Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
To purchase hard copies of this book, please contact the representative in India:
CBS Publishers & Distributors Pvt. Ltd.
www.cbspd.com
|
customercare@cbspd.com
Chronic hepatitis C virus (HCV) infection in chronic kidney disease (CKD) patients can accelerate the decline of kidney function, increase the risk of kidney failure, and increase mortality in CKD patients on hemodialysis (HD). Chronic HCV infection is also a risk factor for mortality in kidney transplant patients. Effective detection, evaluation, and treatment for HCV infection can improve kidney and cardiovascular outcomes. In the subsequent 10 years, direct-acting antivirals (DAAs) have become available. DAAs enabled a greater rate of HCV eradication in CKD populations. Patients with stage 1-3b CKD (G1-G3b) can be treated with any licensed DAA regimens. The recommended DAA treatment regimens for CKD stage 4–5, including those undergoing HD (G4-G5D), are the sofosbuvir-free combination therapies (grazoprevir/elbasvir and glecaprevir/pibrentasvir). While sofosbuvir-based regimens are much more accessible, data showed that some countries have limited access (due to drug availability and high cost) to sofosbuvir-free regimens. Because of this phenomenon, some countries have had difficulty providing sofosbuvir-free treatment to CKD G4-G5D patients. As an alternative to those conditions, some clinicians have approved the usage of sofosbuvir-based regimens in CKD G4-G5D, but this decision is still debatable. Kidney Disease: Improving Global Outcomes (KDIGO) 2018 did not approve sofosbuvir-based regimens for CKD G4-G5D. On the contrary, other studies and guidelines have approved sofosbuvir-based regimens for CKD G4-G5D patients.
Gastroenterohepatology Division, Internal Medicine Department, Faculty of Medicine, Udayana University/Prof. I.G.N.G. Ngoerah General Hospital, Denpasar, Bali, Indonesia
Komang Agus Wira Nugraha
Gastroenterohepatology Division, Internal Medicine Department, Faculty of Medicine, Udayana University/Prof. I.G.N.G. Ngoerah General Hospital, Denpasar, Bali, Indonesia
*Address all correspondence to: gsomayana@yahoo.co.id
1. Introduction
Hepatitis C virus (HCV) infection is a global health problem that leads to liver cirrhosis, liver decompensation, and hepatocellular carcinoma (HCC) [1]. HCV infection and chronic kidney disease (CKD) are epidemically correlated [2]. There is a link between HCV and CKD; thus, on the one hand, HCV can cause CKD through mixed cryoglobulinemia in the renal matrix or through the development of glomerulonephritis. On the other hand, CKD (especially in stage 5 CKD) is a risk factor for HCV as many patients receive blood transfusions, hemodialysis (HD), or develop a donor-derived infection after kidney transplantation [1, 3].
Chronic HCV infection in CKD patients can accelerate the decline of kidney function, increase the risk of kidney failure, and increase mortality in CKD patients with HD [4]. Chronic HCV infection is also a risk factor for mortality in kidney transplant patients. Other post-transplant complications in untreated chronic HCV infection patients are diabetes mellitus, chronic allograft nephropathy, rapid graft loss, and lymphoproliferative disorders [3, 5, 6, 7].
Effective detection, evaluation, and treatment for HCV infection can improve kidney and cardiovascular outcomes [4]. In the subsequent 10 years, the development of direct-acting antivirals (DAAs), which enabled a greater rate of viral eradication in CKD populations infected with HCV, has become available [4, 8]. Patients with stage 1-3b CKD (G1-G3b) can be treated with any licensed DAA regimen [8, 9, 10]. Several regimens also have been approved for use in patients with HCV infection and stage 4–5 CKD (G4-G5), including those on dialysis (G5D) [4]. The recommended DAA treatment regimens for CKD G4-G5D are the sofosbuvir-free combination therapies that consist of grazoprevir/elbasvir and glecaprevir/pibrentasvir [8, 10].
Unfortunately, the availability and cost of sofosbuvir-free therapies have become a problem for low- and middle-income countries. Most countries can only access sofosbuvir-based therapies. In 2019, a total of 62 low- and middle-income countries had registered at least one version of sofosbuvir/daclastavir, sofosbuvir/velpatasvir, or sofosbuvir/ledipasvir. Low- and middle-income countries can now aim for a 12-week course of treatment with WHO-prequalified generic sofosbuvir and daclatasvir for as little as US$ 60 per patient [11]. Therefore, high cost and limited drug availability of certain DAA regimens are the major barriers to achieving HCV eradication in CKD patients [4].
Sofosbuvir-based regimens are mainly eliminated through the renal route and have been initially licensed for patients with a glomerular filtration rate (GFR) above 30 mL/min [12, 13, 14]. Its use in patients with CKD G4-G5D is not indicated in label [12]. On the contrary, several studies found that sofosbuvir-based regimens were effective and safe in patients with GFR ≤30 mL/min [12, 15]. All DAAs are now recommended by the American Association for the Study of Liver Diseases (AASLD) for GFR ≤ 30 mL/min [15]. Based on the controversies and growing studies of DAAs treatment, this review will summarize the epidemiology, detection, evaluation, and recommended DAAs treatment in CKD patients. The role of sofosbuvir-based regimens in CKD G4-G5D patients will also be briefly discussed here. Finally, we hope this review could help us to create optimal strategies aimed at improving the quality of care and overcoming drug availability or cost barriers for CKD patients.
HCV is a common infection in CKD patients, with a prevalence rate of 10–16% worldwide [16]. The serum anti-HCV and HCV ribonucleic acid (RNA) have been detected in a significant proportion of patients with CKD [1]. According to the Dialysis Outcomes and Practice Patterns Study (DOPPS, 1996–2005), HCV prevalence in HD patients was 9.9% overall [17]. Among patients with HD, its prevalence in Belgium is 4%, about 20% in the Middle East, and an intermediate prevalence in Italy, Spain, China, Japan, and Russia [17, 18, 19]. In Taiwan, Malaysia, South Korea, Thailand, Singapore, and Hong Kong, the prevalence of HCV infection in HD patients is 13, 4, 4, 3.96, 2.1, and 0.9% [4]. In the United States (US), the prevalence of chronic HCV infection in HD patients has been estimated to be five times higher than in the general population [3]. HCV prevalence was higher among US black patients compared with US non-black patients (8.9 vs. 4.1%) [17].
