Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
To purchase hard copies of this book, please contact the representative in India:
CBS Publishers & Distributors Pvt. Ltd.
www.cbspd.com
|
customercare@cbspd.com
The anti-atherogenic, anti-inflammatory, and vasomotor effects of statins on the arteries are well known, but there are no significant literature data about statins treatment effects on veins. This study describes the potential morphological changes that may occur in the venous wall in the case of the patients with chronic venous disease (CVD) which associates atorvastatin treatment for at least two years. The patients were clinically evaluated, and at the same time, a microscopic morphological analysis was performed on surgically removed veins fragments. The obtained results prove an improvement in the CVD prognosis, as well as a better postoperative evolution in these patients, and suggest an improvement in the blood flow in the vasa vasorum from the venous adventitia, as well as a potential phlebotonic and phlebotrophic effect of statins.
Abdominal Surgery and Phlebology Research Center, “Victor Babeș” University of Medicine and Pharmacy Timișoara, Timișoara, Romania
1st Surgical Clinic, “Pius Brînzeu” Emergency County Hospital, Timișoara, Romania
*Address all correspondence to: matei.sergiu@umft.ro
1. Introduction
Chronic venous disease (CVD) is a prevalent condition with global spread, affecting about a quarter of the adult population, significantly influencing the quality of life of these patients. The prevalence of CVD is highest in Western countries. More recent epidemiological studies of venous diseases in which the CEAP classification was used show a prevalence of 60–70% CEAP clinical class C0 and C1, about 25% for C2 and C3, and up to 5% for C4 to C6 with skin changes or venous ulcers. A recently published comprehensive systematic review on global epidemiology of CVD including >300,000 adults showed that the pooled prevalence of C2 disease is increasing. C2 disease had a progression rate of 22% developing a venous leg ulcer in six years. The incidence of varicose veins is approximately 2% per year [1, 2, 3]. At the same time, the incidence of cardio-metabolic diseases is worldwide increasing because of an increase in the standard of living [4], and in many cases, these diseases are associated with varicose veins of the lower limbs due to common risk factors such as obesity, sedentary lifestyle or inadequate nutrition [5].
Dyslipidemia is defined by the presence of nonoptimal levels of blood lipids, and it is a common risk factor for cardiovascular diseases. In clinical practice guidelines, dyslipidemia is mostly defined by elevated total cholesterol and/or low-density lipoprotein cholesterol, but the definition is also often extended to include nonoptimal levels of high-density lipoprotein cholesterol, triglyceride, apolipoprotein B, and apolipoprotein A1. Because dyslipidemia is one the most important modifiable risk factors for cardiovascular diseases [6], treatment is frequently indicated as primary prevention, even at an early age, statins being currently the most commonly prescribed drug worldwide for lowering serum cholesterol [7].
The beneficial effects of statins on clinical events may involve nonlipid mechanisms that modify endothelial function, smooth muscle cells, and monocyte–macrophage: vasomotor function, inflammatory responses, and plaque stability. Augmented bioactivity of nitric oxide by statins therapy either indirectly by its effect on lipoprotein levels and protection of LDL from oxidation, or directly by effects on nitric oxide synthesis and release, might account for enhancement of endothelium-dependent vasodilation. Recent experimental and animal studies have demonstrated that statins dose-dependently decrease smooth muscle cells migration and proliferation, independently of their ability to reduce plasma cholesterol. Moreover, statins are able to reduce the in vitro cholesterol accumulation in macrophages and expression of matrix metalloproteinase, resulting in plaque stability. These effects of statins were completely prevented by the addition of mevalonate and partially by all-trans farnesol and all-trans geranylgeraniol, confirming the specific role of isoprenoid metabolites, probably through prenylated proteins, in regulating these cellular events. Statins have been shown to prevent the activation of monocytes into macrophages, inhibit the production of pro-inflammatory cytokines, C-reactive protein, and cellular adhesion molecules. Statins decrease the adhesion of monocyte to endothelial cells. Accordingly, statins exert their cardiovascular benefits through a direct antiatherogenic properties in the arterial wall, beyond their effects on plasma lipids [8].
The anti-atherogenic, anti-inflammatory, and vasomotor functions of statins on the arterial wall are well known [8, 9], and despite the fact that the pleiotropic effects of statins have been documented for over 20 years [10], only a few studies debate the advantages of statins in healing venous leg ulcers, and there are no studies documenting how statins act on the venous wall morphology, and particularly in patients diagnosed with CVD.
This paper represents a sequel of a previous study [11] regarding the impact of statin medication in the case of the phlebological patient and the morphological changes that may occur in the venous wall in this case, debating additionally the clinical evolutions of those patients and the clinical implications of these observations.
