Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
To purchase hard copies of this book, please contact the representative in India:
CBS Publishers & Distributors Pvt. Ltd.
www.cbspd.com
|
customercare@cbspd.com
Autoimmune Rheumatic Diseases (ARDs) are chronic multisystemic diseases that have a low prevalence (estimated to range from 4 to 5% of the general population), and the impact on mortality in ARDs is lower (mortality reported in ARDs is 0.3 to 2.1) in general statistics worldwide compared to other diseases with higher prevalence such as arterial hypertension (HBP) or diabetes mellitus (DM). The objective of this review is to update the concepts regarding mortality associated with ARD, and the most relevant studies and review were included. The causes of mortality among ARDs vary widely between geographic areas and cannot be generalized, although the most important frequency reported is in rheumatoid arthritis (RA), systemic lupus erythematosus (SLE) and scleroderma (SSc). It has recently been reported that measuring the standardized mortality rate (SMR) identifies the inflammatory diseases with increased risk: 4.80 in systemic vasculitis (SV), 2.9 in SLE, and 1.44 in RA. The causes of death are regularly associated with acute events (infections and respiratory and cardiovascular diseases) and less frequent related to the disease severity. Other reported associated factors have been age, duration, type of presentation of the disease, and socioeconomic status. We found that the variation between the main reported causes is little; significantly higher mortality (five times more) has been found in the regional analysis in Latin America compared to that in Europe. The most important factor in the last decades is the habitual use of drugs that increase the risk of immunosuppression and infection.
Internal Medicine Department, Rheumatology Unit - Roosevelt Hospital, Post Graduate School of San Carlos University of Guatemala, Guatemala
*Address all correspondence to: drherreram@gmail.com
1. Introduction
Autoimmune rheumatic diseases have a low prevalence of associated mortality (0.3 to 2.1) [1]. When the mortality of ARDs is compared with more prevalent diseases (DM and BHP), the statistical impact is lower worldwide, and consequently, the study of its causes has been limited.
The objective of this review is to update the concepts on mortality associated with ARD, and we searched for studies of the last 50 years in the main databases (Pubmed, Cochrane, Google academic, and Scopus) using the words autoimmune disease, rheumatic disease, and mortality in autoimmune disease and then looking for causes of mortality in VS, SLE, and RA.
The information analyzed comes from databases of better organized institutions and complemented with the analysis of studies that describe in detail the causes of mortality in the different latitudes; sixty-five reports (cases, observational studies, and database analysis) of mortality and rheumatic disease were reviewed, including at the end 25 that contain the most important information.
Recently was informed that measure the standardized mortality ratio risk identified at population in risk. In general terms, the group of rheumatic diseases has a risk of 2.03 (95% CI: 1.79–2.29) and has been reported particularly for those considered as inflammatory. The highest risk reported was 4.80 in systemic vasculitis, followed by 2.9 in systemic lupus erythematosus and 1.44 in rheumatoid arthritis [2].
Some studies also report that patients with diseases such as Myositis (MI), SSc, and Sjogren’s syndrome (SS) may have a significant risk, which is not yet considered among the most important because its prevalence is lower.
The causes of death are regularly associated with acute events, infections, cardiovascular and lung diseases, and a lower probability with the clinical spectrum of the disease.
Other related factors reported are age and duration of the disease, the severity of presentation, and the adverse effects relating to the treatment administered [3, 4, 5]. The comorbidities, specialty cardiovascular, metabolic, and respiratory are the most important [6, 7, 8].
Most recently, use of novelty pharmacies (monoclonal antibodies, Jak inhibitors) in combination with glucocorticoids and immunosuppressive drugs has been proposed as the factor that increases the risk [9, 10, 11, 12]. However, it should be noted that thanks to this therapeutic innovation, ARD patients have improved their quality and life expectancy.