The characteristics of patients associated with the prevalence of HCV infection in prevalent patients undergoing dialysis included younger age; US black race; longer dialysis vintage; history of hepatitis B virus (HBV), human immunodeficiency virus (HIV) positivity, and cirrhosis; substance abuse; and glomerulonephritis as the etiology of end-stage renal disease. Patients with HCV infection had an unadjusted lower prevalence of coronary artery disease (CAD), hypertension, peripheral vascular disease, diabetes mellitus, congestive heart failure (CHF), lung disease, cerebrovascular disease, and cancer, which reflects the younger age of HCV infection patients [17].
HCV incidence was 1.2 per 100 patient-years in the DOPPS 5 study (2012–2015) and ranged from 0 in Belgium, Sweden, and Turkey to 2.9 in Italy. Patients who had HD for more than 10 years had higher rates of HCV seroconversion (seroconversion among patients with an initial negative HCV antibody measurement). HBV-positive and HIV-positive patients also had a higher rate of HCV seroconversion. The use of HD isolation stations for chronic HCV infection patients was associated with lower rates of HCV seroconversion, although the association was not significant statistically [17].
The annual incidence of HCV infection in patients with HD has decreased from 2.9 to 1.2% from 1996 to 2015. But on the other side, this annual incidence remains much higher than the global incidence of 23.7 per 100.000 in the general population [17, 18, 19]. The higher incidence and prevalence rate of HCV infection in patients with GFR ≤ 30 mL/min compared to the general population can be attributed to three factors. First, there is a direct association between HCV infection and cryoglobulinemic nephropathy, membranoproliferative glomerulonephritis, or membranous glomerulonephritis. HCV is also associated with insulin resistance, diabetes mellitus, and cardiomyopathies, which could worsen kidney function. Second, the risk of nosocomial HCV infection increases in patients with CKD receiving kidney replacement therapy [1]. In kidney failure patients, dialysis modality is an independent risk factor for acquiring HCV infection, with HD being associated with a higher risk of HCV infection than peritoneal dialysis (PD). HCV seroprevalence and seroconversion rates among HD patients vary widely, suggesting a need for consistent, rigorous local infection control measures [4]. Third, HCV infection may occur as a result of donor-derived infection following kidney transplantation [1, 3].
If acute HCV infection is not treated, approximately about 65.4–92% of patients on maintenance HD develop chronic infection. Making an early diagnosis is difficult because most infected patients are asymptomatic, and have serum alanine transaminase (ALT) levels below the reference limit for subjects without advanced kidney diseases. This condition also makes determining the precise duration of HCV infection difficult for clinicians [20, 21, 22].
Current evidence indicate that the course of HCV infection is less aggressive in patients on hemodialysis than in nonuremic patients. Studies about the effects of HCV genotypes on the progressivity of CKD remain controversial, but HCV viremia is associated with progressive kidney failure [23, 24, 25]. According to REVEAL-HCV studies, patients with HCV genotype 1 infection tended to develop end-stage renal disease. On the contrary, patients with HCV genotype 2 infection are more likely to develop CKD stage 2 or higher [1].
Chronic HCV infection in CKD patients can increase the risk of mortality [4]. Data showed that mortality is a firm outcome of the natural history of HCV infection [1]. A meta-analysis reported that the pooled adjusted hazard ratio for all-cause mortality in HCV-positive patients undergoing hemodialysis was 1.207 (95% CI 1.12–1.30, p < 0.001; I2 = 75.59%) compared with HCV-negative patients [26]. Other meta-analysis revealed the summary estimate for adjusted death risk (all-cause mortality) with anti-HCV antibody across the retrieved studies was 1.26 (95% CI: 1.18–1.34) (P < 0.0001) The overall estimate for adjusted death risk (liver disease-related mortality) was 5.05 (95% CI: 2.53–10.0) (P < 0.0001) [27]. On the other hand, dialysis patients with active HCV infection who undergo kidney transplantation have better survival compared with patients on maintenance dialysis [1]. Unfortunately, the graft survival rates in kidney transplantation recipients with HCV infections are worse than those in kidney transplantation recipients without HCV infections [28].
4. Detection and evaluation of HCV infection in CKD
The first step in the evaluation of chronic hepatitis C in CKD or end-stage renal disease (ESRD) patients is similar to that of other patients in the general population. The evaluation should include biochemical liver function test for alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), and gamma-glutamyl transferase (GGT). Because of pronounced viremia reduction mediated by HD-induced activation CD69+ lymphocytes and an increased serum level of alpha-interferon (IFN-α), chronic hepatitis C in ESRD patients tend to show normal or mildly elevated liver enzymes [28]. Hemodialysis is also responsible for increasing the production of hepatocyte growth factor (HGF), which could stimulate hepatocyte turnover and liver regeneration. HGF plays a protective role against exogenous toxins and is associated with the indolent course of liver disease [28, 29]. The effect of increased HGF may account for less severe histological liver findings. Albumin, bilirubin, platelet count, and prothrombin time (PT) examinations can also reflect liver fibrosis progression. Low platelet and prolonged PT are the signs of advanced liver fibrosis or the development of portal hypertension [28].
Patients with CKD, including those initiating kidney replacement, should undergo screening for HCV. A positive anti-HCV antibody can indicate the presence of an active infection (chronic or acute), the resolution of a past infection, or a false positive. The presence of HCV antibody is not protective against HCV infection, because the virus can escape the host’s immune response even in the presence of HCV antibody. The clinical relevance of positive HCV antibody is limited as a marker of exposure to HCV and persists even after the patient achieves sustained virologic response (SVR) or cure [3]. Therefore, the detection of anti-HCV antibody by screening immunoassays with infection confirmed by nucleic acid testing (NAT) is required to make a diagnosis. In HD patients, the positive predictive value (PPV) of anti-HCV antibody was 73% and the negative predictive value (NPV) was 90%. HCV-RNA was positive in 10% of anti-HCV-negative patients. This figure results from the delay between viremia after contamination and seroconversion (the “window period”). As a result, initial NAT testing should be done in HD units with a high HCV prevalence. Because HD can reduce the level of viremia, NAT blood samples should be drawn before dialysis. However, this reduction in HCV RNA is not dependent on the dialysis schedule or type of membrane used [10].
