone bullying: Impact on self-esteem and well-being. Young Consumers. 2011; 12 :295-309 - 24.
Hinduja S, Patchin J. Bullying Beyond the Schoolyard: Preventing and Responding to Cyberbullying. Thousand Oaks: Sage Publications; 2009 - 25.
Valkenburg P, Peter J, Schouten A. Friend networking sites and their relationship to adolescents’ well-being and social self-esteem. Cyberpsychology & Behavior. 2006; 9 (5):584-590 - 26.
Cook C, Williams K, Guerra N. Predictors of bullying and victimization in childhood and adolescence: A meta-analytic investigation. School Psychology Quarterly. 2010; 25 :65-83 - 27.
Murphy T, Laible D, Augustine M. The influences of parent and peer attachment on bullying. Journal of Child and Family Studies. 2017; 26 (5):1388-1397. DOI: 10.1007/s10826-017-0663-2 - 28.
Aslan S. The analysis of the relationship between school bullying perceived parenting styles and self-esteem in adolescents. Procedia - Social and Behavioral Sciences. 2011; 30 :1798-1800. DOI: 10.1016/j.sbspro.2011.10.346 - 29.
Baldry A. Bullying in schools and exposure to domestic violence. Child Abuse & Neglect. 2003; 27 :713-732. DOI: 10.1016/s0145-2134(03)00114-5 - 30.
Chan H, Chui W. Social bonds and school bullying: A study of Macanese male adolescents on bullying perpetration and peer victimization. Child & Youth Care Forum. 2013; 42 :599-616. DOI: 10.1007/s10566-013-9221-2 - 31.
Pearce J, Thompson A. Practical approaches to reduce the impact of bullying. Archives of Disease Childhood. 1998; 79 :528-531. DOI: 10.1136/adc.79.6.528 - 32.
Rigby K, Cox I. The contribution of bullying at school and low self-esteem to acts of delinquency among Australian teenagers. Personality and Individual Differences. 1996; 21 :609-612. DOI: 10.1016/0191-8869(96)00105-5 - 33.
Slee P. Peer victimization and its relationship to depression among Australian primary school students. Personality and Individual Differences. 1995; 18 :57-62. DOI: 10.1016/0191-8869(94)00114-8 - 34.
O’Moore M, Kirkham C. Self-esteem and its relationship to bullying behavior. Aggressive Behavior. 2001; 27 :269-283. DOI: 10.1002/ab.1010 - 35.
Fredstrom B, Adams E, Gilman R. Electronic and school-based victimization: Unique contexts for adjustment difficulties during adolescence. Journal of Youth and Adolescence. 2011; 40 :405-415. DOI: 10.1007/s10964-010-9569-7 - 36.
Rosen N, Nofziger S. Boys, bullying, and gender roles: How hegemonic masculinity shapes bullying behavior. Gender Issues. 2019; 36 :295-318. DOI: 10.1007/s12147-018-9226-0 - 37.
Ploeg R, Steglich C, Veenstra R. The way bullying works: How new ties facilitate the mutual reinforcement of status and bullying in elementary schools. Social Networks. 2020; 60 :71-82. DOI: 10.1016/j.socnet.2018.12.006 - 38.
Eriksen I, Lyng S. Relational aggression among boys: Blind spots and hidden dramas. Gender and Education. 2018; 30 (3):396-409. DOI: 10.1080/09540253.2016.1214691 - 39.
Fares E, Ramirez J, Cabrera M, Lozano F, Salas F. Justification of physical and verbal aggression in Uruguayan children and adolescents. The Open Psychology Journal. 2011; 4 :45-54 - 40.
Nansel T, Overpeck M, Pilla R, Ruan W, Simons-Morton B, Scheidt P. Bullying behaviors among U.S. youth: Prevalence and association with psychosocial adjustment. Journal of the American Medical Association. 2001; 285 :2094-2100. DOI: 10.1001/jama.285.16.2094 - 41.
Fluck J. Why do students bully? An analysis of motives behind violence in schools. Youth & Society. 2014; 49 :1-21. DOI: 10.1177/0044118X14547876 Available from:http://yas.sagepub.com/content/early/2014/08/28/0044118X14547876 - 42.
Alstot A, Alstot C. Behavior management: Examining the functions of behavior. Journal of Physical Education, Recreation & Dance. 2015; 86 (2):22-28. DOI: 10.1080/07303084.2014.988373 - 43.
Ellis A. Reason and Emotion in Psychotherapy. New York: Lyle Stuart; 1962 - 44.
Erikson E, Joan M. The Life Cycle Completed: Extended Version. New York: W. W. Norton; 1997 - 45.
Tobias S, Chapanar T. Predicting resilience after cyberbully victimization among high school students. Journal of Psychological and Educational Research. 2016; 24 (1):7-25. Available from:http://www.marianjournals.com/files/JPER_articles/JPER_24_1_2016/Tobias_Chapanar_JPER_2016_24_1_7_25.pdf