Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
To purchase hard copies of this book, please contact the representative in India:
CBS Publishers & Distributors Pvt. Ltd.
www.cbspd.com
|
customercare@cbspd.com
An organization of cells and molecules with specific functions for protection against infection is known as the immune system. When immune system reacts against its own cells known as an autoimmune disease. Autoimmune thyroid diseases are grouped under endocrinal diseases in which the immune system attacks the body’s own thyroid gland. In autoimmune thyroid disease (AITD), an immunological alteration occurs in the follicular cells of the thyroid gland. In this case, certain enzymes, surface proteins, and receptors such as thyroperoxidase, thyroglobulin, and thyroid-stimulating hormone (TSH) receptors start acting as antigens; against these antigens, relevant antibodies are produced by the body, and cell-mediated cytotoxicity gets induced. These autoimmune endocrinal diseases are characterized by the presence of high titers of antibodies like thyroperoxidase antibodies (TPO-Abs) and thyroglobulin antibodies, produced by our own body system. In conclusion, anti-TPO can play a crucial role in the diagnosis of autoimmune thyroiditis. Anti-TPO is the prognosis marker for the child and adult who have normal thyroid function tests in euthyroidism, subclinical thyroidism. Thus, anti-TPO along with thyroid function tests play a substantial role in the clinical management of autoimmune thyroiditis.
National Academy of Medical Sciences, Bir Hospital, Kathmandu, Nepal
*Address all correspondence to: nurakantn@gmail.com
1. Introduction
Immune system is made up of complex organ systems, cells, and proteins to fight against pathogens (microbes). This immune system helps to keep the body healthy by protecting fight against pathogens. Defects in the immune system or malfunctioning in the immune response can provoke illness or disease. When the immune systems reacts against self-cells is known as autoimmune disease. These autoimmune diseases are either organ-specific or systemic disease. Autoimmune thyroiditis is organ-specific autoimmune disease.
Autoimmune thyroid diseases are grouped under endocrinal diseases in which the immune system attacks the body’s own thyroid gland. These autoimmune endocrinal diseases are characterized by the presence of high titers of antibodies, such as TPO-Abs (thyroperoxidase antibodies) and thyroglobulin antibodies, produced by our own body system.
Due to the organ-specific autoimmune disorders, autoimmune thyroid disease is much more common in women than men [1]. Men are affected by 1%, whereas women are by 2–4%, which rate surges with age worldwide [2].
Hereditary factors, that is, gene alteration are one of the main causes in manifestation of AITD, and other factors such as advancing age, smoking, iodine overconsumption, adverse effects of medication, and hormonal changes (in females) known as environmental and endogenous are also responsible for the initiation of AIDT [3, 4].
In AITD, immunological alteration occurs in the follicular cells of the thyroid gland. In this case, certain enzymes, surface proteins, and receptors such as thyroperoxidase, thyroglobulin, and TSH receptors start acting as antigen; against these antigens, relevant antibodies are produced by the body, and cell-mediated cytotoxicity gets induced. This leads to autoimmune thyroid disease. These antibodies damage the thyrocytes and cause inflammation of the thyroid gland [4, 5].
The common antibodies measured in serum samples are thyroglobulin and thyroperoxidase antibodies [5]. TPO antibody has frequently been found in the general population as compared to other antibodies. Along with TSH, free T3 and free T4, anti-TPO antibodies are more specific in the diagnosis of AITD. The levels of free T3, free T4, and TSH help in distinguishing the two conditions: hypothyroidism and hyperthyroidism. Hypothyroidism is a condition in which the level of thyroid hormones (free T3, free T4 decreases), and in hyperthyroidism, the level of thyroid hormones increases from its normal range. The titer of anti-TPO antibodies above its normal value indicates an autoimmune response to the thyroid gland. So, anti-TPO antibody testing is helpful in differentiating between autoimmune thyroid disease and other thyroid disorders.
Thyroid diseases are classified as euthyroidism, subclinical thyroidism, and clinical or overt thyroidism on the basis of thyroid hormone levels. Anti-TPO antibody, TSH, free T3, and free T4 remain normal in euthyroidism. In subclinical thyroidism, anti-TPO antibodies and TSH are increased and patients remain asymptomatic with mild impairment in the thyroid gland. It is more common than overt thyroidism, and it can prevent the progression of overt thyroidism and have effects on early diagnosis and treatment of subclinical thyroidism [6]. Anti-TPO Abs and TSH are remarkably increased in overt thyroidism, whereas other thyroid hormones’ levels depend upon hyperthyroidism or hypothyroidism. Clinical thyroiditis is a symptomatic disease and depression, unexplained weight loss, etc. are the main complications. Hashimoto and graves’ thyroid diseases are common examples. In this chapter, we will discuss a brief introduction of immune system and its type and a detail discussion of autoimmune thyroiditis, the role of anti-TPO in autoimmune thyroiditis, and the clinical application of anti-TPO in diagnosis and management of autoimmune disease.