Anti-HCV antibody will remain the initial screening test for patients with HD, because of its low cost. The HCV core antigen test could be an alternative if the NAT test could not be performed. But for some countries, the HCV core antigen is not yet available and is expensive. Given that HCV core antigen has a detection threshold of at least 3000 IU/mL, and most patients with HCV have high levels of viremia, good concordance between HCV core antigen and NAT has been demonstrated [4].
In immunosuppressed patients (HIV-positive, chemotherapy, or transplant recipients), a HCV RNA test needs to be performed even if the anti-HCV antibody is negative [3]. A study in German reported an overall prevalence of 0.8% of HCV RNA-positive subjects, although HCV antibody levels were negative [30]. An HCV genotype test is still recommended if the patient has detectable HCV viremia to personalize appropriate treatment choices. It is also important to consider potential resistant associated substitutions (RAS) before starting treatment in specific conditions [3].
All HD patients should be screened for HCV infection using the ALT level monthly and the anti-HCV antibody or NAT every 6 months. If a newly acquired HCV infection is detected, all patients should be screened and the testing frequency should be increased [10]. Some countries perform the NAT test annually for patients who either are HD and anti-HCV positive [4].
The cirrhosis condition carries an increased risk of the development of HCC, liver transplantation, or mortality. Guidelines from Kidney Disease: Improving Global Outcomes (KDIGO) 2018, recommended the use of non-invasive markers of liver fibrosis, and liver biopsy can be performed if non-invasive markers are not conclusive or to rule out other liver-related comorbidities. Due to recurrent anticoagulation and uremic platelet dysfunction in HD patients, liver biopsy carries a lot of risks [3].
Transient elastography (fibroscan), AST platelet ratio index (APRI), fibrotest/fibrometer, and Fibrosis-4 (FIB4) index are recommended as an initial test for staging liver fibrosis. Transient elastography measures shear wave velocity from a transducer at the end of an ultrasound probe passing through the liver. The velocity is then converted into liver stiffness measurement and expressed in kilopascal (kPa). A study about the validation of transient elastography in chronic hepatitis C patients with dialysis reported that transient elastography was better than APRI for fibrosis stage ≥ F2 and ≥ F3. The difference was not statistically significant in stage F4, probably because of the small number of cirrhotic subjects in the population of the study [31]. The severity of portal hypertension needs to be confirmed after cirrhosis is suspected or confirmed. Endoscopy is indicated to confirm esophageal varices [10].
5. Treatment of HCV infection in patients with CKD
Multiple studies have found an association between sustained SVR and a reduction in ESRD-related mortality, a reduction in vascular events, an improvement in cryoglobulinemic vasculitis, and a reduced risk of deterioration in kidney function [10]. A recent KDIGO clinical guideline recommended that all CKD patients infected with HCV should be evaluated for antiviral treatment [4, 8, 10]. Interferon-free regimens should be applied in CKD patients because interferon-based therapy is associated with low efficacy (SVR rates of 37–41%), poor tolerability, and acute rejection of graft or allograft loss in kidney transplant recipients [8, 10, 32]. Ribavirin was also used with caution in CKD patients due to its proclivity to cause anemia [10].
DAA is the backbone of treatment for HCV infection in CKD patients. The choice of specific DAA regimens is based on HCV genotype, viral load, treatment history, drug interactions, GFR, liver fibrosis stage, and kidney or liver transplant candidacy [8]. All CKD patients also should undergo evaluation for HBV infection (hepatitis B surface antigen/HBsAg and anti-hepatitis B core/anti-HBc) before beginning DAA treatment [4, 10]. If hepatitis B surface antigen (HBsAg) is detected, HBV antiviral treatment should be considered to prevent HBV reactivation as a consequence of DAA treatment. If there is a history of resolved HBV infection, clinicians should monitor HBV reactivation during DAA treatment (using serial HBV DNA and liver function tests) [10].
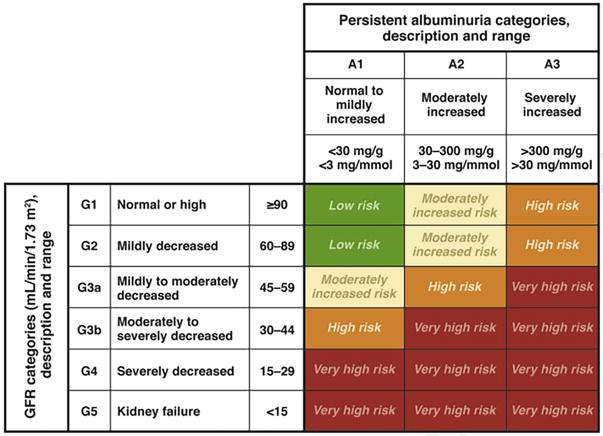
The classification of CKD is important to determine before starting DAA treatment. CKD is classified on the basis of cause, GFR category (G1 to G5), and albuminuria category (A1 to A3, presented as albumin-creatinine ratios). Figure A1 shows the classification and its prognosis, as used by KDIGO [10].
5.1 Treatment of HCV infection in patients with CKD GFR category G1 to G5 and G5D
The KDIGO and European Association for the Study of the Liver (EASL) recommended that patients with CKD G1-3b be treated with any licensed DAA regimens [4, 8, 10, 33]. No dose modification is necessary for most DAA regimens. Protease-inhibitors (telaprevir, boceprevir, simeprevir, paritaprevir, sovaprevir, asunaprevir, faldaprevir, glecaprevir) are contraindicated in liver cirrhosis patients because of risk of hepatic decompensation or hepatotoxicity [10]. Table 1 shows the treatment options for HCV infection in patients with CKD according to the KDIGO HCV in CKD guideline.
Kidney function
Regimen(s)
Strength of evidence
CKD G1-G3b
Any licensed DAA regimen
1A
CKD G4-G5, including HD
HCV genotypes 1
Grazoprevir/elbasvir
1B
Glecaprevir/pibrentasvir
1B
HCV genotypes 2
Glecaprevir/pibrentasvir
1B
HCV genotypes 3
Glecaprevir/pibrentasvir
1B
HCV genotypes 4
Grazoprevir/elbasvir
2D
Glecaprevir/pibrentasvir
1B
HCV genotypes 5
Glecaprevir/pibrentasvir
2D
HCV genotypes 6
Glecaprevir/pibrentasvir
2D
Table 1.
Treatment options for HCV infection in patients with CKD according to the KDIGO HCV in CKD guideline [8].
