Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
End stage kidney disease contributes to a huge burden on global health. Recent advances have shown that ischemic and hypoxic conditions may contribute to the progression of the disorder and that acute kidney injury may cause and aggravate the condition. Ischemia and hypoxia are two distinct conditions with different pathophysiological and structural consequences as proven in the brain and liver of rats. Until now, these differences have not been shown to exist in the kidney. In this study, we assess the possible functional differences in the outcome of ischemic and hypoxic stress on the kidney. For this purpose, we perfused isolated rabbit kidneys with their autologous blood and applied short periods of ischemia or hypoxia in separate series of experiments. The results showed that the kidneys exposed to hypoxic stress suffered more functional damage than those subjected to ischemia. This conclusion was based on a lower creatinine clearance and urine osmolality, and a higher fractional excretion of urea, sodium, and glucose in the hypoxia series of kidneys. Consequently, we recommend monitoring hypoxemic conditions closely and correcting the condition as soon as possible, since even for a short period it may already have deteriorating effects on the renal function.
Faculty of Medicine, Department of Physiology, Anton de Kom University of Suriname, Paramaribo, Suriname
Paul Steels
Faculty of Medicine, Department of Physiology, University of Hasselt, Hasselt, Belgium
Jerry Toelsie
Faculty of Medicine, Department of Physiology, Anton de Kom University of Suriname, Paramaribo, Suriname
*Address all correspondence to: robbert.bipat@uvs.edu
1. Introduction
1.1 Ischemia or hypoxia
Ischemia and hypoxia play major roles in the pathophysiology of important diseases and conditions like stroke [1], cardiovascular disease [2], and even Alzheimer’s dementia [3], but also in therapeutic procedures like the survival of organ transplants [4, 5]. Survival of organ transplants as well as patients depends on the proper function of the graft [6], while for some procedures like renal transplantation, there is an inherent period of sustained ischemia and hypoxia [7, 8].
Traditionally the terms ischemia and hypoxia are mixed and often used without any distinction between these two entities [3, 9, 10, 11, 12, 13]. This assumption is probably based on the common molecular reactions observed in ischemia as well as hypoxia [14]. Investigators, however, have found clear distinctions in the pathophysiological consequences of these entities. For instance, a study on rats showed that experimental ischemia of the brains led to necrosis of the neurons while this consequence was absent under hypoxic conditions, even at a low perfusion pressure of 30 mmHg [15]. Another study showed that the veno-arterial difference of PCO2 was far less under hypoxic conditions compared to ischemia in the hindlimb of dogs [16], and consequently implies that ischemia and hypoxia may follow different mechanisms of disease. In this chapter ischemia is defined as a sudden decrease in perfusion pressure of the kidney, while hypoxia is defined as a reduction in partial oxygen pressure in the blood with intact perfusion [17, 18].
In addition to the pathologic conditions mentioned above, hypoxia also plays a role in the physiological regulation of physiological processes. For instance, the process of angiogenesis is triggered by hypoxic conditions in the absence of a total ischemic shutdown of the vessels [10]. Hypoxia also plays a role in the differentiation of stem cells [19, 20]. Furthermore, the condition is involved in wound healing [21] and it is believed that mild hypoxia promotes vessel growth in the placenta during pregnancy [22].
Conditions involving hypoxia, but not ischemia include, for instance, moderate to severe anemia and diseases that limit the gas exchange in the lungs. Anemia leads to hypoxic conditions in the tissues of organs that are prone to an already low oxygen pressure under physiological conditions. These are, for example, the epithelial lining of the gut [23] and the medullary vasa recta in the kidneys [24]. Recent findings, however, demonstrate that both structural and functional changes occur because of anemia leading to hypoxia in tissues that are normally abundantly oxygenated [25]. Furthermore, tumors are especially susceptible to hypoxia in anemic states [26].
Apart from anemia, conditions that limit the diffusing capacity in the pulmonary alveoli will also lead to hypoxic conditions in other organs and tissues. For instance, hypoxic hepatitis can be the result of respiratory or cardiac failure with respiratory failure being responsible for 13–20% of the cases [27]. One of the important contributing factors to the damage seen in this disorder of the liver is hypoxemia [28]. The condition was formerly more known as “shock liver” and the change in nomenclature highlights the role that hypoxia plays in its pathophysiology [28].
Recently we saw more hypoxemic conditions with the advent of the SARS-2 COVID 19 pandemic. Even without clear signs, patients suffering from this infection show mild to moderate hypoxemia [29]. Furthermore, in the absence of direct damage caused by the virus, pathologic conditions observed in the heart, liver, and kidneys in severe conditions of this infection hint toward the involvement of hypoxic conditions in these organs [30, 31, 32, 33]. Recently studies described the possible effect of air pollution on the development of chronic kidney disease [34]. The cause is probably the presence of specific particulate matter in the air, but it remains to be determined if a low atmospheric oxygen content may also contribute to this [35].
1.2 Kidney disease and hypoxia
The global prevalence of chronic kidney disease was estimated between 9 and 14% of the population, and the number of patients who needed kidney replacement therapy exceeded 5 million in 2017 [36, 37]. With an annual individual cost of up to 40,000 Euro [38], this easily amounts to at least 200 billion Euro and is one of the most challenging public health concerns. The main causes of chronic kidney disease are diabetes and hypertension [39]. Furthermore, acute kidney injury plays a key role in the etiology and progress of the disease [40]. For both the acute and the chronic phases of the disease, hypoxia of the medullary environment plays a role in both the initial cause and then the progression to chronic and end-stage renal disease [41, 42, 43, 44]. The hypoxia may be the result of ischemic disease [45], nephrotoxic damage of the renal interstitial space [43, 46], or from disturbances not related to the kidney [31].