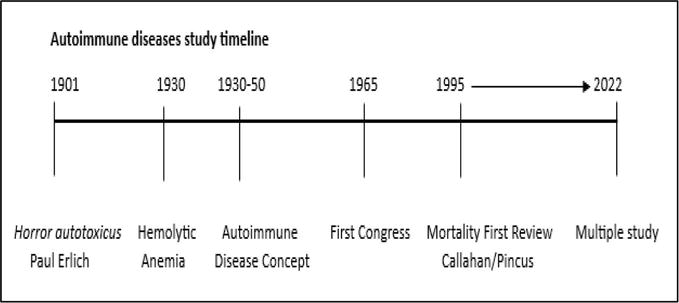
The notion of autoimmune diseases in humans’ dates to the beginning of the 20th century, and currently, more than 40 human diseases have been described that could have this name.
The first widely described autoimmune disease with underlying pathophysiological mechanisms was Hemolytic Anemia, described in 1925 by Lederle [13]. However, autoimmune diseases were not officially recognized as such until the 1940s–50s, and until then, the reports on mortality in these diseases were scarce. The first congress on these diseases was held in 1965.
In this line of time (Figure 1), the main events related to autoimmune diseases are identified.
Figure 1.
Line of time.
2.2 Background
The study of rheumatic diseases focused on morbidity, loss of function, instability caused by joint damage, and reduced quality of life. Nonetheless, in 1955, it was estimated that the 5-year survival in patients with SLE, vasculitis, and polymyositis was only 5%, and it was considered part of the “natural history” of the disease; it was considered that the systemic inflammatory process and the progression of disease were the cause of death [14].
As early as 1953, Cobb et al. described the course of death in 130 patients with rheumatoid arthritis who were followed for nine years. The first cause of death reported in 25% was infection, 24% heart disease and 13% various forms of nephropathy [15]; besides, in similar study, Mitchell reported a decrease in 5–15 years life expectancy in this patient [16].
In 1976, Urowitz and his collaborators suggested bimodality as the cause of death in SLE: 1. Early death with an active disease that requires high doses of glucocorticoids is regularly associated with infections and 2. A late death in an inactive disease, which has required many years of glucocorticoid intake and whose outcome is heart disease [17].
2.3 Current development in mortality trends
Due to the wide variation in mortality in rheumatic diseases, it has been necessary to develop precise and weighted analyses that calculate the risk; one of them is the SMR. This is obtained by calculating the relationship between the deaths observed in a cohort and those expected in a group of the same size from the general population (in the same area and standardized by age and sex).
Toledano et al. measured the SMR in rheumatic diseases and performed a meta-analysis in 2012, finding 32 studies that were analyzed (16 in RA, 7 in SC, 5 in SLE, and 2 in Vasculitis). They reported that the highest risk is in inflammatory diseases, vasculitis 4.8, SLE 2.9, and RA 1.4, and reported that the leading cause of mortality is cardiovascular diseases, followed by pulmonary, renal, and infectious diseases [2]. In ARDs with an inflammatory component, SMR 2.03 is higher and becomes evident when compared with that of fibromyalgia, an entity without an inflammatory burden, with 0.49 [18].
Recently, in 2020, Scherlinger and collaborators have carried out a review of the mortality of rheumatic diseases between 2001 and 2014; the six main diseases, SLE, SSC, MI, SS, Vasculitis, and MCTD (mixed connective tissue disease), reported according to the World Health Organization were included. The number of deaths per million inhabitants was estimated using the ASMR (aged-standardized mortality rate), with the most important data being SLE 2.68 and SSc 1.48. The following were reported during 2014 (reports from 35 to 85 countries): 6418 deaths in SLE, 4287 in SSc, 1313 in MI, 438 in SS, 235 in MCTD, and 1350 in Vasculitis [19].
It is found that the ASMR is up to five times higher in the countries of Latin America compared to the in the countries of Europe, not finding this relationship with countries of other continents [19]. This could be related to inequity in the provision of medical care and the quality of health services in each of the countries that consistently report mortality.