Recommendation grades (1 or 2) and strength of evidence (A to D) are provided for each recommended regimen and HCV genotype. Level 1, “we recommend”; level 2, “we suggest”. Grade A, high quality of evidence; B, moderate quality of evidence; C, low quality of evidence; D, very low quality of evidence [8].
KDIGO recommended that CKD patients with GFR below 30 mL/min/1.73 m2 (CKD G4-G5D) be treated with a ribavirin-free DAA-based regimen. For patients with CKD G4-G5D, the first-line treatment recommendation is either glecaprevir/pibrentasvir for all HCV genotypes or grazoprevir/elbasvir for genotypes 1 and 4. For patients with CKD G5 who are receiving PD, no evidence is available; therefore, following the proposed regimens for patients receiving HD is reasonable [8].
The EXPEDITION-4 study’s phase III trial found that using glecaprevir/pibrentasvir in 104 CKD G4-G5 patients resulted in SVR12 rate of 98% (SVR after 12 weeks post-treatment) [34]. In the nonrandomized multicenter EXPEDITION-5 study of CKD G3b-G5 patients with HCV infection, it was shown that glecaprevir/pibrentasvir treatment yielded a high SVR12 rate (97%) [35]. In a prospective study of the Japanese population assessing 8 or 12 weeks of glecaprevir/pibrentasvir treatment, SVR was achieved in 100% of patients with CKD G4, 99% of patients with CKD G5, and 99% of patients on HD [36]. A study about the safety and efficacy of glecaprevir/pibrentasvir in 2238 CKD patients with HCV infection genotype 1–6, reported an overall SVR rate of 98%, with no difference between CKD G1-G3 or G4-G5 [37].
Grazoprevir/elbasvir also demonstrated promising results in CKD patients. A randomized controlled trial of grazoprevir/elbasvir in CKD G4-G5 with HCV genotype 1, reported an SVR rate of 94% in patients who received immediate treatment and an SVR rate of 98% in patients with postponed treatment [38, 39]. In a quasi-experimental study of CKD G5D in Bandung (Indonesia), grazoprevir/elbasvir was effective in reducing liver fibrosis degree (based on the APRI score) [40].
5.2 HCV treatment for kidney transplant recipients
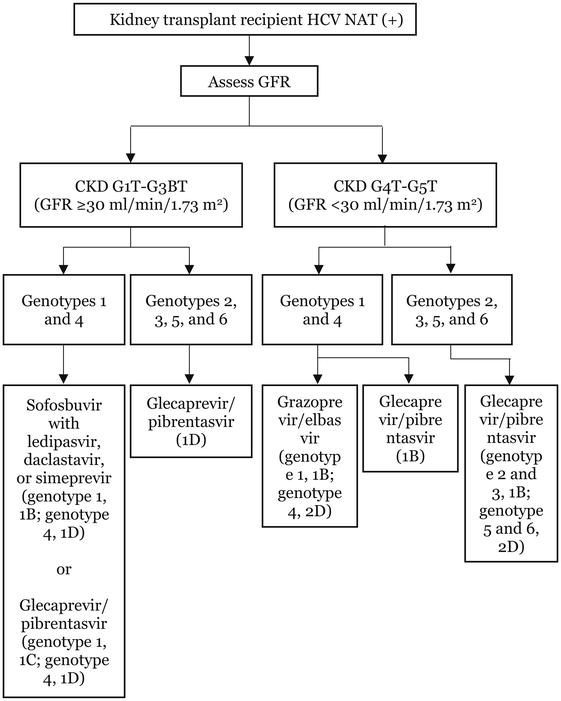
Kidney transplant recipients infected with HCV should be evaluated for treatment with a DAA-based regimen. The choice of DAA regimen should be based on HCV genotype and subtype, viral load, prior treatment history, drug interactions, GFR, stage of liver fibrosis, liver transplant candidacy, and comorbidities. Specific to drug–drug interactions, clinicians should do a pre-treatment assessment of the interaction between DAA and immunosuppressive drugs [8]. Drug interactions are an important issue in kidney transplant recipients, and DAA treatment could provoke the elevation or suppression of the immunosuppressive drug level in the blood, resulting in graft rejection or toxicity. Immunosuppressive drugs called calcineurin inhibitors (tacrolimus, cyclosporine), are metabolized by cytochrome P-450 [10]. In those receiving calcineurin inhibitors, monitoring of the calcineurin inhibitor level should be done [8]. Protease inhibitors DAA are associated with a significant risk of interaction with calcineurin inhibitors. Non-structural protein 5A/NS5A inhibitors (ledipasvir, daclastavir) and non-structural protein 5B/NS5B inhibitors (sofosbuvir) are associated with a lower risk of interaction with calcineurin inhibitors. Concurrent use of elbasvir-grasoprevir with cyclosporine is not recommended because it increases the area under the curve for grazoprevir by 15-fold and that for elbasvir by 2-fold. Grazoprevir/elbasvir could induce an elevation of tacrolimus levels by 43%. On the other hand, protease inhibitors do not interact with mycophenolate mofetil [10]. Figure 1 shows the algorithm of DAA treatment in kidney transplant recipients.
Figure 1.
Treatment scheme for kidney transplant recipients. Recommendation grades (1 or 2) and strength of evidence (A to D) are provided for each recommended regimen and HCV genotype. Sofosbuvir/velpatasvir-based regimens may be considered in kidney transplant recipients with GFR ≥ 30 mL/min/1.73 m2 given their availability in certain jurisdictions. T suffix in GFR categories (e.g., G1T) denotes transplant recipient [8].
According to one study, DAA treatment achieved SVR rates of more than 95% in kidney transplant recipients [8]. Evidence showed that glecaprevir/pibrentasvir treatment in kidney and liver transplant recipients could achieve an overall SVR of 98% [41]. For patients with GFR ≥30 mL/min/1.73 m2, a sofosbuvir-based regimen has been added to the therapeutic options. A previous study discovered that kidney transplant recipients with GFR ≥ 40 mL/min/1.73 m2 had a 100% SVR after receiving the sofosbuvir/ledipasvir regimen [42]. Lai and colleagues [42] reported that grazoprevir/elbasvir for 12 weeks is highly effective in genotype 1b HCV-infected liver and kidney transplant recipients [43].