A series of morpho-anatomical parameters for a study group and a control group, which analyzed patients with CVD, were compared in the initial study. Those parameters included age (years), BMI (kg/m2), lumen (thrombosed/free), maximum venous diameter (cm)—it took into account the maximum diameter at the level of the vein of the largest caliber from the surgically excluded specimens, for each patient—venous wall thickness (cm); thickening of TI; thickening of TM; disorganized muscle bundles in TM; fragmentation of elastic fibers in TM; collagen increased in TA; absence of vasa vasorum in TA. This research study was a retrospective one.
A number of inclusion criteria were common for both groups, as follows: CVD, C2–C3 CEAP stage; an average period of 60 +/− 4 months from the first presentation to a physician for venous disorders symptoms, for each patient; venous reflux affecting superficial venous system, objectivated by Doppler ultrasound; no previous endovenous treatment (thermal or nonthermal ablation, foam, etc.); outpatient admission for CVD surgical treatment; serum cholesterol values below 180 mg/dl; signing an informed consent for study participation.
The specific inclusion criterion for the SG was chronic atorvastatin treatment for a period of at least two years’ time (range: 29 +/− 2 months), dosage: 10 mg/day.
According to those criteria, 50 patients were included in the study group, and 52 patients were included in the control group. Regarding the therapeutic indication for atorvastatin treatment among the patients in the study group, 39 patients had high serum cholesterol values at the time of starting the treatment, and 11 patients were using this treatment as primary prevention.
Before surgery, all the patients were examined by duplex ultrasound. All those patients were subsequently operated for venous insufficiency. In accordance with the dimensions and topographic position of the veins that had to be surgically treated, different opening procedures (phlebectomies, classic stripping, or cryostripping) were performed. According to the preoperative mapping of the superficial venous network of the lower limb, only the veins that showed reflux during the ultrasound examination were surgically excluded.
A total of 215 fragments of varicose veins (great saphenous veins, small saphenous veins, or/and their venous tributaries) were collected from the SG, and 179 fragments of varicose veins were collected from the CG. The specimens were collected in fixative solution (10% buffered formalin) and then were analyzed by the Pathology Laboratory. The collected fragments were analyzed macroscopically and microscopically. The macroscopic analysis evaluated the maximum diameter, the thickness of the venous wall, and the aspect of the lumen (free/thrombosed).
For the microscopical analysis, all the venous fragments were prepared on microscope slides. In this regard, several cross-sections were cut from the areas of maximum wall thickness. Any existing thrombus was included. The processing of the parts was performed manually by dehydration in alcoholic solutions, clearing, paraffining, and performing paraffin inclusion, and sections with a thickness of 4 micrometers were made using the semi-automatic rotary microtome Medite M530. For each case, two successive sections were obtained, these being colored in the usual Hematoxylin–Eosin stain, and the Masson trichrome (with aniline blue) stain to highlight fibrosis. The coloring was performed using Bio Optica reagents, by using an automatic Leica Autostainer XL stainer, following the standard recommended protocols. Microscopically, the evaluation was a qualitative one, tracking the changes at vascular components level: thickening of the intima, thickening of the media, with the eventual disorganization of muscle bundles and/or fragmentation of elastic fibers, respectively, increased collagen quantity and the presence/absence of vasa vasorum in the adventitia. A team of two pathologists analyzed the sections displayed on the slides, using a Zeiss Axioskop 2 Plus microscope. The results represent the common conclusion of both doctors.
The aim of this study was to identify and compare the potential morphological changes that may occur in the venous wall in CVD patients due to the atorvastatin treatment.
2.2 Follow-up and clinical implications
This study represents the continuation of the previous one and followed the clinical implications of the effects of statin treatment in the patient with CVD how that may influence disease progression and postsurgical evolution for both groups of patients, being followed by a series of parameters, early and one year postoperatively. The following data were analyzed: hospitalization period, complications (bruising <2 cm surface, bruising = 2–10 cm surface, hematoma), the postoperative outcomes and the recurrences.
2.3 Statistical analysis
Data obtained from the control and study groups were statistically analyzed using Microsoft Excel. The chi-square test (χ2 test) was used, and for greater accuracy, for the small sample size, we used Fisher’s exact test. Student’s t distribution test was also used for small study groups with continuous distribution of values. In order to have independent results between the values obtained, the Pearson correlation coefficient was applied. We specify that the resulting p-value below <0.05 was considered statistically significant.
2.4 Ethical approval
This research was conducted at the Timișoara Emergency County Hospital, in the Phlebology Department, with the consent of the Ethics Commission (REC number: HR.233/04.03.2021, REC number: NR. 332/14.10.2022) and in accordance with the rules of the Helsinki Declaration.