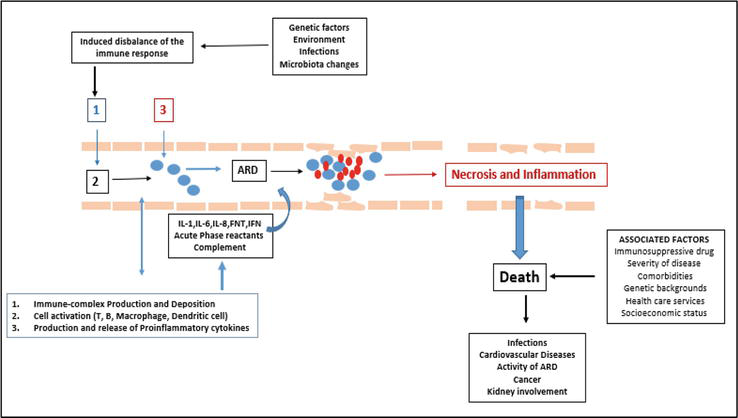
ARDs are a heterogeneous group of diseases, characterized by an immune dysregulation resulting in inflammation and multi-organ involvements that can conditioned the died.
The immune dysregulation involves tissues, cells, and molecules that usually participated in immune response, especially against infectious agents [20].
Usually factors involved in this dysregulation are several: Ambiental, genetic, infectious diseases, and most recent changes in the microbiome and hygienic hypothesis.
Because of this initial stimulus, the immune response has become unbalanced, and our own tissues become the target of action, named horror autotoxicus for Paul Erlich in 1901 [20].
This imbalance is reflected in the different pathways that participate in the immune response, which react to the presence of an “autoantigen” that is not recognized as their own (loss of self-tolerance), because the peptide sequences are similar and can be confused with those of foreign agents.
3.2 Hypothesis and ARD development
In recent years, different hypotheses have been accepted as triggers for an autoimmune disease; the most important are [21]: Exposure of cryptic antigens, overexpression of MHC (Major Histocompatibility Complex) and costimulatory molecules, neoantigen (microorganism + self-antigen), super antigen (polyclonal activation of T lymphocytes), and molecular mimicry.
Initially, the autoantigen is caught for antigen presenting cells (APC) and presented to the T cells in the thymus, in response the most autoreactive T cells that undergo apoptosis, but a small percentage of them enter the general circulation and escape the usual controls: clonal anergy (in peripheral lymphoid tissue), phenomenon of suppression by Treg cells and immunological ignorance (whose mechanisms are still unknown).
These reactive T cells are responsible for activating B cells that produce and release specific antibodies and proinflammatory cytokines, which in turn are responsible for amplifying inflammation and triggering the phenomena of tissue destruction and the systemic manifestations of autoimmune diseases, which can be perpetuated and cause death of the patient [21].
Figure 2 illustrates the process of generalized inflammation, with the possible triggers for an ARD and the factors that contribute to death as the outcome. Timely therapeutic intervention (pharmacological or non-pharmacological) can change the outcome.
In recent years, data collection through population-based studies has increased; it is the most widely used method for analyzing the prevalence of comorbidities.
However, it is pertinent in the analysis to establish that it requires considerable resources and the self-filling of documents by the patients, which implies the probability of making errors in the identification of the main pathologies, especially in the case of ARDs, which are diseases with great clinical and complex heterogeneity.
The report of various studies has assessed the co-occurrence of ARD with other diseases at the time of death, regularly using death certificate data, among the most frequent is include to cardiovascular diseases, pulmonary disorders, coagulation and hemorrhagic disorders, and renal failure.
We have reported in our center the mortality-associated comorbidities in ARD; those of the highest prevalence were HBP at 38.9% and DM type II at 11.3%. Specifically, in SLE, 50% reported HBP, 8.7% antiphospholipid syndrome (APS) associated with thrombosis, and 6.5% chronic kidney disease (CKD). In RA, the main association was HBP in 26.9% and DM-II in 23% of cases. In 24.3%, no comorbidity was reported [22].
These data are like those reported by another investigators: Panoulas et al. and Petri et al. reported in RA and SLE the double the prevalence of HBP in comparison with the general population [6, 7].