5.3 Management of patients with HCV infection, before and after kidney transplantation
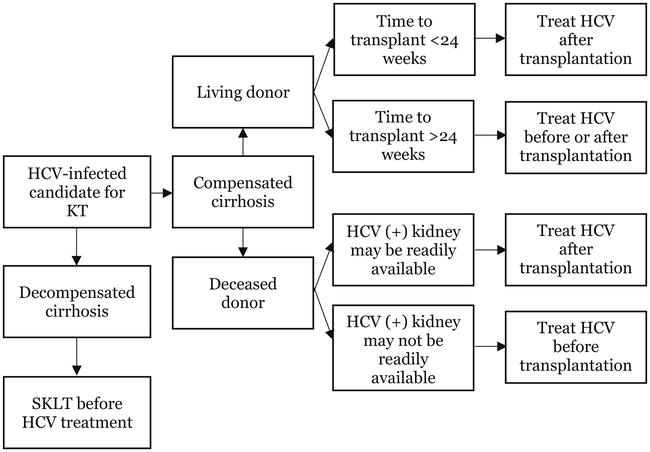
HCV infection in potential kidney transplant recipients can be treated before or after kidney transplantation [10, 44, 45]. The timing of DAA treatment depends on donor type, wait list times, HCV genotypes, transplantation center-specific policies, and the degree of liver fibrosis. For deceased donors, KDIGO recommends that kidney from HCV NAT-positive donors be directed to kidney transplant recipients who are NAT-positive. But, if acceptance of a graft from HCV NAT-positive donor could reduce the wait time for transplantation, patients could undergo transplantation with an HCV-positive kidney and get DAA treatment after transplantation [10, 44]. On the other side, HCV NAT-positive living donors should be treated and SVR should be confirmed before transplantation, as long as the patients have no evidence of cirrhosis [8, 46]. Figure 2 shows the HCV treatment algorithm in kidney transplant candidates.
5.4 Sofosbuvir-based regimen in HCV-infected patients with CKD GFR category G4-G5D
Although alternative DAA (glecaprevir/pibrentasvir and grazoprevir-elbasvir) had already been approved for advanced CKD patients, a need for safety and efficacy data on sofosbuvir-based regimens remained, due to limited access to those alternative DAA in some countries and the risks associated with the use of protease-inhibitor containing regimens in patients with advanced fibrosis or cirrhosis. As a consequence of this phenomenon, sofosbuvir-based regimens were being administered off-label to patients with ESRD, including those undergoing HD. AASLD currently recommends all DAAs for GFR ≤ 30 mL/min [15]. US Food and Drug Administration (FDA) also approved the use of three sofosbuvir-based regimens (sofosbuvir/ledipasvir, sofosbuvir-velpatasvir, and sofosbuvir-velpatasvir-voxilaprevir) in patients with GFR below 30 mL/min [45].
Sofosbuvir, a non-structural N5B polymerase inhibitor, was approved in 2013 and is now the backbone of many DAA regimens, enhancing the cure bar above 90% [47, 48, 49]. Sofosbuvir has large renal excretion and has been initially licensed for patients with GFR of more than 30 mL/min [12, 13, 14]. According to the KDIGO guidelines, sofosbuvir-based regimen is not indicated on label in CKD patients with GFR ≤ 30 mL/min [44]. The circulating metabolite of sofosbuvir, GS-331007, is primarily eliminated by the kidney and accumulates up to 5- to 20-fold in patients with severe kidney impairment or ESRD, respectively [50]. It is still unclear about the association between the increased concentration of GS-331007 and renal toxicity. There were case reports that revealed acute interstitial nephritis in sofosbuvir/ledipasvir [51] and sofosbuvir/daclastavir [52] consumption, in the setting of CKD. Unfortunately, kidney injury has not been reported in a larger clinical trial of sofosbuvir [45].
Several studies have reported the efficacy and safety of sofosbuvir-based regimens in those with GFR ≤30 mL/min. A real-life multicenter retrospective cohort study on 4944 chronic HCV patients with CKD, reported that sofosbuvir-based regimens are effective and safe for treating patients with severe CKD and those with associated hepatic decompensation. In this study, SVR12 was achieved in 96.7% of patients with severe renal impairment [53].
A multicenter, prospective, single-center study of patients undergoing HD evaluated full-dose sofosbuvir once daily or three times weekly paired with simeprevir, daclastavir, ledipasvir, or ribavirin. A sofosbuvir-based regimen was administered after HD, and they reported that GS-331007 did not accumulate between dialysis sessions or during therapy. SVR12 or SVR24 was achieved in 83% of subjects, and no serious adverse events (SAE) occurred (including cardiac events) [54].
An observational study in patients on HD in Rabat (Morocco) revealed a 100% SVR after being treated with sofosbuvir (400 mg) and daclastavir (60 mg), three times per week (after HD session). None of them had side effects or developed hepatobiliary and cardiac toxicity. There were fatigue and headache side effects, but the symptoms disappeared after the end of treatment [55].
In Jinnah Hospital in Lahore, Pakistan, a prospective open-label, parallel, non-randomized interventional trial was conducted in 36 patients with HCV on maintenance HD. The subjects were enrolled and then equally allocated in 1:1 ratio to group 1 who received 400 mg daily sofosbuvir/60 mg daily daclatasvir and group 2 who received three times per week of 400 mg sofosbuvir and daily 60 mg daclatasvir for 12 weeks. Patients with compensated liver cirrhosis got therapy for 24 weeks. They reported that sofosbuvir/declatsavir is highly effective and tolerable in patients with HCV genotype 1 & 3 undergoing HD, especially when given daily [56].
A phase II clinical trial (single-arm study) looked at the treatment response of 59 patients with genotype 1–6 HCV infection and ESRD who were on HD (92%) or PD (8%) at the time. All patients received sofosbuvir/velpatasvir (400/100 mg) once daily for 12 weeks. About 32% of patients had kidney transplant before and 29% of patients had liver cirrhosis. After 12 weeks, 56 of 59 patients achieved SVR (95%; 95% CI 86–99%). SAE was reported for 19% of patients, and all were deemed to be unrelated to the DAA regimen [57].
The efficacy and safety of sofosbuvir-based regimens in CKD patients with GFR category G4-G5D were also revealed by systematic review and meta-analysis. Li et al. [2] analyze 21 studies in which HCV patients with stage 4 or 5 CKD received sofosbuvir-based therapy. In total 717 patients were enrolled, including 58.4% HD patients or PD recipients. Pooled SVR12/24 was 97.1% and the SAE rate was 4.8%. There was no significant difference at SVR12/24 (97.1 vs. 96.2%, p = 0.72) or SAE rate (8.8 vs. 2.9%, p = 0.13) between subgroups applying the full or decreased dose of sofosbuvir. Patients with and without liver cirrhosis achieved comparable SVR (RR 0.93, 95% CI 0.85–1.02).