For the study group, the age range varied between 44 and 73 years (mean age–56.32). For the control group, the age range varied between 43 and 75 years (mean age–55.08 years). Regarding this parameter, the groups were statistically equivalent.
Body-mass-index analyses revealed normal distribution in the groups. Student’s t test was used for the statistical comparison between groups, but the result did not reveal significant differences (p = 0.95). From the descriptive point of view, the variation range of BMI was 19.7–37.9 kg/m2 (average 28.25 +/−4.36 kg/m2; median 28.25 kg/m2) for the study group, while the BMI range of the control group was within 20.5–38.2 kg/m2 (average 28.3 +/− 4.02 kg/m2; median 28.4 kg/m2).
Intravenous thrombi were not identified in many cases, the most frequent being observed free venous lumen (study group – 45 patients: free lumen, 5 patients: the lumen was occupied by thrombus; control group −43 patients: free lumen, 9 patients: the lumen was occupied by thrombus). There were not observed statistically significant differences were between the groups (p = 0.28).
Maximum venous diameter analyses revealed in the study group values which ranged between 0.2–1.3 (mean 0.45 +/− 0.303; median 0.45), while in the control group the values ranged between 0.2 and 1.6 (0.781 +/− 0.29; median 0.7). From a statistical point of view, highly significant differences are highlighted for this parameter when comparing the two groups (p = 0.00078). In the case of the SG, a functional impairment is observed predominantly in the small-caliber veins (venous tributaries and collateral veins), while in the CG the major trunks (great saphenous veins, small saphenous veins) were affected in most of the patients.
For the venous wall thickness parameter, no statistical differences between the analyzed groups were noted. Descriptively, values between 0.1 and 0.5 centimeters were found in SG (average of 0.21 +/− 0.1; median 0.2), while in CG, the values ranged between 0.1 and 0.6 centimeters (average 0.2 +/− 0.14; median 0.2).
A statistically significant difference between groups was observed regarding thickening of the venous TI (p = 0.04). Venous TI thickening was identified in 20 patients from SG, and in 31 patients from CG.
Analyses of venous TM thickening, with the four cases found (collagen; collagen + muscle fibers; muscle fibers; without thickening) revealed statistically significant differences (p = 0.0079) between groups. Results regarding TI and TM thickening are presented in Table 1.
Thickening of tunica intima (TI)
study group
control group
yes
20
31
no
30
21
χ2Test p = 0.047628
Thickening of tunica media (TM)
study group
control group
yes, collagen
40
26
yes, collagen + muscle fibers
5
11
yes, muscle fibers
5
11
no
0
4
Fisher’s Exact Test p = 0.0079
Table 1.
Analysis of tunica intima (TI) and tunica media (TM) thickening for both groups.
The presence of disorganized muscle bundles in the TM did not revealed statistically significant differences between groups (p = 0.11). Also, the analysis of the fragmentation of elastic fibers from TM showed insignificant results, also (p = 0.57). A weak correlation (0.66) between the disorganized muscle bundles and the fragmentation of the elastic fibers in the TM was observed in the study group, fact that was noted in the control group (0.57), too. This observation suggests that the correlation of these parameters is not a consequence of the atorvastatin treatment.
No statistically significant differences between the two groups (p = 0.92) regarding the presence of increased collagen in TA was observed.
In this study, the absence of vasorum vessels in TA was an interesting parameter. Despite the fact that it provided significant “p” values in the χ2 test, the results were slightly above the minimum value of 0.05 in the Fisher test. For that reason, it could be considered a questionable result.
The morphology of the analyzed specimens is presented in Figure 1 for SG and Figure 2 for CG.
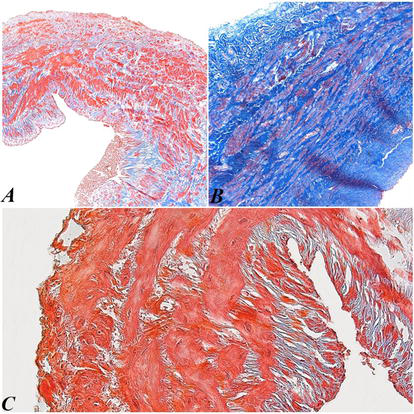
Figure 1.
Most of the study cases showed a significant infiltration at the vascular wall, and in some cases, the intima appeared thicker than media (A, original magnification x100). Thickening of the tunica media was observed, with collagen deposits and fibrous tissue between muscle fibers (C, original magnification x200). Also, Masson’s trichrome staining showed subendothelial collagen deposition with reduced intimal smooth muscle cells (B, original magnification x200).