1.3 Isolated perfused kidneys
The kidney is a very intricate organ with highly coordinated activity. The experimental investigation of renal function must be separated from extrarenal and potential intrarenal regulatory mechanisms due to the interdependence of organs [47, 48]. Studies in vivo are frequently hampered by contemporaneous changes in blood pressure, circulating fluid volume, CO2 and O2 tensions, or neurogenic and hormonal reactions to experimental stimuli [48]. For these reasons, it is very convenient to study the function of the kidney under healthy and pathological circumstances in isolated perfused preparations of the organ. There are various methods to isolate and perfuse kidneys.
The idea to artificially perfuse organs originated in the 18th century when Le Gallois thought of a substitute for the heart to maintain any part of the body indefinitely [49], first attempts to perfuse isolated organs were not made until the 19th century by Löbell [50]. With the introduction of the isolated perfused rat kidney in 1959, the era of isolated perfused kidneys started [51] and in the following years, kidneys of various animals like dogs, rabbits, pigs, sheep, monkeys and even human kidneys have been isolated and perfused [52]. Studies concentrated on the physiology, pathophysiology, and pharmacology of renal function [53, 54, 55, 56].
In the past 60 years, it has become clear that the function of the isolated perfused kidneys depends largely on the choice of perfusate. This varies between a completely artificial physiological buffer to autologous blood. All studies have shown that the best physiological results were achieved from preparations perfused with any kind of perfusates that contained red blood cells, preferably autologous blood [48]. Organs perfused with a low content of red blood cells always show moderate to severe degrees of necrosis in the medullary part of the kidneys [57]. For these reasons, we developed an isolated rabbit kidney model that was perfused with autologous blood [58].
1.4 Aim of the study
In this study we applied short-term ischemic and hypoxic conditions to isolated rabbit kidneys perfused with autologous blood. The goal of this was to determine whether there is a difference in effects with these two conditions since this will affect the way we think about their pathophysiologic mechanisms and possible management of these conditions in the clinical setting. Isolated kidneys perfused with blood already show structural and functional defects in the organ at 7–25 minutes of warm ischemia [59]. Consequently, we limited the ischemia and hypoxia time to 25 minutes, to keep the possibility of fast recovery of the organ after reperfusion and reoxygenation. This allowed us to establish possible functional differences between these two kinds of interventions since previous studies showed that the isolated organ worked perfectly for about 2–3 hours [58].
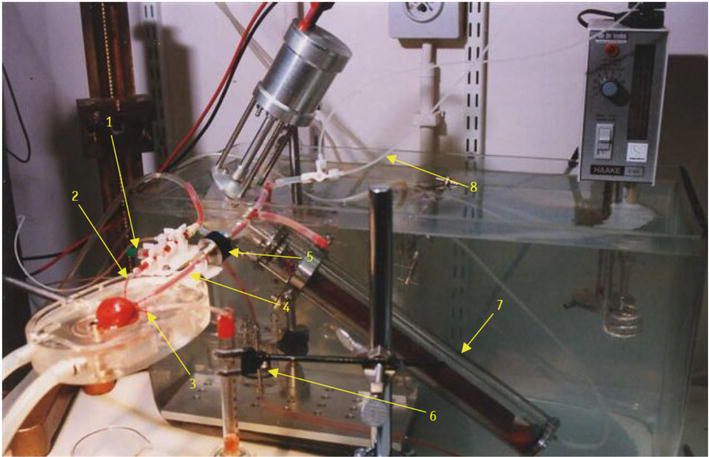
The surgery and perfusion were carried out exactly as described by Cuypers and coworkers [48, 58]. Briefly, rabbits weighing 3–4 kg had their left kidneys removed under ketamine anesthesia (3–10 mg/kg body weight), and the kidney was then perfused with a modest volume (25 ml) of the same animal’s heparinized blood in a closed circuit with a pump and an oxygenator. Warm oil was dripped over the kidney surface while the entire circulatory system was kept in a bath with temperature control set at 38°C. A PowerLab 4E analog-digital converter (AD Instruments) was used to constantly monitor and record perfusion pressure (Gould Statham pressure transducer: P23 ID) and renal blood flow (RBF; Skalar Transflow 600 System, extracorporeal probe, internal diameter 3 mm). The pumping system was set to maintain the perfusion pressure at 100 mm Hg. The oxygenator was perfused with a gas mixture of either 96% O2 and 4% CO2 under normal conditions or 96% N2 and 4% CO2 to create a hypoxic condition at a perfusion rate of 300 mL/min. Figure 1 gives an overview of this setup.
Figure 1.
The experimental setup. 1. Arterial sampling site, 2. Arterial line, 3. Ureter, 4. Venous line, 5. Flow sensor, 6. Pulsating pump in warm water bath, 7. Oxygenator in water bath, 8. Infusion lines. Taken from [48] with permission.