A systematic review and meta-analysis by Fabrizi et al. [12] showed that sofosbuvir-based regimens were safe and effective in patients with CKD stages 4–5. Thirty clinical studies were retrieved, then the pooled SVR12 and SAE rates were 0.99 (95% CI, 0.97;1.0, I2 = 99.8%) and 0.09 (95% CI, 0.05;0.13, I2 = 84.3%), respectively. The pooled drop-out rate due to adverse events was 0.02 (95% CI, −0.01;0.04, I2 = 16.1%). Reduced GFR was found in 14.19% of patients, and 26.38% of patients got anemia. SAE were common in full-dose sofosbuvir and ribavirin-based regimens.
Another systematic review and meta-analysis of 20 studies also suggested that sofosbuvir-based regimens for HD patients were effective and safe. The efficacy of the sofosbuvir-based regimen was 92% (95% CI 80–99%), 98% (95% CI 96–100%), and 100% (95% CI 95–100%) for the following doses: 400 mg on alternate days, 400 mg daily, and 200 mg daily, respectively. Among the studies that reported adverse events, anemia was the most common, with a pooled prevalence of 15% [58].
Effective detection, evaluation, and treatment for HCV infection can improve kidney and cardiovascular outcomes in CKD patients. Several studies have found an association between SVR and a reduction in ESRD-related mortality, a reduction in vascular events, an improvement in cryoglobulinemic vasculitis, and a reduced risk of deterioration in kidney function. The development of DAAs enabled a greater rate of HCV eradication in CKD patients. Any licensed DAA regimen can be used in patients with CKD G1-G3b. The recommended DAA regimens for CKD G4–5D, are the sofosbuvir-free combination therapies (grazoprevir/elbasvir and glecaprevir/pibrentasvir). While KDIGO did not recommend sofosbuvir-based regimens as the drug of choice in patients with CKD G4–5D, data from multiple studies have demonstrated the effectiveness and safety of sofosbuvir-based regimens in CKD G4-G5D. Currently, AASLD and the US FDA have approved the use of sofosbuvir-based regimens in CKD G4-G5D patients.
The authors would like to express gratitude for the support of all medical staff from the Gastroenterohepatology Division, Internal Medicine Department, Faculty of Medicine, Udayana University/Prof. I.G.N.G. Ngoerah General Hospital.
Current CKD classification used by KDIGO guideline [10].
References
1.Liu CH, Kao JH. Pan-genotypic direct-acting antivirals for patients with hepatitis C virus infection and chronic kidney disease stage 4-5. Hepatology International. 2022;16:1001-1019. DOI: 10.1007/s12072-022-10390-z
2.Li M, Chen J, Fang Z, et al. Sofosbuvir-based regimen is safe and effective for hepatitis C infected patients with stage 4-5 chronic kidney disease: A systematic review and meta-analysis. Virology Journal. 2019;16:1-11. DOI: 10.1186/s12985-019-1140
3.Cottone C, Bhamidimarri KR. Evaluating CKD/ESRD patient with hepatitis C infection: How to interpret diagnostic testing and assess liver injury. Seminars in Dialysis. 2019:1-8. DOI: 10.1111/SDI.12760
4.Li PKT, Bavanandan S, Mohamed R, et al. 2018 Kidney disease: Improving global outcomes (KDIGO) hepatitis C in chronic kidney disease guideline implementation: Asia summit conference report. Kidney International Reports. 2020;5:1129-1138. DOI: 10.1016/j.ekir.2020.05.001
5.Fabrizi F, Martin P, Dixit V, et al. Post-transplant diabetes mellitus and HCV seropositive status after renal transplantation: Meta-analysis of clinical studies. American Journal of Transplantation. 2005;5(10):2433-2440. DOI: 10.1111/j.1600-6143.2005.01040.x
6.Burra P, Buda A, Livi U, et al. Occurrence of post-transplant lymphoproliferative disorders among over thousand adult recipients: Any role for hepatitis C infection? European Journal of Gastroenterology & Hepatology. 2006;18(10):1065-1070. DOI: 10.1097/01.meg.0000231752.50587.ae
7.Baid-Agrawal S, Farris AB, Pascual M, et al. Overlapping pathways to transplant glomerulopathy: Chronic humoral rejection, hepatitis C infection, and thrombotic microangiopathy. Kidney International. 2011;80(8):879-885. DOI: 10.1038/ki.2011.194
8.Gordon CE, Berenguer MC, Doss W, et al. Prevention, diagnosis, evaluation, and treatment of hepatitis C virus infection in chronic kidney disease: Synopsis of the kidney disease: Improving global outcomes 2018 clinical practice guideline. Annals of Internal Medicine. 2019;171(7):496-457. DOI: 10.7326/M19-1539
9.Shin HP, Park JA, Burman B, et al. Efficacy and safety of sofosbuvir-based regimens for treatment on chronic hepatitis C genotype 1 patients with moderately impaired renal function. Clinical and Molecular Hepatology. 2017;23:316-322. DOI: 10.3350/cmh.2016.0087
10.Awan AA, Jadoul M, Martin P. Hepatitis C in chronic kidney disease: An overview of the KDIGO guideline. Clinical Gastroenterology and Hepatology. 2019;18(10):2158-2167. DOI: 10.1016/J.CGH.2019.07.050
11.World Health Organization (WHO). Accelerating access to hepatitis C diagnostics and treatment: Overcoming barriers in low- and middle-income countries. In: Global Progress Report 2020. Geneva: World Health Organization; 2021
12.Fabrizi F, Cerutti R, Dixit V, et al. Sofosbuvir-based regimens for HCV in stage 4-stage 5 chronic kidney disease. A systematic review with meta-analysis. Nefrología. 2021;41(5):578-589. DOI: 10.1016/j.nefroe.2021.11.011