Sabio et al. reported HBP in 40% of patients with SLE compared with the 11% of controls of the same age [8].
Other authors also include minor comorbidities, musculoskeletal disease, genitourinary system, blood diseases, and diseases of the skin and subcutaneous tissue, and confirm the classic cause, cardiovascular diseases (55.5%), followed by diseases of the respiratory system (35.9%), endocrine and metabolic disorders (21.6%), and neoplasms (20.9%) [23].
4.2 Analysis of identified risks
The vascular compromise suggested the close relationship between the constant inflammatory states that affect the blood vessels, especially in the heart, kidney, and the central and peripheral nervous system.
The importance of therapeutic intervention is vital; however, it is not free of complications. This could explain the bimodal presentation of mortality reported by Urowitz [17].
The use of corticosteroids, immunosuppressants such as cyclophosphamide, and, recently, monoclonal antibodies decreases the risk of progression of the disease by controlling inflammation but increases the risk of infection.
In the case of metabolic diseases, especially DM type II could be secondary at use of glucocorticoids and lifestyle patterns no modified that increase the risk of death secondary to immunosuppression and vascular diseases associated. The use of concomitant drugs to control glucose levels and blood pressure continuously contributes to a good control of the disease and a better outcome.
Survival of patients with ARD in the last 5 decades has improved significantly due to the use of medications such as glucocorticoids, immunosuppressants, monoclonal antibodies, and concomitant drugs (antihypertensive agents, antibiotics, etc.).
However, for the extended use of glucocorticoids, there has also been an increase in the risk of developing infections. Saag et al. reported an 8 times increased risk (OR) compared to those who do not use them [9].
Petri et al. reported a higher risk of infection when comparing patients with SLE with and without hospitalization, with doses of prednisone higher than 10 mg/day [7], and Listing et al. in RA found that doses of glucocorticoids above 5 mg were associated with an increase in mortality [10].
In general terms, an increased risk of death has not been demonstrated with the use of immunosuppressants; two authors, Bultink and Listing, reported a lower risk of mortality (not statistically significant) in patients with SLE intake any immunosuppressant drugs [10, 11], and Mok et al. highlight that the use of immunosuppressants was not associated with increased survival in patients with SLE; however, the risk of infections increases considerably [12].
In recent years, the number of studies on the causes of mortality in ARDs has increased, although the methodologies used are diverse; the results of most studies show infections as the main cause, followed by cardiovascular and pulmonary diseases.
Some studies have also described disease activity as the cause of death, and it stands out that at least two of them report the cause of death as missing or unknown.
Recently, in a population study in Greece, Bournia et al. have described that mortality in rheumatic diseases occurs more frequently compared to the general population, preferably in young patients and the prevalence is higher in the main inflammatory diseases (SLE, SV and SSC) [24].
It is possible that factors such as the quality of care provided by health services and the socioeconomic conditions of the patients are not correctly recorded, and for now, it is not possible to establish a direct relationship with these factors that are mentioned anecdotally as contributors to the mortality of the ARDs.
The consensus is that effective therapeutic modalities such as treat-to-target and effective control of comorbidities improve survival and, with experience obtained with this methodology in RA and EA during the years 2015–2019, should be extended to all ARDs [24].
Table 1 summarizes the most important studies in recent years and identifies the main causes. Most agree in reporting that infections, CV and pulmonary complications, and disease activity are the leading causes of death.
It also allows you to view the comorbidities that are reported as a product of the same disease, associated with the disease or consequence of the therapeutic used, such as HBP, endocrine and metabolic diseases, kidney failure, liver complications, and cancer.
We found that the variation between the main reported causes is little; the results of most studies show infections as the main cause, followed by cardiovascular and pulmonary diseases.
The risk is largely different among various ARDs, due to diverse underlying pathogenetic mechanisms and the degree of vital organ involvement, as well as due to different therapeutic regimes used and different age of onset of each disease.
