 Open access peer-reviewed chapter
Open access peer-reviewed chapter
Abstract
In conventional arthroscopic repair of rotator cuff tears, a standard approach involves the use of three portals. However, the anterior portal poses potential risks, including cephalic vein injury leading to hematoma formation and the need for conversion to an open surgical technique, which can be particularly challenging when the patient is positioned laterally. The primary objective of this article is to elucidate an innovative technique employing a modified anterolateral portal, thereby eliminating the need for the conventional anterior portal. This modification significantly mitigates the risk of cephalic vein injury and preserves the integrity of the anterior deltoid muscle, offering a safer and more effective approach to rotator cuff repair.
Keywords
- synovial joints
- shoulder
- arthroscopy
- rotator cuff repair
- surgery
1. Introduction
Rotator cuff injury (RCI) stands out as one of the most prevalent shoulder problems, accounting for approximately 23% of consultations with shoulder surgery specialists. This condition can manifest with painful symptoms, limitations in shoulder mobility and strength, often resulting in work absenteeism. It affects around 20% of the general population, and in individuals aged over 80, the incidence can reach a staggering 50% [1, 2].
While conservative treatment is an initial option, in cases of unsatisfactory progression, surgical treatment is the recommended alternative, performed through open or arthroscopic procedures. Among surgical techniques, arthroscopy is highlighted for providing optimized joint visualization with minimal surrounding tissue trauma [3, 4].
Traditionally, arthroscopic repair of RCI involves the creation of three classic surgical portals: anterior, posterior, and lateral, with the option to incorporate accessory portals. Creating arthroscopic portals in the shoulder may seem like a straightforward procedure, but there are risks associated with neurovascular structure injury near the joint. Anatomical studies in cadavers have shown that anterior portals pose the highest risk of injuries. Out of every six dissections conducted in cadavers exposed to anterocentral and anteroinferior portals, one resulted in cephalic vein injury, accounting for 16.6% of the total cadavers dissected with cephalic vein injuries following shoulder arthroscopy using these portals [5, 6].
The aim of this manuscript is to present an arthroscopic technique for RCI repair and acromioplasty, utilizing a variation of the lateral-anterior portal, with the intention of avoiding anterior portals and, in turn, reducing the associated risks.
2. Description of the technique
This study received approval from the Research Ethics Committee of the institution (CAAE 59538722.3.0000.5374; number 5,568,644 issued on August 8, 2022). The indications and contraindications remain consistent with those of the traditional anterior portal arthroscopic repair.
3. Patient positioning
On the surgical table following general anesthesia, the patient is placed in a lateral decubitus position on the side opposite to the one being operated. The upper limb to be treated is secured within a shoulder distraction system in a lateral decubitus, using a tubular mesh and sterile drapes, which facilitates abduction, anterior flexion, and traction during the surgical procedure. Traction is applied using weights approximately equal to 10% of the patient’s body weight, typically ranging between 5 and 10 kg, providing adequate arthroscopic visualization. Proper head protection and cushions on all bony prominences are necessary to prevent pressure injuries and neuropraxias. The primary advantage of this position is the reduced risk of cerebral hypoperfusion.
4. Creation of portals
Following the preparation and placement of surgical drapes, the initial step involves marking the portals, utilizing three primary anatomical references: the scapular spine, the acromion, and the clavicle. The posterior portal is located 2 to 3 cm below and 1 to 2 cm medially from the posterior-lateral edge of the acromion. Subsequently, a new marking is made, starting from the medial curvature of the acromion, extending from the posterior part of the acromioclavicular joint, moving laterally across the acromion. The lateral-anterior (LA) portal is marked 2 cm distal and lateral to the acromion, immediately up to 1 cm anterior to the lateral marking (Figure 1).

Figure 1.
Marking of the two portals for shoulder arthroscopy: The traditional posterior and the lateral-anterior (LA).