13.Desnoyer A, Pospai D, Gervais MP, et al. Sofosbuvir-containing regimen for HCV infection in hemodialysis patients: 400 mg daily or only on the day of hemodialysis. Journal of Hepatology. 2016;65(1):40-47. DOI: 10.1016/J.HEP.2016.02.044
14.Sise MF, Backman E, Ortiz GA, et al. Effect of sofosbuvir-based hepatitis C virus therapy on kidney function in patients with CKD. Clinical Journal of the American Society of Nephrology. 2017;12:1615-1623. DOI: 10.2215/CJN.02510317
15.AASLD-IDSA HCV Guidance Panel. Hepatitis C guidance: AASLD-IDSA recommendations for testing, managing, and treating hepatitis C; 2020. Available from: https://www.hcvguidelines.org/unique-populations/renal-impairment [Last update: 27.08.20]
16.Azmi AN, Tan SS, Mohamed R. Hepatitis C and kidney disease: An overview and approach to management. World Journal of Hepatology. 2015;7(1):78-92. DOI: 10.4254/WJH.V7.i1.78
17.Jadoul M, Bieber BA, Martin P, et al. Prevalence, incidence, and risk factors for hepatitis C virus infection in hemodialysis patients. Kidney International. 2019;95:939-947. DOI: 10.1016/j.kint.2018.11.038
18.Liu CH, Kao JH. Treatment of hepatitis C virus infection in patients with end stage renal disease. Journal of Gastroenterology and Hepatology. 2011;26:228-239. DOI: 10.1111/j.1440-1746.2010.06488.x
19.World Health Organization. Global hepatitis report; 2017. Available from: https://www.who.int/publications/i/item/global-hepatitis-report-2017. [Accessed 30 November 2022]
20.Yuki N, Ishida H, Inoue T, et al. Reappraisal of biochemical hepatitis C activity in hemodialysis patients. Journal of Clinical Gastroenterology. 2000;30:187-194. DOI: 10.1097/00004836-200003000-00012
21.Lopes EP, Gouveia EC, Albuquerque AC, et al. Determination of the cut-of value of serum alanine aminotransferase in patients undergoing hemodialysis, to identify biochemical activity in patients with hepatitis C viremia. Journal of Clinical Virology. 2006;35:298-302. DOI: 10.1016/J.JCV.2005.09.010
22.Milotic I, Pavic I, Maleta I, Troselj-Vukic B, Milotic F. Modified range of alanine aminotransferase is insufficient for screening of hepatitis C virus infection in hemodialysis patients. Scandinavian Journal of Urology and Nephrology. 2002;36:447-449. DOI: 10.1080/003655902762467611
23.Lai TS, Lee MH, Yang HI, et al. Hepatitis C viral load, genotype, and increased risk of developing end-stage renal disease: REVEAL-HCV study. Hepatology. 2017;66:784-793. DOI: 10.1002/hep.29192
24.Lai TS, Lee MH, Yang HI, et al. High hepatitis C viral load and genotype 2 are strong predictors of chronic kidney disease. Kidney International. 2017;92:703-709. DOI: 10.1016/j.kint.2017.03021
25.de Paula FK, Carmo RA, de Figueiredo Antunes CM, et al. HCV genotypes and hepatic siderosis in patients with chronic renal failure on haemodialysis in Brazil. Nephrology, Dialysis, Transplantation. 2007;22:2027-2031. DOI: 10.1093/ndt/gfm028
26.Greeviroj P, Lertussavavivat T, Thongsricome T, et al. The world prevalence, associated risk factors and mortality of hepatitis C virus infection in hemodialysis patients: A meta-analysis. Journal of Nephrology. 2022;35:2269-2282. DOI: 10.1007/s40620-022-01483-x
27.Fabrizi F, Dixit V, Messa P. Hepatitis C virus and mortality among patients on dialysis: A systematic review and meta-analysis. Clinics and Research in Hepatology and Gastroenterology. 2019;43(3):244-254. DOI: 10.1016/j.clinre.2018.10.009
28.Fabrizi F, Martin P, Dixit V, et al. Meta-analysis of observational studies: Hepatitis C and survival after renal transplant. Journal of Viral Hepatitis. 2014;21:314-324. DOI: 10.1111/jvh.12148
29.Marinaki S, Boletis JN, Sakellariou S, et al. Hepatitis C in hemodialysis patients. World Journal of Hepatology. 2015;7(3):548-558. DOI: 10.4254/wjh.v7.i3.548
30.Hinrichsen H, Leimenstoll G, Stegen G, et al. Prevalence and risk factors of hepatitis C virus infection in hemodialysis patients: A multicenter study in 2796 patients. Gut. 2002;51(3):429-433. DOI: 10.1136/gut.51.3.429
31.Liu CH, Liang CC, Huang KW, et al. Transient elastography to assess hepatic fibrosis in hemodialysis chronic hepatitis C patients. Clinical Journal of the American Society of Nephrology. 2011;6(5):1057-1065. DOI: 10.2215/cjn.04320510
32.Kamar N, Ribes D, Izopet J, et al. Treatment of hepatitis C virus infection (HCV) after renal transplantation: Implication for HCV-positive dialysis patients awaiting a kidney transplant. Transplantation. 2006;82:853-856. DOI: 10.1097/01.tp.0000238898.14393.c9
33.European Association for the Study of the Liver (EASL). EASL recommendations on treatment of hepatitis C: Final update pf the series. Journal of Hepatology. 2020;73:1170-1218. DOI: 10.1016/j.jhep.2020.08.018
34.Gane E, Lawitz E, Pugatch D, et al. Glecaprevir and pribentasvir in patients with HCV and severe renal impairment. NEJM. 2017;377:1448-1455. DOI: 10.1056/NEJMoa1704053
35.Lawitz E, Flisiak R, Abunimeh M, et al. Efficacy and safety of glecaprevir/pibrentasvir in renally impaired patients with chronic HCV infection. Liver International. 2020;40:1032-1041. DOI: 10.1111/liv.14320
36.Atsukawa M, Tsubota A, Toyoda H, et al. The efficacy and safety of glecaprevir plus pibrentasvir in 141 patients with severe renal impairment: A prospective, multicenter study. Alimentary Pharmacology & Therapeutics. 2019;49:1230-1241. DOI: 10.1111/apt.15218
37.Pol S, Pockros P, Pugatch D, et al. Safety and efficacy of glecaprevir/pibrentasvir in adults with chronic hepatitis C virus infection genotype 1-6 and chronic kidney disease: An integrated analysis. Journal of Hepatology. 2017;66(Suppl. 1):S738. DOI: 10.1016/s0168-8278(17)31967-0