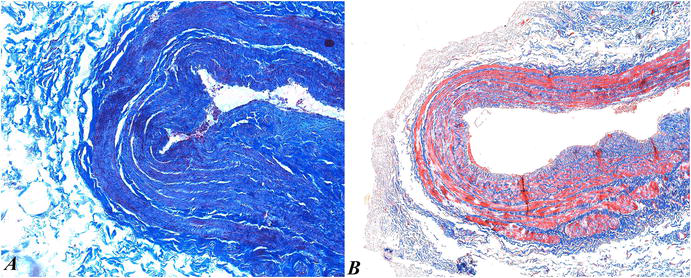
Figure 2.
In the control group, most of the cases showed moderate intimal thickening, with medial thickening through collagen deposits and hypertrophy of muscle fibers (A, original magnification x200). In some cases, muscle bundles were disorganized, with fragmentation of elastic fibers in the media, and absence of vascularity in the adventicea (B, original magnification x100).
Analyzing the correlations identified with respect to the studied parameters, the closest correlation was found between wall thickness and increased collagen in TA (0.83), a correlation that was not observed in CG. We can, therefore, consider this fact to be related to the atorvastatin treatment. To a slightly lower degree (0.61), a thickening of the TI correlated with the increase of collagen in the TA was also identified. The last correlation found in this study was the one between the maximum diameter and the wall thickness (0.69). Although a correlation is observed between these two parameters, it should be taken into account that no statistically significant differences were observed between groups, except in terms of the maximum venous diameter. Correlations are presented in Table 2, the relevant values being highlighted.
code
1
2
3
4
5
6
7
8
9
10
Study group
1
1
2
0.1804
1
3
−0.1943
−0.1415
1
4
0.0550
−0.2736
0.6914
1
5
−0.0863
−0.1319
0.2560
0.4678
1
6
0.2526
0.0650
−0.2936
0.0565
0.2721
1
7
−0.1827
−0.2423
0.4113
0.3696
0.25
0.1360
1
8
−0.0807
−0.1920
0.5285
0.3234
0.1666
0
0.6667
1
9
−0.0700
−0.2887
0.3570
0.8347
0.6123
0.1666
0.4082
0.1020
1
10
—
—
—
—
—
—
—
—
—
1
Control group
1
1
2
0.1323
1
3
−0.0033
0.1677
1
4
0.0205
0.2445
0.3350
1
5
−0.0065
−0.1368
−0.0544
0.0413
1
6
0.2477
0.0177
0.0628
0.1978
0.1494
1
7
−0.0268
−0.0982
0.1254
0.2721
0.1805
0.4612
1
8
0.2212
0.0822
0.2704
0.1368
0.1869
0.3768
0.5728
1
9
−0.0396
0.1262
0.2503
0.2040
0.0038
0.1332
0.3514
0.3629
1
10
0.1926
0.0507
0.1112
0.0350
0.1355
0.1689
0.3662
0.4482
0.3374
1
Table 2.
Correlations between the analyzed parameters (1–10) * for the study and control group (Pearson correlation coefficients)* 1- Age (years); 2- BMI; 3- Maximum diameter (cm); 4- Wall thickness (cm); 5- Thickening of TI; 6- Thickening of TM; 7-Disorganized muscle bundles on TM; 8- Fragmentation of elastic fibers in TM; 9- Collagen increased in TA; 10- Absence of vasa vasorum in TA.
Regarding short-term postoperative follow-up, the following complications were encountered: bruising <2 cm surface in 9 cases (18%) in the SG and 12 cases (23.07%) in the CG; bruising = 2–10 cm in 5 cases (10%) in the SG and 9 cases (17.30%) in the CG; haematoma in one case (2%) in the SG and 2 cases (3.84%) in the CG. Although the proportions in which these complications were observed vary between the two groups, no statistically significant differences were highlighted. However, due to the slightly reduced number of these complications in the SG, it was associated with a shorter hospitalization period (average = 1.34 days) compared to the CG (average 1.75 days), statistically significant difference (p = 0.002). Regarding postoperative analgesia, no statistically significant differences were observed between the two groups regarding the type and quantity of analgesic drugs needed in postoperative pain management.
Overall, the postoperative outcomes were favorable in both groups. At the one-year evaluation, recurrent varicose veins presented as unsystematized varicose veins objectivable in the operated limb in clinical setting, were identified in two cases from the CG and in no case from the SG. However, no statistically significant differences were highlighted between the two groups from this point of view.