2.2 Perfusion and renal function
A ureteral catheter was used to collect urine. Continuous infusion (0.1 ml/min) was administered throughout the perfusion to make up for urine excretion. The infusion solution’s composition (in mM) was as follows: 35 mM NaCl, 40 mM KCl, 7.3 mM creatinine, 133 mM urea, 3.4 mM NaH2PO4, 13.6 mM Na2HPO4, 22.6 mM NaHCO3, 10 mM glutamine, and 55 mM glucose. Additionally, it had 30 IU/l of [Arg8]-vasopressin (AVP; Sigma). Additional NaCl (145–290 mM) was administered to make up for the extra urine output and osmolyte loss when urine flow (UF) surpassed 0.1 ml/min. All infusion was stopped when urine flow was zero. The hematocrit was maintained at 32–33% by replacing any blood loss through sampling and hemorrhage with an equivalent volume of whole blood. The kidneys were given at least 25 minutes to recover after the perfusion was established. After the first recovery, there were four 30-min perfusion sessions (P1–P4) during which urine was taken. At the conclusion of each period, blood samples were obtained. As a baseline, the data entered in P1 were used.
2.3 Experimental procedures
In the first series of experiments (n = 5), the perfusion of the kidney was shut down with a direct bypass of the arterial line to the venous line during the second period (P2). In P3 the perfusion was restored. The reason for keeping the blood in circulation was to prevent stagnation, which would lead to the formation of thrombotic and vasoconstrictive factors [60]. In the second series of studies (n = 5), the oxygenator’s oxygen supply was stopped at the end of P1 and replaced with nitrogen (96 percent N2, 4 percent CO2), which was provided during P2 (25–30 min). This caused a drop in mean arterial blood PO2 from 144 ± 36 to 11 ± 3 mm Hg (n = 5, with SD). The perfusion pressure was kept at 100 mmHg and the flow rate of gas through the oxygenator at 300 mL/min. In P3 and P4 the perfusion and oxygenation were restored (Figure 2).
Figure 2.
Protocol of experiments.
2.4 Animals and chemicals
The highest-grade chemicals were used throughout, and they were all acquired from Sigma Belgium. White adult rabbits were housed in the university’s animal facility. All institutional ethical norms and procedures were followed when handling animals.
2.5 Analyses and calculations
A Beckman Synchron Clinical System CX3 was used to perform Na+, K+, urea, and creatinine analyses on plasma and urine samples. A Knauer-Halb micro-osmometer was used to measure the osmolality of the plasma and urine. To assess the glomerular filtration rate, creatinine clearance (CCr) was computed as CCr = (UCr UF)/PCr, where UCr and PCr stand for the creatinine concentrations in the urine and plasma, respectively (GFR). With the use of a Chiron Diagnostics 238 pH/blood gas analyzer, pH, PCO2, and PO2 were measured (Bayer) [58].
2.6 Statistics
The data are presented as median with interquartile range and were evaluated using Student’s T-test to compare the two series, and the Brown-Forsythe ANOVA test, followed by Dunnett’s T3 multiple comparisons test to compare values within the series. Differences were deemed significant at p < 0.05.
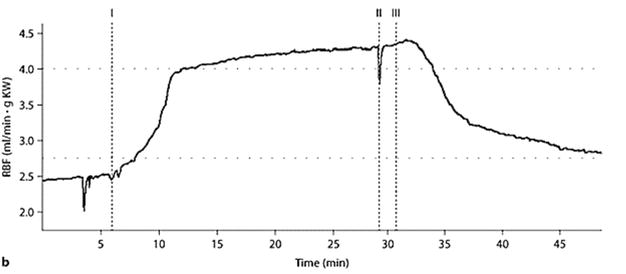
The RBF increased during hypoxia in P2, but returned to the lower value in P3 and P4. Figure 3 is a representative trace of this flow. After reperfusion, The RBF recovered in P3 and P4 in the ischemia series. The urine flow stopped in both series during the interventions in P2. In P3 and P4 it recovered in both series, but in the hypoxia series, there was a significantly higher urine flow compared to P1. The lack of urine flow in the P2 did not allow us to determine the rest of the parameters in this period. In both series the creatinine clearance (CCr) decreased in P3 and P4, but at a much lower value in the hypoxia series, despite a comparable increase of urine flow.
Figure 3.
Renal blood flow during hypoxia in an individual experiment. I: Start hypoxia, II: Sampling of blood, III: Reoxygenation (taken from [61] under a creative commons attribution non-commercial-No-Derivs 3.0 license. The full article is available at https://www.karger.com/article/FullText/333478).
Urine osmolality decreased after both interventions but was significantly lower in the hypoxia series. The absolute urea excretion was significantly lower in the hypoxia series after reoxygenation and recovered in P4. In P3 and P4, the fractional excretion of urea was however higher in both series. The fractional excretion of sodium increased significantly higher after reoxygenation. Furthermore, the plasma potassium value was significantly higher in P3 after reoxygenation but decreased in P4 closer to the control value in P1. Finally, we found that the plasma glucose decreased significantly after reoxygenation and compared with the ischemia series, and in addition the fractional excretion of glucose was significantly higher after reoxygenation.
In the present study we investigated the effects of two conditions, ischemia and hypoxia, on isolated rabbit kidneys perfused with autologous blood. Both these conditions led to acute renal failure, reflected by a significant decrease in creatinine clearance, increase of plasma urea, and decrease of urine osmolality in the presence of AVP, after reperfusion and reoxygenation, respectively. In addition, the decline in function was already observed after a short 30-minute intervention.