The higher mortality (five times more) that has been reported in Latin America compared to in Europe is significantly important. It could be related to the quality and inequity in the provision of health services; this analysis is beyond this review.
The most important factor in the last decades is the habitual use of drugs that increase the risk of immunosuppression and infection. It is common that the ARDs are characterized by increased morbidity and mortality, due to disease-specific factors and iatrogenic damage (e.g., drug-related side effects) and the associated comorbidity as cardiovascular disease, malignancy, and increased risk for infections.
The routine electronic or manual recording systems for death, admissions, and hospital discharge statistics provide only a partial picture of the prevalence of ARDs and could be the reason why these diseases have a low lethality and hospitalization frequency.
This research did not receive any specific funding from public sector, commercial sector, or not-for-profit agencies.
References
1.Thomas SL, Griffiths C, Smeeth L, Rooney C, Hall AJ. Burden of mortality associated with autoimmune diseases among females in the United Kingdom. American Journal of Public Health. 2010;100:2279-2287. Available from: https://ajph.aphapublications.org/doi/abs/10.2105/AJPH.2009.180273
2.Toledano E, Candelas G, Rosales Z, Martínez C, León L, Abásolo L, et al. A meta-analysis of mortality in rheumatic diseases. Reumatología Clínica. 2012;8:334-341. DOI: 10.1016/j.reuma.2012.05.006
3.Tselios K, Gladman D, Sheane B, Su J, Urowitz M. All-cause, cause-specific and age-specific standardized mortality ratios of patients with systemic lupus erythematosus in Ontario, Canada over 43 years (1971-2013). Annals of the Rheumatic Diseases. 2019;78:802-806. DOI: 10.1136/annrheumdis-2018-214802
4.Martinez M, Quinteros C, Abud C. Hospitalizations and mortality in Mexican patients with systemic lupus erythematosus (SLE) or rheumatoid arthritis (RA). Annals of the Rheumatic Diseases. 2014;73(Suppl. 2):115. DOI: 10.1136/annrheumdis-2014-eular.4784
5.Mok C, Kwok L, Ho L, Chan P, Yip S. Life expectancy, standardized mortality ratios, and causes of death in six rheumatic diseases in Hong Kong, China. Arthritis and Rheumatism. 2011;63:1182-1189. DOI: 10.1002/art.30277
6.Panoulas V, Metsios G, Pace A, John H, Treharne G, Banks M, et al. Hypertension in rheumatoid arthritis. Rheumatology (Oxford, England). 2008;47:1286-1298. DOI: 10.1093/rheumatology/ken159
7.Petri M, Mease P, Merrill J, Lahita R, Iannini M, Yocum D, et al. Effects of prasterone on disease activity and symptoms in women with active systemic lupus erythematosus. Arthritis and Rheumatism. 2004;50:2858-2868. DOI: 10.1002/art.20427
8.Sabio J, Vargas-Hitos J, Navarrete-Navarrete N, Mediavilla J, Jiménez-Jáimez J, Díaz-Chamorro A, et al. Prevalence of and factors associated with hypertension in young and old women with systemic lupus erythematosus. The Journal of Rheumatology. 2011;38:1026-1032. DOI: 10.3899/jrheum.101132
9.Saag KG, Koehneke R, Caldwell JR, Brasington R, Burmeister LF, Zimmerman B, et al. Low dose long-term corticosteroid therapy in rheumatoid arthritis: An analysis of serious adverse events. The American Journal of Medicine. 1994;96:115-123. DOI: 10.1016/0002-9343(94)90131-7
10.Listing J, Kekow J, Mangere B. Mortality in rheumatoid arthritis: The impact of disease activity, treatment with glucocorticoids, TNF inhibitors and rituximab. Annals of the Rheumatic Diseases. 2015;74:415-421. DOI: 10.1136/annrheumdis-2013-204021