Only the venous segments that showed reflux during duplex examination were surgically removed; therefore, the maximum diameters of the veins analyzed in this study refer strictly to these specimens. At the same time, we must take into account the fact that the surgically removed specimens were fixed in formalin solution, which led to a contraction of the veins and a decrease in their diameter through the action of the solution on the tissues. However, given the fact that all specimens were collected, prepared, and stored in the same way, the results obtained faithfully reflect the differences that appear between the study groups.
There are literature data which claim that the thickness of the GSV wall may increases with age, and it could be also slightly influenced by patient’s gender [12, 13]. Although this study included patients with a wide range of ages, and the groups were made up of patients of both sexes, we did not identify statistically significant correlations between these parameters, the thickness of the venous wall, or the total diameter of the vessel.
In accordance with literature data, analyzing the control group, it was observed that CVD is associated with an increase in venous diameter [14]; a thickening of venous TI and TM [15]; that collagen content and thickness of the wall were increased at the level of the proximal segments compared to the distal ones [16]. However, the predominant damage to small-caliber vessels (collateral and perforating veins) which was noted in the study group, as well as the close correlation between the thickness of the venous wall and collagen deposits in the adventitia in these patients, suggest that these aspects could be related with the atorvastatin treatment.
Having a high efficiency in reducing serum cholesterol, current data suggest that atorvastatin is one of the most frequently used drugs in the treatment of dyslipidemias [17, 18]. Most frequently in current clinical practice, doses of 10–40 mg are used; higher doses being rarely used [19]. For the uniformity of the study group, only patients treated with doses of 10 mg of atorvastatin per day were included in this research. In this sense, a future direction of research aimed at prospective and randomized studies on larger groups of patients, would be useful to evaluate the evolution of CVD and the subsequent changes that occur at the level of the venous wall in patients treated with higher doses of atorvastatin, or with other statins; those studies will be useful for a comparative analysis and a better understanding of how these drugs have an effect on phlebological diseases.
There are literature data which claim that the increased number of apoptotic cells in the venous wall structure in patients with chronic venous insufficiency phenomenon were noted mostly in the proximal lower limb vein specimens, and could be involved in the final fibrosclerotic process acceleration, a main characteristic of the varicose vein wall [20]. Even if with the appearance of irreversible changes occurring in the more advanced stages of CVD (CEAP class >3) a decrease in inflammatory markers can be observed [21], as a result of the resolution of repeated inflammatory phenomena and fibrosis [22, 23], the inflammatory component remains one of the main factors incriminated in the emergence of this disease [23, 24, 25]. Due to the anti-inflammatory effect of statins on the vascular wall [8], as in the case of similar substances that reduce inflammation in the venous endothelium such as sulodexide [25, 26], the progression of CVD seems to be slowed down. This statement is supported by the observations of our study which proves a predominant impairment of the smaller veins within the study group.
At the same time, the anti-inflammatory properties of statins associated with their vasculotrophic and vasomotor effects [8] can explain the clinical observations, which highlight a rapid favorable postoperative evolution, including a decrease in hospitalization time, and a much lower complications rate. The fact that the absence of vasa vasorum in TA was not observed in any case of the study group, correlated with the data from the literature that prove the beneficial impact of statins exerted on blood vessels [8] are arguments that support the hypothesis that limiting CVD only to small caliber vessels with local fibrosis could be a result of atorvastatin treatment. These observations suggest that statin treatment may have a role on venous tone and trophicity. By improving the nutrient blood supply in the venous wall through vassa vasorum vessels, the vein tone is maintained for a longer time, and by this way, the progression of CVD could be delayed.
Moreover, there are several other studies that prove beneficial clinical effects of statins on various venous pathologies. A study conducted by Evangelista et al. showed that in the management of venous ulcers, simvastatin 40 mg daily in addition to standard wound care and compression is associated with a significant improvement in healing rate and time, as well as a better QoL for these patients [27]. There are several more studies in this field of investigation that support this hypothesis [28]. Furthermore, addition of simvastatin to standard therapy for the prevention of variceal rebleeding does not reduce rebleeding, but increases survival in patients with liver cirrhosis [29].
Additionally, statins seem to also impact venous thromboembolism. Lipid lowering therapy is associated with decreased venous thromboembolism risk after adjusting for known risk factors [30]. Several studies recommend that statins may be an alternative to anticoagulant treatment in thrombus formation and embolic events prevention [31, 32]. Considering the fact that deep venous thrombosis is one of the most frequent etiological factors responsible for CVD occurrence [33], and superficial venous thrombophlebitis is associated with the CVD progression as well [34, 35], the effects of statins may explain the observations related to the SG. Intraluminal thrombi where noted in 2.25 times lower percentage in the SG (4 patients) comparing with CG (9 patients). Those observations may be the result of the statin treatment and its beneficial effects on the circulatory system, and implicitly, on the morphology of the venous wall.