4.1 Renal blood flow, urine flow, and creatinine clearance
The increased renal blood flow during hypoxia is surprising since previous studies showed that hypoxemia leads to increased vascular resistance in the kidneys. Subjects who received donor kidneys had a higher vascular resistance under hypoxemic conditions, while the resistance was much lower with hyperoxia in the allograft [62]. Older studies concluded that reperfusion after ischemic injury resulted in a reduction of renal blood flow of up to 50% after reperfusion, a phenomenon called “no-reflow” [63, 64, 65]. The lower flow was not only the result of vasoconstriction but also suggestively an entrapment of red blood cells [66]. A recent study also reported a sustained lower renal blood flow in experimental ischemia in in vivo experiments conducted on rats [67]. We do not have any plausible explanation for the absence of significant vasoconstriction after ischemia and even the presence of vasodilatation during hypoxemia and after reoxygenation in our experiments. It may be due to the fact that the isolated organ is not under influence of other systemic influences after ischemia-reperfusion. Support for this can be found in the fact that with hypoxemia there is a generalized vasodilatation with resulting decreased perfusion pressure and renal blood flow. This induces vasoconstriction as a compensatory mechanism and is probably mediated by the renin-angiotensin aldosterone system [68]. Obviously, these mechanisms are not involved in our model.
The cessation of urine flow and consequently the creatinine clearance during ischemia is clearly the result of the absence of any perfusion pressure. However, this phenomenon is also observed during hypoxia. In previous reports, we showed that the absence of urine flow is possibly the result of a generalized swelling of oxygen-dependent cells. We found that the intratubular hydrostatic pressure increased during the hypoxic phase but remained at the control level when the infusion included mannitol. In these experiments, in the presence of mannitol, urine flow, and creatinine clearance remained reasonably good and were perhaps not due to the diuretic effect since furosemide did not produce this improvement [61, 69]. The high renal blood flow and the absence of vasoconstriction after reoxygenation argues against structural changes in the vessels.
4.2 Urine osmolality and urea excretion
The urine osmolality was significantly lower after both reperfusion and reoxygenation, but significantly less after the latter. Generally, acute renal failure is associated with lower urine osmolality values [70]. Here we observed a significantly lower urine osmolality in the case of hypoxia, to almost the plasma osmolality. This difference cannot be explained simply by the lack of energy in the thick ascending limb of the loop of Henle, since this should be the case in both experimental conditions. It is more plausible that with intact and higher blood flow in case of hypoxia, the necessary solutes for concentrating the urine are washed out in the medulla of the organ. The relatively low blood flow in the renal medulla under physiological conditions is absolutely necessary for the maintenance of this solute gradient [71]. The accompanying hypoxia will only worsen the concentrating capacity in this case [71].
We observed that the absolute excretion of urea was initially lower with hypoxia but recovered in the last period. Previous results showed that urea is necessary for the maximum concentrating capacity of these isolated perfused kidneys [72]. What we observed in the present study is that the absolute excretion of urea recovered quickly despite a very low creatinine clearance. Consequently, the fractional excretion (FEUrea) is significantly higher compared to controls, and this is more pronounced in the hypoxia series. In fact, one study suggested that a higher FEUrea is more closely associated with tubular necrosis and that a lower FEUrea reflects the possibility of prerenal failure [73]. Our findings are in line with these latter two outcomes, and this adds more evidence that the damage is more prominent in the hypoxia series compared to the ischemia series. Moreover, it was found that the FEUrea was significantly higher in persistent acute renal failure compared to the transient form that lasted up to 3 days in patients and that this parameter hence is useful as a marker for the seriousness of the condition [74]. The FEUrea can be calculated with a simple formula in a clinical setting, without determination of the GFR 1.
4.3 Sodium and potassium
Similar to the fractional excretion of urea, that of sodium (FENa) was also significantly higher in the hypoxia series compared to the ischemia after reoxygenation and reperfusion. Since the reabsorption of sodium is ATP dependent, this could mean that the high fractional excretion in the presence of sufficient energy after reoxygenation, there are already widespread functional problems after the short period of oxygen deprivation [75]. On the other hand, we also observe a high plasma potassium (PK) immediately after reoxygenation, which is immediately resolved in the last period of perfusion in the absence of a high K excretion. This means that the abundance of potassium was probably caused by exit from the intracellular space in the hypoxic state but re-entered the cells after oxygen supply was restored [61].
4.4 Glucose
The lower plasma glucose in the hypoxia series may be explained by the high energy demand to restore the intracellular potassium content as explained in the previous section [76]. In addition, it indicates that there are enough remaining cells to keep the metabolism ongoing. Furthermore, it may reflect a high utilization of glucose and ongoing glycolysis during the deprivation of oxygen. Indeed one study showed a tight coupling of the sodium-potassium ATPase to glycolysis in rat cardiomyocytes [77]. We also observed a higher fractional excretion of glucose after hypoxia compared to ischemia, which indicates that the hypoxic stress also interfered with the proximal tubule function [78]. All these factors may explain the worse outcome of renal function during hypoxia compared to the ischemic state.
4.5 Clinical and therapeutic implications
The results of this study show that there is a functional difference between the outcome in conditions characterized by compromised perfusion of the kidney and a situation with intact circulation but with a low oxygen content of the blood. The outcome of the latter is worse with respect to renal functional parameters like creatinine clearance, urine osmolality, fractional excretion of urea, sodium and glucose, and escape of potassium from the intracellular space. Examples of clinical conditions accompanied by a low oxygen content in the blood are severe anemia [79], compromised diffusion of oxygen in the lungs as we have seen in COVID-19 cases [31, 80], and cardiopulmonary bypass procedures [81]. The present results accentuate that it is of paramount importance to preserve the oxygen supply to the kidneys, to prevent worsening of the organ’s function in circulatory compromised situations or procedures. It is, therefore, important to monitor hemoglobin level and oxygen saturation in patients at risk, since hypoxemia may sometimes be present without clinical signs [80, 82]. In addition, we have shown that even a short period of hypoxemia may already cause functional damage to the kidney. This should be a reason to recommend that the monitoring and treatment of the hypoxemia conditions should be more vigilant [83]. Who knows, maybe there is such a condition as pulmo-renal syndrome similar to hepatorenal syndrome?