38.Roth D, Nelson DR, Bruchfeld A, et al. Grazoprevir plus elbasvir in treatment-naïve and treatment-experienced patients with hepatitis C virus genotype 1 infection and stage 4-5 chronic kidney disease 9 the C-SURFER study: A combination phase 3 study. Lancet. 2015;386:1537-1545. DOI: 10.1016/S0140-6736(15)00349-9
39.Bruchfeld A, Roth D, Martin P, et al. Elbasvir plus grazoprevir in patients with hepatitis C virus infection and stage 4-5 chronic kidney disease: Clinical, virological, and health-related quality-of-life outcomes from a phase 3, multicentre, randomised, double-blind, placebo-controlled trial. The Lancet Gastroenterology & Hepatology. 2017;2:585-594. DOI: 10.1016/S2468-1253(17)30116-4
40.Laksono B, Agustanti N, Supriyadi R, et al. Reduction of liver fibrosis after treatment with elbasvir/grazoprevir in patients with hepatitis C infection in chronic kidney disease on hemodialysis, a quasi-experimental study. The Indonesian Journal of Gastroenterology Hepatology and Digestive Endoscopy. 2021;22(1):21-28. DOI: 10.24871/221202121-28
41.Reau N, Kwo PY, Rhee S, et al. Glecaprevir/pibrentasvir treatment in liver or kidney transplant patients with hepatitis C virus infection. Hepatology. 2018;68:1298-1307. DOI: 10.1002/hep.20046
42.Colombo M, Aghemo A, Liu H, et al. Treatment with ledipasvir sofosbuvir for 12 or 24 weeks in kidney transplant recipients with chronic hepatitis C virus genotype 1 or 4 infection: A randomized trial. Annals of Internal Medicine. 2017;166:109-117. DOI: 10.7326/M16-1205
43.Lai PC, Chen CH, Jeng LB, et al. Grazoprevir/elbasvir treatment in liver or kidney transplant recipients with genotype 1b hepatitis C virus infection. Antimicrobial Agents and Chemotherapy. 2022;66(2):1-9. DOI: 10.1128/AAC.02003-21
44.Kidney Disease: Improving Global Outcomes Hepatitis CWG. KDIGO 2018 clinical practice guideline for the prevention, diagnosis, evaluation, and treatment of hepatitis C in chronic kidney disease. Kidney International Supplements;2018(8):91-165
45.Sise ME, McQuaid T, Martin P. Sofosbuvir-based hepatitis C therapies in patients with chronic and end-stage kidney disease. Nephrology, Dialysis, Transplantation. 2021;1:1-8. DOI: 10.1093/ndt/gfab072
46.Hart A, Smith JM, Skeans MA, et al. OPTN/SRTR 2016 annual data report: Kidney. American Journal of Transplantation. 2018;18(Suppl 1):18-113. DOI: 10.1111/ajt.14557
47.Afdhal N, Zeuzem S, Kwo P, et al. Ledipasvir and sofosbuvir for untreated HCV genotype 1 infection. The New England Journal of Medicine. 2014;370(20):1889-1898. DOI: 10.1056/NEJMoa1402454
48.Feld JJ, Jacobson IM, Hezode C, et al. Sofosbuvir and Velpatasvir for HCV genotype 1, 2, 4, 5, and 6 infection. The New England Journal of Medicine. 2015;373(27):2599-2607. DOI: 10.1056/NEJMoa1512610
49.Lawitz E, Mangia A, Wyles D, et al. Sofosbuvir for previously untreated chronic hepatitis C infection. The New England Journal of Medicine. 2013;368(20):1878-1887. DOI: 10.1056/NEJMoa1214853
50.Kirby BJ, Symonds WT, Kearney BP, et al. Pharmacokinetic, pharmacoynamic, and drug-interaction profile of the hepatitis C virus NS5B polymerase inhibitor sofosbuvir. Clinical Pharmacokinetics. 2015;54:677-690. DOI: 10.1007/S40262-015-0261-7
51.Wanchoo R, Thakkar J, Schwartz D, et al. Harvoni (ledipasvir with sofosbuvir)-induced renal injury. The American Journal of Gastroenterology. 2016;111:148-149. DOI: 10.1038/ajg.2015.391
52.Ashraf T, Majoni W. Acute interstitial nephritis associated with sofosbuvir and daclastavir. ACG Case Reports Journal. 2017;4:e84. DOI: 10.14309/crj.2017.84
53.Eletreby R, El Serafy M, Anees M, et al. Sofosbuvir-containing regimens are safe and effective in the treatment of HCV patients with moderate to severe renal impairment. Liver International. 2019;00:1-9. DOI: 10.1111/liv.14299
54.Desnoyer A, Pospai D, Le MP, et al. Pharmacokinetics, safety and efficacy of a full dose sofosbuvir-based regimen given daily in hemodialysis patients with chronic hepatitis C. Journal of Hepatology. 2016;65:40-47. DOI: 10.1016/j.jhep.2016.02.044
55.Tamzaourte M, Zajjari Y, Berrag S, et al. Safety and efficacy of sofosbuvir based regimen in the treatment of hepatitis C virus infection among hemodialysis patients in Morocco. Journal of Clinical Nephrology. 2021;5:077-080. DOI: 10.29328/journal.jcn.1001078
56.Cheema SUR, Rehman MS, Hussain G, et al. Efficacy and tolerability of sofosbuvir and daclatasvir for treatment of hepatitis C genotype 1 & 3 in patients undergoing hemodialysis - A prospective interventional clinical trial. BMC Nephrology. 2019;20:1-8. DOI: 10.1186/s12882-019-1631-4
57.Borgia SM, Dearden J, Yoshida EM, et al. Sofosbuvir/velpatasvir for 12 weeks in hepatitis C virus-infected patients with end-stage renal disease undergoing dialysis. Journal of Hepatology. 2019;71:660-665. DOI: 10.1016/j.jhep.2019.05.028
58.Shehadeh F, Kaliigeros M, Byrd K, et al. Efficacy and safety of sofosbuvir in the treatment of hep C among patients on hemodialysis: A systematic review and meta-analysis. Scientific Reports. 2020;10:1-10. DOI: 10.1038/S41598-020-71205-5
Written By
Gde Somayana and Komang Agus Wira Nugraha
Submitted: 29 December 2022Reviewed: 30 December 2022Published: 15 May 2023
 Open access peer-reviewed chapter
Open access peer-reviewed chapter