Through the posterior portal, the trocar is introduced, followed by a 30° angled scope into the intra-articular glenohumeral space for diagnostic arthroscopy. The trocar is then inserted directly into the subacromial space with the scope facing the underside of the acromion. Before introducing the cannula into the LA portal, the assistance of an intravenous catheter (18-gauge Jelco) is used, which can be visualized with the scope already inserted into the posterior portal.
The key differentiators of this technique are the omission of anterior portals and, notably, the accessory portal created directly lateral to the acromial edge and anterior to the lateral marking with the aid of the 18-gauge Jelco catheter for locating the most suitable anchor insertion site. A small incision of 2 to 3 millimeters is sufficient for this portal, eliminating the need for cannula insertion. Through this portal, the anchor guide is introduced, and subsequently, the anchor is secured in the optimal position for RCI repair. By rotating the limb internally and externally, the ideal anchor or anchors’ positions can be determined.
5. Diagnostic arthroscopy and acromioplasty
We begin by inserting a 4.0 mm, 30° angled optic scope coupled to a camera with a light source through the posterior portal into the subacromial space. After visualizing the underside of the acromion, the scope is directed toward the lateral region of the shoulder. Using an 18-gauge intravenous catheter (Jelco 18) inserted into the previously marked LA portal, the optimal position for cannula insertion is confirmed.
Once the cannula is introduced through the LA portal, other instruments are sequentially inserted through this portal. Soft tissue debridement is performed using a shaver blade and radiofrequency probe to remove devitalized tissues and expose the undersurface of the acromion. Subsequently, acromioplasty and lateral clavicle resection are carried out with the bone shaver, if required. The scope is then directed to the patient’s humerus, allowing visualization of the subacromial bursa, which is then excised during bursectomy.
At this point, the rotator cuff is visible. Under direct visualization through the scope, the extent of the lesion is assessed, and the most suitable anchor placement location is determined. Irregular edges of the damaged rotator cuff are debrided using the soft tissue shaver, and the humeral surface, which will serve as the footprint for rotator cuff reattachment, is decorticated with the bone shaver. Once again, with the aid of the intravenous catheter (Jelco 18) inserted immediately lateral to the acromion, the optimal anchor insertion site is confirmed to ensure that it is positioned at approximately a 45° angle relative to the humeral surface. A small incision of 2 to 3 millimeters is made at the location where the venous catheter was inserted to create the accessory portal.
Through this accessory portal, the anchor guide is introduced, and subsequently, the anchor is secured in the most appropriate position for rotator cuff repair. By externally and internally rotating the operated limb, the optimal anchor position can be identified. The anchor, loaded with two suture threads, is inserted at a 45° angle relative to the humerus. Each suture thread is separately secured (Figure 2).
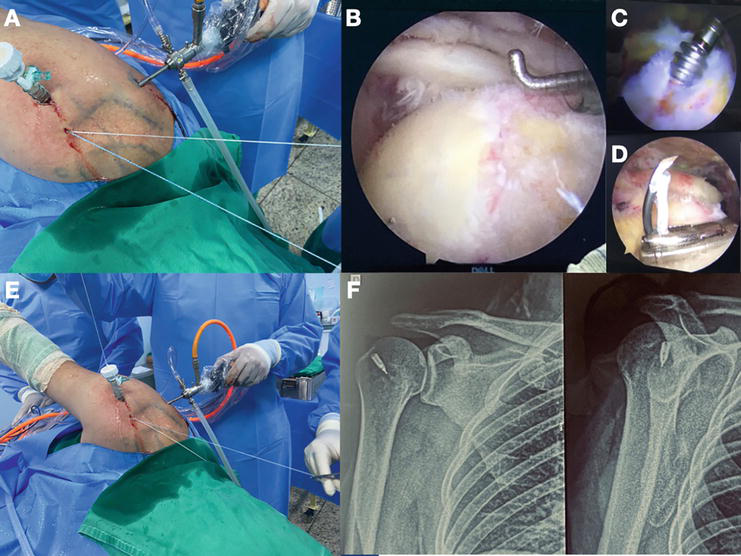
Figure 2.