There is a clear distinction in the pathophysiological consequences of ischemia and hypoxia. In this study, we showed thathypoxemia without compromise of the circulation has a significantly worse outcome for renal function, even when present for only a short time of 30 minutes. Acute kidney disease or injury can evolve into chronic disorders or may worsen an already chronic situation. We, therefore, recommend that possible hypoxic states must be monitored closely and corrected adequately in conditions accompanied by an inherent circulatory or oxygen content deficiency.
We are indebted to Prof Dr. Yves Cuypers, who passed away in 2018. He taught us the technique of perfusing isolated kidneys with blood. Our gratitude also involves Wilfried Leyssens who passed away in 2015. They both participated in the design of and assisted to conduct the study presented here.
“The authors declare no conflict of interest.” The study was carried out with funds available from the university.
References
1.Nour M, Scalzo F, Liebeskind DS. Ischemia-reperfusion injury in stroke. Interventional Neurology. 2012;1:185-199. DOI: 10.1159/000353125
2.Semenza GL. Hypoxia-inducible factor 1 and cardiovascular disease. Annual Review of Physiology. 2014;76:39. DOI: 10.1146/annurev-physiol-021113-170322
3.Salminen A, Kauppinen A, Kaarniranta K. Hypoxia/ischemia activate processing of amyloid precursor protein: Impact of vascular dysfunction in the pathogenesis of Alzheimer’s disease. Journal of Neurochemistry. 2017;140:536-549. DOI: 10.1111/JNC.13932
4.Zhao H, Alam A, Soo AP, George AJT, Ma D. Ischemia-reperfusion injury reduces long term renal graft survival: Mechanism and beyond. eBioMedicine. 2018;28:31-42. DOI: 10.1016/j.ebiom.2018.01.025
5.Fernández AR, Sánchez-Tarjuelo R, Cravedi P, Ochando J, López-Hoyos M. Review: Ischemia reperfusion injury—A translational perspective in organ transplantation. International Journal of Molecular Sciences. 2020;21:8549. DOI: 10.3390/IJMS21228549
6.Yarlagadda SG, Coca SG, Formica RN, Poggio ED, Parikh CR. Association between delayed graft function and allograft and patient survival: A systematic review and meta-analysis. Nephrology Dialysis Transplantation. 2009;24:1039-1047. DOI: 10.1093/NDT/GFN667
7.Perico N, Cattaneo D, Sayegh MH, Remuzzi G. Delayed graft function in kidney transplantation. Lancet. 2004;364:1814-1827. DOI: 10.1016/S0140-6736(04)17406-0
8.Rosenberger C, Eckardt KU. Oxygenation of the transplanted kidney. Seminars in Nephrology. 2019;39:554-566. DOI: 10.1016/j.semnephrol.2019.10.005
9.Northington FJ, Chavez-Valdez R, Martin LJ. Neuronal cell death in neonatal hypoxia-ischemia. Annals of Neurology. 2011;69:743-758. DOI: 10.1002/ana.22419
10.Semenza GL. Vascular responses to hypoxia and ischemia. Arteriosclerosis, Thrombosis, and Vascular Biology. 2010;30:648-652. DOI: 10.1161/atvbaha.108.181644
11.Jiang M, Liu K, Luo J, Dong Z. Autophagy is a Renoprotective mechanism during in vitro hypoxia and in vivo ischemia-reperfusion injury. The American Journal of Pathology. 2010;176:1181-1192. DOI: 10.2353/AJPATH.2010.090594
12.Douglas-Escobar M, Weiss MD. Biomarkers of hypoxic-ischemic encephalopathy in newborns. Frontiers in Neurology. 2012;3:144. DOI: 10.3389/
13.Malek M, Nematbakhsh M. Renal ischemia/reperfusion injury; from pathophysiology to treatment. Journal of Renal Injury Prevention. 2015;4:20. DOI: 10.12861/jrip.2015.06
14.Rosenberger C, Mandriota S, Jürgensen JS, Wiesener MS, Hörstrup JH, Frei U, et al. Expression of hypoxia-inducible factor-1α and -2α in hypoxic and ischemic rat kidneys. Journal of the American Society of Nephrology. 2002;13:1721-1732. DOI: 10.1097/01.asn.0000017223.49823.2a
15.Miyamoto O, Auer RN. Hypoxia, hyperoxia, ischemia, and brain necrosis. Neurology. 2000;54:362-362. DOI: 10.1212/wnl.54.2.362
16.Vallet B, Teboul JL, Cain S, Curtis S. Venoarterial CO2 difference during regional ischemic or hypoxic hypoxia. Journal of Applied Physiology. 2000;89:1317-1321. DOI: 10.1152/jappl.2000.89.4.1317
17.Brezis M, Rosen S, Silva P, Epstein FH. Renal ischemia: A new perspective. Kidney International. 1984;26:375-383. DOI: 10.1038/ki.1984.185
18.Abuelo JG. Normotensive ischemic acute renal failure. New England Journal of Medicine. 2007;357:797-805. DOI: 10.1056/NEJMra064398
19.Hawkins KE, Sharp TV, Mckay TR. The role of hypoxia in stem cell potency and differentiation. 2013;8:771-782. DOI: 10.2217/rme.13.71
20.Abdollahi H, Harris LJ, Zhang P, McIlhenny S, Srinivas V, Tulenko T, et al. The role of hypoxia in stem cell differentiation and therapeutics. Journal of Surgical Research. 2011;165:112-117. DOI: 10.1016/J.JSS.2009.09.057