Overall, the results of this study suggest that atorvastatin treatment provide additional benefits in patients with CVD, this medication bringing anti-inflammatory, anticoagulant, phlebotonic and phlebotrophic effects. According to this study results, minimally invasive surgical procedures for phlebological patients that combine statin medication should be considered. In those cases, ASVAL technique could be performed for reflux veins excision [36]. The preservation of GSV was described in several papers [37, 38, 39]; if during clinical follow-up venous reflux is noted, venous ablation could be achieved by intravenous procedures [40], such as foam sclerotherapy [41], intravenous laser treatment [42], or VenaSeal. Preservation of the GSV can be considered a useful aspect in this category of patients under the conditions of a potential need for a venous graft for a vascular bypass, also.
Atorvastatin treatment seems to play a role in the morphological modifications of the venous wall associated with CVD, leading to increased collagen deposits and a relatively concentric parietal thickening, affecting all venous parietal layers. In this category of patients, CVD expression is predominantly observed in smaller vessels, suggesting that the disease progresses slowly to larger venous trunks. The anti-inflammatory role of statin medication can be considered beneficial for the surgical phlebological patient. Moreover, the results of the study suggest a potential phlebotonic and phlebotrophic effect of statins. However, despite the fact that at first sight, the results of this study suggest that in this category of patients, minimally invasive procedures and conservative approach for GSV and SSV may be recommended, long-term clinical follow-up and further studies on larger number of patients are needed to determine if statin drug treatment could be considered as a decisional factor in CVD management.
A part of this work, which represents the initial stage of this study, was published in “Phlebology: The Journal of Venous Disease,” Volume 37 Issue 3, April 2022, as a research article entitled “Impact of statin treatment on patients diagnosed with chronic venous disease.” “Morphological analysis of the venous wall and clinical implications”. The initial article was cited accordingly.
The author has no other conflicts of interest to declare.
Clinical, Aetiological, Anatomical and Pathological Classification
LDL
low-density lipoprotein
SG
study group
CG
control group
BMI
body mass index
TI
tunica intima
TM
tunica media
TA
tunica adventitia
GSV
great saphenous vein
SSV
small saphenous vein
References
1.Rabe E, Guex JJ, Puskas A, Scuderi A, Fernandez Quesada F, VCP Coordinators. Epidemiology of chronic venous disorders in geographically diverse populations: Results from the vein consult program. International Angiology. 2012;31(2):105-115
2.Rabe E, Berboth G, Pannier F. Epidemiologie der chronischen Venenkrankheiten [Epidemiology of chronic venous diseases]. Wien Med Wochenschr. 2016;166(9):260-263. DOI: 10.1007/s10354-016-0465-y
3.Fakhry AM. Egyptian clinical practice guidelines of venous diseases from theory to practice. Acta Phlebology. 2022;23:1-2. DOI: 10.23736/S1593-232X.22.00522-7
4.Durga DR, Mounika N, Mudimala P, Adela R. Efficacy and safety of Saroglitazar in patients with cardiometabolic diseases: A systematic review and Meta-analysis of randomized controlled trials. Clinical Drug Investigation. Dec 2022;42(12):1049-1064. DOI: 10.1007/s40261-022-01219-6. Epub 2022 Nov 4. PMID: 36329293
5.Saklayen MG. The global epidemic of the metabolic syndrome. Current Hypertension Reports. 2018;20(2):12. DOI: 10.1007/s11906-018-0812-z
6.Noubiap JJ, Nansseu JR, Bigna JJ, Jingi AM, Kengne AP. Prevalence and incidence of dyslipidaemia among adults in Africa: A systematic review and meta-analysis protocol. BMJ Open. 2015;5(3):e007404. DOI: 10.1136/bmjopen-2014-007404
7.Abdullah K, Rohatgi A. Statins: Practical considerations - A review. European Cardiology. 2014;9(2):71-75. DOI: 10.15420/ecr.2014.9.2.71