Repair of the rotator cuff injury using the two-portal technique; A) patient in lateral decubitus position, with the scope introduced through the posterior portal and the cannula in the lateral-anterior (LA) portal. An accessory incision is used to insert the anchor; B) arthroscopic image of the shoulder with a rotator cuff injury; C) insertion of the anchor into the humeral head; D) passage of the suture through the cuff; E) retrieval of the thread and knot through the LA portal; F) shoulder X-rays with a metallic anchor in the humeral head.
One of the suture threads, in the most suitable position, is selected, and its two ends are separated. One end is brought through the LA portal and fastened to a suture passer with a retrieval system. The suture passer is introduced through the cannula and is used to repair the rotator cuff. The end of the suture thread is brought back through the LA portal and secured. The other end of the same suture thread is also brought to the LA portal. With both ends of the thread through the LA portal, the self-locking “SMC” knot is used for the repair and fixation of the cuff to the anchor and bone.
If necessary, the same procedure can be performed with the other suture thread loaded in the anchor already inserted. Additionally, more anchors can be used if the extent of the lesion requires it, using the same accessory portal for anchor insertion and rotating the limb to locate the optimal position. This allows for the technique to be employed even for extensive lesions (Figure 3). If required, acromioplasty can also be performed through the LA portal (Figure 4).
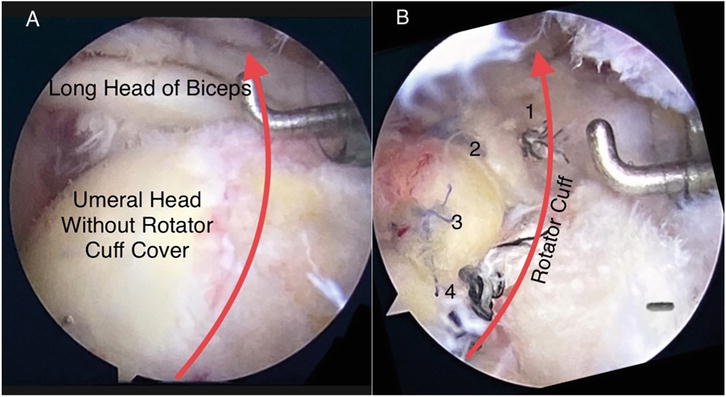
Figure 3.
A) Extensive rotator cuff injury; B) repaired with two anchors and four sutures using the two-portal and accessory technique.
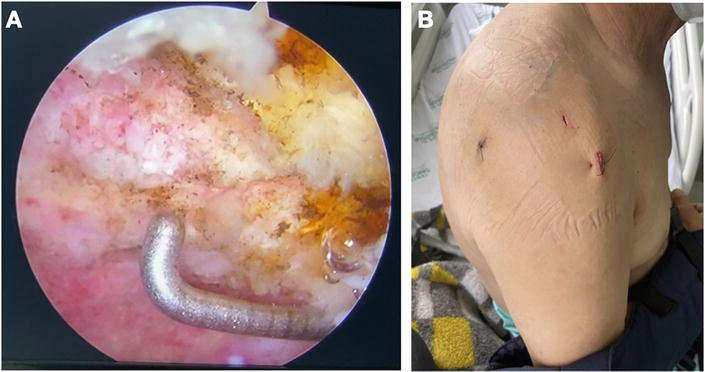
Figure 4.
A) Acromioplasty through the LA portal; B) final appearance of the surgical scar with two portals and an accessory.
6. Final comments
The primary outcome of this study is the detailed description of the surgical technique for repairing rotator cuff injuries (RCI) and performing acromioplasty using a modified lateral-anterior portal (LA) while avoiding the use of the anterior portal. This technique offers several key advantages, including a reduced risk of cephalic vein injury, less trauma to the deltoid muscle (particularly its anterior portion), and cost savings due to the use of a single cannula.