21.Hong WX, Hu MS, Esquivel M, Liang GY, Rennert RC, McArdle A, et al. The role of hypoxia-inducible factor in wound healing. 2014;3:390-399. Available from: https://homeliebertpubcom/wound. DOI: 10.1089/wound.2013.0520
22.Stangret A, Skoda M, Wnuk A, Pyzlak M, Szukiewicz D. Mild anemia during pregnancy upregulates placental vascularity development. Medical Hypotheses. 2017;102:37-40. DOI: 10.1016/j.mehy.2017.03.007
23.Arthur CM, Nalbant D, Feldman HA, Saeedi BJ, Matthews J, Robinson BS, et al. Anemia induces gut inflammation and injury in an animal model of preterm infants. Transfusion (Paris). 2019;59:1233-1245. DOI: 10.1111/TRF.15254
24.Evans RG, Smith DW, Lee CJ, Ngo JP, Gardiner BS. What makes the kidney susceptible to hypoxia? The Anatomical Record. 2020;303:2544-2552. DOI: 10.1002/AR.24260
25.Cahill LS, Gazdzinski LM, Tsui AK, Zhou YQ , Portnoy S, Liu E, et al. Functional and anatomical evidence of cerebral tissue hypoxia in young sickle cell anemia mice. Journal of Cerebral Blood Flow and Metabolism. 2017;37:994-1005. DOI: 10.1177/0271678x16649194/asset/images/large/10.1177_0271678x16649194-fig 2.jpeg
26.Wilson MJ, van Haaren M, Harlaar JJ, Park HC, Bonjer HJ, Jeekel J, et al. Long-term prognostic value of preoperative anemia in patients with colorectal cancer: A systematic review and meta-analysis. Surgical Oncology. 2017;26:96-104. DOI: 10.1016/j.suronc.2017.01.005
27.Henrion J. Hypoxic hepatitis. Liver International. 2012;32:1039-1052. DOI: 10.1111/J.1478-3231.2011.02655.X
28.Waseem N, Chen PH. Hypoxic hepatitis: A review and clinical update. Journal of Clinical and Translational Hepatology. 2016;4:263. DOI: 10.14218/JCTH.2016.00022
29.Fuglebjerg NJU, Jensen TO, Hoyer N, Ryrsø CK, Madsen BL, Harboe ZB. Silent hypoxia in patients with SARS CoV-2 infection before hospital discharge. International Journal of Infectious Diseases. 2020;99:100-101. DOI: 10.1016/J.IJID.2020.07.014
30.Li J, Fan JG. Characteristics and mechanism of liver injury in 2019 coronavirus disease. Journal of Clinical and Translational Hepatology. 2020;8:13. DOI: 10.14218/JCTH.2020.00019
31.Ahmadian E, Hosseiniyan Khatibi SM, Razi Soofiyani S, Abediazar S, Shoja MM, Ardalan M, et al. Covid-19 and kidney injury: Pathophysiology and molecular mechanisms. Reviews in Medical Virology. 2021;31:e2176. DOI: 10.1002/RMV.2176
32.Chong WH, Saha BK. Relationship between severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and the Etiology of acute kidney injury (AKI). The American Journal of the Medical Sciences. 2021;361:287-296. DOI: 10.1016/J.AMJMS.2020.10.025
33.Khalil S, Collins A, Mubarak N, Khalil T. Third degree heart block and elevated troponin following acute respiratory hypoxic failure in a COVID-19 recovered patient in the absence of coronary artery disease. Journal of Cardiology Case Reports. 2020;4:1-3
34.Tsai HJ, Wu PY, Huang JC, Chen SC. Environmental pollution and chronic kidney disease. International Journal of Medical Sciences. 2021;18:1121. DOI: 10.7150/IJMS.51594
35.Al-Aly Z, Bowe B. Air pollution and kidney disease. Clinical Journal of the American Society of Nephrology. 2020;15:301. DOI: 10.2215/CJN.16031219
36.Cockwell P, Fisher LA. The global burden of chronic kidney disease. The Lancet. 2020;395:662-664. DOI: 10.1016/S0140-6736(19)32977-0
37.Lv JC, Zhang LX. Prevalence and disease burden of chronic kidney disease. In: Liu B-C, Lan H-Y, Lv L-L, editors. Renal Fibrosis: Mechanisms and Therapies. Vol. 1165. New York LLC: Springer; 2019. pp. 3-15. DOI: 10.1007/978-981-13-8871-2_1/COVER
38.Sánchez-Escuredo A, Alsina A, Diekmann F, Revuelta I, Esforzado N, Ricart MJ, et al. Economic analysis of the treatment of end-stage renal disease treatment: Living-donor kidney transplantation versus Hemodialysis. Transplantation Proceedings. 2015;47:30-33. DOI: 10.1016/J.TRANSPROCEED.2014.12.005
39.Levey AS, Coresh J. Chronic kidney disease. The Lancet. 2012;379:165-180. DOI: 10.1016/S0140-6736(11)60178-5
40.Venkatachalam MA, Griffin KA, Lan R, Geng H, Saikumar P, Bidani AK. Acute kidney injury: A springboard for progression in chronic kidney disease. American Journal of Physiology. Renal Physiology. 2010;298:1078-1094. DOI: 10.1152/ajprenal.00017.2010/asset/images/large/zh20051058870007.jpeg
41.Ullah MM, Basile DP. Role of renal hypoxia in the progression from acute kidney injury to chronic kidney disease. Seminars in Nephrology. 2019;39:567-580. DOI: 10.1016/j.semnephrol.2019.10.006