8.Koh KK. Effects of statins on vascular wall: Vasomotor function, inflammation, and plaque stability. Cardiovascular Research. 2000;47(4):648-657. DOI: 10.1016/s0008-6363(00)00146-2
9.Owens CD. Statins and other agents for vascular inflammation. Journal of Vascular Surgery. 2012;56(6):1799-1806. DOI: 10.1016/j.jvs.2012.08.045
10.Bellosta S, Ferri N, Arnaboldi L, Bernini F, Paoletti R, Corsini A. Pleiotropic effects of statins in atherosclerosis and diabetes. Diabetes Care. 2000;23(Suppl 2):B72-B78
11.Matei S-C, Matei M, Anghel FM, Derban MD, Olariu A, Olariu S. Impact of statin treatment on patients diagnosed with chronic venous disease. Morphological analysis of the venous wall and clinical implications. Phlebology. 2022;37(3):188-195. DOI: 10.1177/02683555211053566
12.Chandrashekar A, Garry J, Gasparis A, Labropoulos N. Vein wall remodeling in patients with acute deep vein thrombosis and chronic postthrombotic changes. Journal of Thrombosis and Haemostasis. 2017;15(10):1989-1993. DOI: 10.1111/jth.13793
13.Arima T, Otsuka S, Mitsuoka H, Nakano T, Naito M, Ishibashi H. Site-specific mechanical properties of the human great saphenous vein: Cadaveric comparisons among the thigh, knee, and lower leg harvest sites. Phlebology. 2022;37(6):445-451. DOI: 10.1177/02683555221088103
14.Kim MJ, Park PJ, Koo BH, Lee SG, Byun GY, Lee SR. Association between venous reflux and diameter of great saphenous vein in lower thigh. Journal of Vascular Surgery. Venous and Lymphatic Disorders. 2020;8(1):100-105. DOI: 10.1016/j.jvsv.2019.04.016
15.Bissacco D, Oberto S, Kontothanassis D, Caggiati A. Venous intima-media thickness increases both in deep and superficial systems in patients with great saphenous vein reflux. Journal of Vascular Surgery. Venous and Lymphatic Disorders. 2019;7(6):832-838. DOI: 10.1016/j.jvsv.2019.07.005
16.Labropoulos N, Summers KL, Sanchez IE, Raffetto J. Saphenous vein wall thickness in age and venous reflux-associated remodeling in adults. Journal of Vascular Surgery. Venous and Lymphatic Disorders. 2017;5(2):216-223. DOI: 10.1016/j.jvsv.2016.11.003
17.Malhotra HS, Goa KL. Atorvastatin: An updated review of its pharmacological properties and use in dyslipidaemia. Drugs. 2001;61(12):1835-1881. DOI: 10.2165/00003495-200161120-00012
18.Jameson K, Zhang Q, Zhao C, Ramey DR, Tershakovec AM, Gutkin SW, et al. Total and low-density lipoprotein cholesterol in high-risk patients treated with atorvastatin monotherapy in the United Kingdom: Analysis of a primary-care database. Current Medical Research and Opinion. 2014;30(4):655-665. DOI: 10.1185/03007995.2014.890926
19.Laufs U, Karmann B, Pittrow D. Atorvastatin treatment and LDL cholesterol target attainment in patients at very high cardiovascular risk. Clinical Research in Cardiology. 2016;105(9):783-790. DOI: 10.1007/s00392-016-0991-z
20.Buján J, Jiménez-Cossio JA, Jurado F, Gimeno MJ, Pascual G, García-Honduvilla N, et al. Evaluation of the smooth muscle cell component and apoptosis in the varicose vein wall. Histology and Histopathology. 2000;15(3):745-752. DOI: 10.14670/HH-15.745
21.Sachdev U, Vodovotz L, Bitner J, Barclay D, Zamora R, Yin J, et al. Suppressed networks of inflammatory mediators characterize chronic venous insufficiency. Journal of Vascular Surgery. Venous and Lymphatic Disorders. 2018;6(3):358-366. DOI: 10.1016/j.jvsv.2017.11.009
22.Raffetto JD, Khalil RA. Mechanisms of varicose vein formation: Valve dysfunction and wall dilation. Phlebology. 2008;23(2):85-98. DOI: 10.1258/phleb.2007.007027
23.Buján J, Pascual G, Bellón JM. Interaction between ageing, inflammation process, and the occurence of varicose veins. Phlebolymphology. 2008;15(4):123-130
24.Spiridon M, Corduneanu D. Chronic venous insufficiency: A frequently underdiagnosed and undertreated pathology. Maedica (Bucur). 2017;12(1):59-61
25.Urbanek T, Zbigniew K, Begier-Krasińska B, et al. Sulodexide suppresses inflammation in patients with chronic venous insufficiency. International Angiology. 2015;34(6):589-596
26.Urbanek T, Krasinski Z, Sumińska-Jasińska K, Baum E, Borej-Nowicka G, Begier-Krasińska B, et al. Sulodexide reduces the inflammatory reaction and senescence of endothelial cells in conditions involving chronic venous disease. International Angiology. 2016;35(2):140-147