Other authors have previously proposed various portal approaches for shoulder RCI repair. One technique involved creating arthroscopic portals based on the location of the rotator cuff tear. However, this approach utilized four portals: posterior, anterior, lateral, and anterosuperior to the suprascapular fossa. In our opinion, the use of the anterior portal does not resolve the issue of the risk of cephalic vein injury with significant bleeding and the potential for conversion to open surgery [7].
Another technique was suggested, using only the posterior and anterolateral portals. The author introduced a variation in which the anterolateral portal is positioned more distally for repairing the long head of the biceps tendon. The most significant finding of the study was that 11 out of 23 portals (47.8%) in the distal anterolateral location were in contact with a distal branch of the axillary nerve. The proximity and frequent contact of this portal with the distal axillary nerve branches on the undersurface of the anterior deltoid necessitate caution when placing these portals. Since our technique focuses on RCI repair, the lateral-anterior portal described here is more lateral and proximal, reducing the risk of axillary nerve branch injury [8].
In another described technique, two portals are used, a single anterolateral working portal in conjunction with a posterior viewing portal, allowing for several procedures, including subacromial bursectomy, acromioplasty, distal clavicle excision, supraspinatus tendon rupture repair, and long head of the biceps tenodesis. However, this study differs from the technique proposed here because the patient is placed in a beach chair position, and the location of the anterolateral portal is more anterior compared to our approach. In our opinion, the more anterior the portal, the higher the risk of venous injury [7].
The limitation of this study is the absence of a case series with data to support the safety and effectiveness of the technique. Although the author has already successfully performed a significant number of cases, a prospective clinical study will be conducted in the future to compare the efficacy and safety of the two-portal technique to the traditional anterior portal approach.
References
- 1.
Yamamoto A, Takagishi K, Osawa T, et al. Prevalence and risk factors of a rotator cuff tear in the general population. Journal of Shoulder and Elbow Surgery. 2010; 19 (01):116-120 - 2.
Malavolta EA, Gracitelli MEC, Assunção JH, Pinto GMR, da Silveira AZF, Ferreira AA. Shoulder disorders in an outpatient clinic: An epidemiological study. Acta Ortopédica Brasileira. 2017; 25 (03):78-78 - 3.
Godinho GG, Souza JMG, Bicalho LA. Reparo das rupturas do manguito rotador do ombropela videoartroscopia cirúrgica: técnica. Revista Brasileira de Ortopedia. 1996; 31 (4):284-288 - 4.
Garrett WE, Swiontkowski MF, Weinstein JN, et al. American Board of Orthopaedic Surgery Practice of the orthopaedic surgeon: Part-II, certification examination case mix. The Journal of Bone and Joint Surgery. American Volume. 2006; 88 :660-667 - 5.
Meyer M, Graveleau N, Hardy P, Landreau P. Anatomic risks of shoulder arthroscopy portals: Anatomic cadaveric study of 12 portals. Arthroscopy. 2007; 23 (5):529-536. DOI: 10.1016/j.arthro.2006.12.022 - 6.
Aouad D, El Rassi G. Shoulder arthroscopic rotator cuff repair with biceps Tenodesis and Acromioplasty using a single working portal. Arthroscopy Techniques. 2021; 10 (4):e1125-e1129. DOI: 10.1016/j.eats.2021.01.005 - 7.
Kim SH, Ha KI, Ahn JH, Park JH. Differential arthroscopic portal placement for rotator cuff repair. Arthroscopy. 2002; 18 (8):E43. DOI: 10.1053/jars.2002.29941 - 8.
Knudsen ML, Hibbard JC, Nuckley DJ, Braman JP. The low-anterolateral portal for arthroscopic biceps tenodesis: Description of technique and cadaveric study. Knee Surgery, Sports Traumatology, Arthroscopy. 2014; 22 (2):462-466. DOI: 10.1007/s00167-013-2444-9. Epub 2013 Feb 12