42.Nangaku M. Hypoxia and Tubulointerstitial injury: A final common pathway to end-stage renal failure. Nephron Experimental Nephrology. 2004;98:e8-e12. DOI: 10.1159/000079927
43.Heyman SN, Khamaisi M, Zorbavel D, Rosen S, Abassi Z. Role of hypoxia in renal failure caused by Nephrotoxins and hypertonic solutions. Seminars in Nephrology. 2019;39:530-542. DOI: 10.1016/j.semnephrol.2019.10.003
44.Fu Q , Colgan SP, Shelley CS. Hypoxia: The force that drives chronic kidney disease. Clinical Medicine & Research. 2016;14:15-39. DOI: 10.3121/cmr.2015.1282
45.Textor SC, Lerman LO. The role of hypoxia in ischemic chronic kidney disease. Seminars in Nephrology. 2019;39:589-598. DOI: 10.1016/J.SEMNEPHROL.2019.10.008
46.Li ZL, Liu BC. Hypoxia and renal Tubulointerstitial fibrosis. Advances in Experimental Medicine and Biology. 2019;1165:467-485. DOI: 10.1007/978-981-13-8871-2_23/COVER
47.Gong R, Dworkin LD. Brenner and Rector’s the Kidney. Philadelphia: Saunders Elsevier; 2008
48.Bipat R. Renal function-study performed on an isolated rabbit kidney perfused with autologous blood [thesis] University of Hasselt. 2004
49.Le Gallois MJJC. Experiments on the principle of life, and particularly on the principle of the motions of the heart, and on the seat of this principle…. Experiments on the Principle of Life, and Particularly on the Principle of the Motions of the Heart, and on the Seat of This Principle… 2012. DOI: 10.1037/13894-000.
50.Hierholzer K, Ullrich KJ. History of renal physiology in Germany during the 19th century. American Journal of Nephrology. 1999;19:243-256. DOI: 10.1159/000013458
51.Weiss C, Passow H, Rothstein A. Autoregulation of flow in isolated rat kidney in the absence of red cells. 1959;196:1115-1118. DOI: 10.1152/ajplegacy.1959.196.5.1115
52.Nizet A. The isolated perfused kidney: Possibilities, limitations and results. Kidney International. 1975;7:1-11. DOI: 10.1038/KI.1975.1
53.Marques AAM, da Silva CHF, de Souza P, de Almeida CLB, Cechinel-Filho V, Lourenço ELB, et al. Nitric oxide and Ca2+−activated high-conductance K+ channels mediate nothofagin-induced endothelium-dependent vasodilation in the perfused rat kidney. Chemico-Biological Interactions. 2020;327:109182
54.Pool MBF, Vos J, Eijken M, van Pel M, Reinders MEJ, Ploeg RJ, et al. Treating ischemically damaged porcine kidneys with human bone marrow-and adipose tissue-derived mesenchymal stromal cells during ex vivo normothermic machine perfusion. Stem Cells and Development. 2020;29:1320-1330
55.Huijink TM, Venema LH, Posma RA, de Vries NJ, Westerkamp AC, Ottens PJ, et al. Metformin preconditioning and postconditioning to reduce ischemia reperfusion injury in an isolated ex vivo rat and porcine kidney normothermic machine perfusion model. Clinical and Translational Science. 2021;14:222-230
56.Pool MBF, Hartveld L, Leuvenink HGD, Moers C. Normothermic machine perfusion of ischaemically damaged porcine kidneys with autologous, allogeneic porcine and human red blood cells. PLoS One. 2020;15:e0229566
57.Lieberthal W, Stephens GW, Wolf EF, Rennke HG, Vasilevsky ML, Valeri CR, et al. Effect of erythrocytes on the function and morphology of the isolated perfused rat kidney. Kidney & Blood Pressure Research. 1987;10:14-24. DOI: 10.1159/000173109
58.Cuypers Y, Vandenreyt I, Bipat R, Toelsie J, Van Damme B, Steels P. The functional state of the isolated rabbit kidney perfused with autologous blood. Pflügers Archiv. 2000;440:634-642. DOI: 10.1007/s004240000320
59.Harper SJF, Hosgood SA, Waller HL, Yang B, Kay MD, Goncalves I, et al. The effect of warm ischemic time on renal function and injury in the isolated hemoperfused kidney. Transplantation. 2008;86:445-451. DOI: 10.1097/tp.0b013e31817fe0cd
60.Nizet A, Cuypers Y, Deetjen P, Kramer K. Functional capacity of the isolated perfused dog kidney. Pflügers Archiv für die Gesamte Physiologie des Menschen und der Tiere. 1967;296:179-195. DOI: 10.1007/BF00363758
61.Bipat R, Steels P, Cuypers Y, Toelsie JR. Mannitol reduces the hydrostatic pressure in the proximal tubule of the isolated blood-perfused rabbit kidney during hypoxic stress and improves its function. Nephron Extra. 2011;1:201-211. DOI: 10.1159/000333478
62.Sharkey RA, Mulloy EMT, O’Neill SJ. Acute effects of hypoxaemia, hyperoxaemia and hypercapnia on renal blood flow in normal and renal transplant subjects. European Respiratory Journal. 1998;12:653-657. DOI: 10.1183/09031936.98.12030653
63.Thiel G, Rougemont D de, Kriz W, Mason J, Torhorst J, Wolgast M. The role of reduced medullary perfusion in the genesis of acute ischemic renal failure. Nephron 1982;31:321-323. DOI: 10.1159/000182674.