11.Bultink I, de Vries F, van Vollenhoven R, Lalmohamed A. Mortality, causes of death and influence of medication use in patients with systemic lupus erythematosus vs matched controls. Rheumatology. 2020;00:1-10. DOI: 10.1093/rheumatology/keaa267
12.Mok C, Tse S, Chan K. Effect of immunosuppressive therapies on survival of systemic lupus erythematosus: A propensity score analysis of a longitudinal cohort. Lupus. 2017;27:722-727. DOI: 10.1177/0961203317739129
13.Lederer M. Form of acute hemolytic anemia-probably of infectious origin. American Journal of Medical Sciences. 1925;170:500-510
14.Callahan L, Pincus T. Mortality in the rheumatic diseases. Arthritis Care and Research. 1995;8:229-241. DOI: 10.1002/art.1790080406
15.Cobb S, Anderson F, Bauer W. Length of life and cause of death in rheumatoid arthritis. The New England Journal of Medicine. 1953;249:553-556. DOI: 10.1056/nejm195310012491402
16.Mitchell DM, Spitz PW, Young DY, Bloch DA, Mc-Shane DJ, Fries JF. Survival, prognosis, and causes of death in rheumatoid arthritis. Arthritis and Rheumatism. 1986;29:706-714. DOI: 10.1002/art.1780290602
17.Urowitz M, Bookman A, Koehler GD, Smythe H, Ogryzlo M. The bimodal mortality pattern of systemic lupus erythematosus. The American Journal of Medicine. 1976;60:221-225. DOI: 10.1016/0002-343(76)90431-9
18.Wolfe F, Hassett AL, Walitt B, Michaud K. Mortality in fibromyalgia: A study of 8,186 patients over thirty-five years. Arthritis Care & Research (Hoboken). 2011;63:94-101. DOI: 10.1002/acr.20460
19.Scherlinger M, Mertz P, Sagez F, Meyer A, Felten R, et al. Worldwide trends in all-cause mortality of auto-immune systemic diseases between 2001 and 2014. Autoimmunity Reviews. 2020;19:102531. DOI: 10.1016/j.autrev.2020.102531
20.Plotz PH. Autoimmunity: The history of an idea. Arthritis and Rheumatism. 2014;66:2915-2920. DOI: 10.1002/art.38796
21.Pollard K, Hultman P, Kono D. Immunology and genetics of induced systemic autoimmunity. Autoimmunity Reviews. 2005;4:282-288. DOI: 10.1016/j.autrev.2004.12.005
22.Leonardo H, Carrascosa M, Arreola R, Herrera-Méndez M. Causes of mortality associated with autoimmune rheumatic disease in a referral hospital. Reumatología Clínica. 2022;18:304-308. DOI: 10.1016/j.reuma.2021.02.010
23.Mitratza M, Klijs B, Hak E, Kardaun J, Kunst A. Systemic autoimmune disease as a cause of death: Mortality burden and comorbidities. Rheumatology. 2021;60:1321-1330. DOI: 10.1093/rheumatology/keaa537
24.Bournia V, Fragoulis G, Mitrou P, Mathioudakis K, Tsolakidis A, Konstantonis G, et al. All-cause mortality in systemic rheumatic diseases under treatment compared with the general population, 2015-2019. RMD Open. 2021;7:e001694. DOI: 10.1136/rmdopen-2021-001694
25.Garen T, Lerang K, Hoffmann-Vold A, Andersson H, Midtvedt Q , Brunbor C, et al. Mortality and causes of death across the systemic connective tissue diseases and the primary systemic vasculitides. Rheumatology. 2019;58:313-320. DOI: 10.1093/rheumatology/key285
26.Dadoniene J, Charukevic G, Jasionyte G, Staškuviene K, Miltiniene D. Mortality in inflammatory rheumatic diseases: Lithuanian National Registry Data and systematic review. International Journal of Environmental Research and Public Health. 2021;18:12338. DOI: 10.3390/ijerph182312338
Written By
Maynor Herrera-Méndez
Submitted: 23 May 2023Reviewed: 18 June 2023Published: 15 December 2023
 Open access peer-reviewed chapter
Open access peer-reviewed chapter