27.Evangelista MT, Casintahan MF, Villafuerte LL. Simvastatin as a novel therapeutic agent for venous ulcers: A randomized, double-blind, placebo-controlled trial. The British Journal of Dermatology. 2014;170(5):1151-1157. DOI: 10.1111/bjd.12883
28.Jull A, Lu H, Jiang Y. Statins and venous leg ulcer healing: Secondary analysis of data from a cohort of three randomised controlled trials. Wound Repair and Regeneration. 2022;30(2):186-189. DOI: 10.1111/wrr.12987
29.Abraldes JG, Villanueva C, Aracil C, Turnes J, Hernandez-Guerra M, Genesca J, et al. Addition of Simvastatin to Standard Therapy for the Prevention of Variceal Rebleeding Does Not Reduce Rebleeding but Increases Survival in Patients With Cirrhosis. Gastroenterology. 2016;150(5):1160-1170. DOI: 10.1053/j.gastro.2016.01.004
30.Ashrani AA, Barsoum MK, Crusan DJ, Petterson TM, Bailey KR, Heit JA. Is lipid lowering therapy an independent risk factor for venous thromboembolism? A population-based case-control study. Thrombosis Research. 2015;135(6):1110-1116. DOI: 10.1016/j.thromres.2015.04.005
31.Chaffey P, Thompson M, Pai AD, Tafreshi AR, Tafreshi J, Pai RG. Usefulness of statins for prevention of venous thromboembolism. The American Journal of Cardiology. 2018;121(11):1436-1440. DOI: 10.1016/j.amjcard.2018.02.024
32.Biere-Rafi S, Hutten BA, Squizzato A, Ageno W, Souverein PC, de Boer A, et al. Statin treatment and the risk of recurrent pulmonary embolism. European Heart Journal. 2013;34(24):1800-1806. DOI: 10.1093/eurheartj/eht046
33.Malkani RH, Karia R, Thadani S. A study of risk factors of chronic venous insufficiency and its association with features suggestive of preceding or present deep venous thrombosis. Indian Journal of Dermatology. 2019;64(5):366-371. DOI: 10.4103/ijd.IJD_271_18
34.Blättler W, Schwarzenbach B, Largiadèr J. Superficial vein thrombophlebitis--serious concern or much ado about little? VASA. 2008;37(1):31-38. DOI: 10.1024/0301-1526.37.1.31
35.Decousus H, Epinat M, Guillot K, Quenet S, Boissier C, Tardy B. Superficial vein thrombosis: Risk factors, diagnosis, and treatment. Current Opinion in Pulmonary Medicine. 2003;9(5):393-397. DOI: 10.1097/00063198-200309000-00009
36.Atasoy MM, Oğuzkurt L. The endovenous ASVAL method: Principles and preliminary results. Diagnostic and Interventional Radiology. 2016;22(1):59-64. DOI: 10.5152/dir.2015.15161
37.Pittaluga P, Chastanet S, Locret T, Barbe R. The effect of isolated phlebectomy on reflux and diameter of the great saphenous vein: A prospective study. European Journal of Vascular and Endovascular Surgery. 2010;40(1):122-128. DOI: 10.1016/j.ejvs.2010.03.031
38.Pittaluga P, Chastanet S. Persistent incompetent truncal veins should not be treated immediately. Phlebology. 2015;30(1 Suppl):98-106. DOI: 10.1177/0268355515569141
39.Zolotukhin IA, Seliverstov EI, Zakharova EA, Kirienko AI. Short-term results of isolated phlebectomy with preservation of incompetent great saphenous vein (ASVAL procedure) in primary varicose veins disease. Phlebology. 2017;32(9):601-607. DOI: 10.1177/0268355516674415
40.Harlander-Locke M, Jimenez JC, Lawrence PF, Derubertis BG, Rigberg DA, Gelabert HA. Endovenous ablation with concomitant phlebectomy is a safe and effective method of treatment for symptomatic patients with axial reflux and large incompetent tributaries. Journal of Vascular Surgery. 2013;58(1):166-172. DOI: 10.1016/j.jvs.2012.12.054
41.Orsini C, Brotto M. Immediate pathologic effects on the vein wall of foam sclerotherapy. Dermatologic Surgery. 2007;33(10):1250-1254. DOI: 10.1111/j.1524-4725.2007.33261.x
42.Kürşat Bozkurt A, Lawaetz M, Danielsson G, Lazaris AM, Pavlovic M, Olariu S, et al. European College of Phlebology guideline for truncal ablation. Phlebology. 2020;35(2):73-83. DOI: 10.1177/0268355519857362
Written By
Sergiu-Ciprian Matei
Submitted: 08 December 2022Reviewed: 29 January 2023Published: 22 March 2023
 Open access peer-reviewed chapter
Open access peer-reviewed chapter