64.Mason J, Torhorst J, Welsch J. Role of the medullary perfusion defect in the pathogenesis of ischemic renal failure. Kidney International. 1984;26:283-293. DOI: 10.1038/KI.1984.171
65.Johnston WH, Latta H. Glomerular mesangial and endothelial cell swelling following temporary renal ischemia and its role in the no-reflow phenomenon. The American Journal of Pathology. 1977;89:153
66.Hellberg POA, Kallskog O, Wolgast M. Red cell trapping and postischemic renal blood flow. Differences between the cortex, outer and inner medulla. Kidney International. 1991;40:625-631. DOI: 10.1038/KI.1991.254
67.Freitas F, Attwell D. Pericyte-mediated constriction of renal capillaries evokes no-reflow and kidney injury following ischaemia. eLife. Cardiology Case Reports. 2020;4:1-26 DOI: 10.7554/elife.74211
68.Huet F, Semama DS, Gouyon JB, Guignard JP. Protective effect of Perindoprilat in the hypoxemia-induced renal dysfunction in the Newborn rabbit. Pediatric Research. 1999;45:138-142. DOI: 10.1203/00006450-199901000-00023
69.Bipat R, Toelsie J, Steels P, Cuypers Y. Mannitol in contrast to furosemide, reduces tubular obstruction and improves renal function during and after hypoxic stress in the isolated rabbit kidney perfused with autologous blood. Abstract presented in the form of a poster at the meeting of the ‘Belgian Society for Fundamental and Clinical Physiology and Pharmacology’, Brussels (Belgium) 17th of November 2001
70.Bagshaw SM, Langenberg C, Wan L, May CN, Bellomo R. A systematic review of urinary findings in experimental septic acute renal failure. Critical Care Medicine. 2007;35:1592-1598. DOI: 10.1097/01.CCM.0000266684.17500.2F
71.Brezis M, Rosen S. Hypoxia of the renal medulla—Its implications for disease. New England Journal of Medicine. 1995;332:647-655
72.Steels P, Toelsie J, Cuypers Y, Bipat R. Urea is important for the urinary concentration capacity of the isolated blood perfused rabbit kidney. In: ASN Renal Week 2010, Denver. Journal of the American Society of Nephrology. 2010;21:484A
73.Carvounis CP, Nisar S, Guro-Razuman S. Significance of the fractional excretion of urea in the differential diagnosis of acute renal failure. Kidney International. 2002;62:2223-2229. DOI: 10.1046/J.1523-1755.2002.00683.X
74.Dewitte A, Biais M, Petit L, Cochard JF, Hilbert G, Combe C, et al. Fractional excretion of urea as a diagnostic index in acute kidney injury in intensive care patients. Journal of Critical Care. 2012;27:505-510. DOI: 10.1016/J.JCRC.2012.02.018
75.Steiner RW. Interpreting the fractional excretion of sodium. The American Journal of Medicine. 1984;77:699-702. DOI: 10.1016/0002-9343(84)90368-1
76.Pirahanchi Y, Jessu R, Aeddula NR. Physiology, Sodium Potassium Pump. Treasure Island (FL), USA: StatPearls; 2022
77.Sepp M, Sokolova N, Jugai S, Mandel M, Peterson P, Vendelin M. Tight coupling of Na+/K+-ATPase with glycolysis demonstrated in Permeabilized rat Cardiomyocytes. PLoS One. 2014;9:e99413. DOI: 10.1371/journal.pone.0099413
78.Bishop JH, Green R, Thomas S. Free-flow reabsorption of glucose, sodium, osmoles and water in rat proximal convoluted tubule. The Journal of Physiology. 1979;288:331-351. DOI: 10.1113/jphysiol.1979.sp012698
79.Greenburg AG. Pathophysiology of anemia. The American Journal of Medicine. 1996;101:7S-11S. DOI: 10.1016/S0002-9343(96)00161-1
80.Nouri-Vaskeh M, Sharifi A, Khalili N, Zand R, Sharifi A. Dyspneic and non-dyspneic (silent) hypoxemia in COVID-19: Possible neurological mechanism. Clinical Neurology and Neurosurgery. 2020;198:106217. DOI: 10.1016/J.CLINEURO.2020.106217
81.Lankadeva YR, Cochrane AD, Marino B, Iguchi N, Hood SG, Bellomo R, et al. Strategies that improve renal medullary oxygenation during experimental cardiopulmonary bypass may mitigate postoperative acute kidney injury. Kidney International. 2019;95:1338-1346. DOI: 10.1016/J.KINT.2019.01.032
82.Swenson KE, Ruoss SJ, Swenson ER. The pathophysiology and dangers of silent hypoxemia in COVID-19 lung injury. Annals of the American Thoracic Society. 2021;18:1098-1105. DOI: 10.1513/annalsats.202011-1376cme/suppl_file/disclosures.pdf
83.Shenoy N, Luchtel R, Gulani P. Considerations for target oxygen saturation in COVID-19 patients: Are we under-shooting? BMC Medicine. 2020;18:1-6. DOI: 10.1186/S12916-020-01735-2/FIGURES/1