The following databases were thoroughly search: Web of Science, Scopus, PubMed/MEDLINE, Google scholar, Sematic Scholar, Embase. The terms autoimmune thyroiditis, Hashimoto thyroiditis, Graves’ disease, and anti-TPO were used in a search for articles that had no specific publication date.
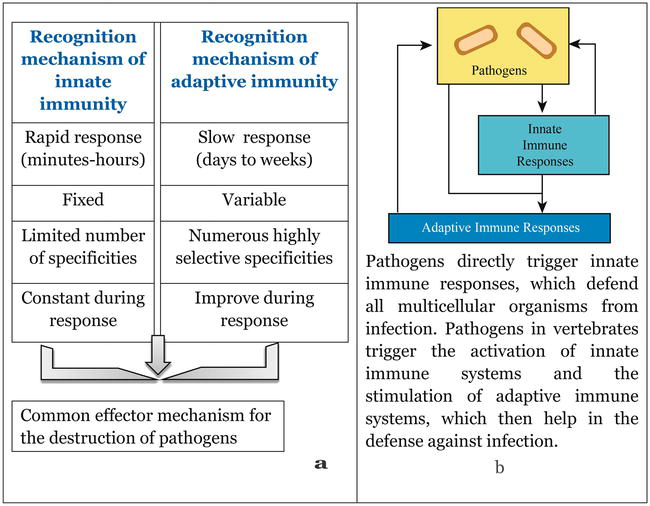
An organization of cells and molecules with a specific function for protection against infection is known as immune system. Basically, there are two types of immune responses, that is, innate immunity and adaptive immunity to intruding microbes (organisms such as bacteria, fungi, and parasites), viruses, cancer cells, and toxins. Innate (natural) immune system is the first line of defense for invading pathogens also known as the non-specific immune system, whereas the adaptive (acquired) immune system is the second line of defense response to repeated exposure to microbial antigens during the innate immune. Phagocytic cells (neutrophils, monocytes, and macrophages) use innate responses that release (basophils, mast cells, and eosinophils), and natural killer cells as inflammatory mediators. Complement, acute-phage proteins, and cytokines-interferons- are the molecular component of innate immunity. Proliferations of antigen-specific B and T cells are mainly involved in the acquired immune system and this occurs when an antigen binds to the surface receptors of these cells. In the response of the antigen, antigen-presenting cells display to lymphocytes and collaborate with them. The production of antibodies by B cells is helped by T cells, which may also kill virally infected cells and destroy intracellular infections by activating macrophages. Pathogens are typically eliminated together by the responses of innate and acquired. Figure 1 shows the principal characteristics of innate and adaptive immunity and innate and adaptive immune responses [7, 8].
Figure 1.
(a) The principal characteristics of innate and adaptive immunity. (b). Innate and adaptive immune responses [7, 8].
3.1 Innate immunity
Within minutes or hours of coming into contact with an antigen, the host activates innate immunity, a non-specific (antigen-independent) defensive mechanism. Since the innate immune system lacks immunologic memory, it is unable to identify or “memorize” the same pathogen should the body come into contact with it again in the future. Four different forms of protective barriers are included in innate immunity: anatomic (skin and mucous membrane), physiological (temperature, low pH, and chemical mediators), endocytic and phagocytes, and inflammatory. The barrier of non-specific host-defense mechanisms is summarized in Table 1. Innate immunity to infections is dependent on pattern recognition receptors (PRRs), which enable a specific subset of immune cells to quickly identify and react to a variety of pathogens that have similar molecular patterns (PAMPs). These include bacterial cell walls such as lipopolysaccharides (LPS) and double-stranded ribonucleic acid (RNA) generated during viral infection.
Barrier
Mechanism
Anatomic
Skin
Mechanical barrier retards entry of microbes
Acidic environment (pH 3–5) retards growth of microbes
Mucous membrane
Normal flora compete with microbes for attachment sites
Mucous entraps foreign microbes
Cilia propel microbes out of body
Physiologic
Temperature
Body temperature/fever response inhibits growth of some pathogens
Low pH
Acidic pH of stomach kills most undigested microbes
Chemical mediators
Lysozyme cleaves bacterial cell wall
Interferon induces antiviral defenses in uninfected cells
Complement lyses microbes or facilitates phagocytosis
Phagocytic/endocytic barriers
Various cells internalize (endocytosis) and break down foreign macromolecules
Tissue damage and infection induce leakage of vascular fluid containing serum protein with antibacterial activity, leading to influx of phagocytic cells into the affected area
Table 1.
Summary of non-specific host-defense mechanism for barriers of innate immunity.
3.2 Adaptive immunity
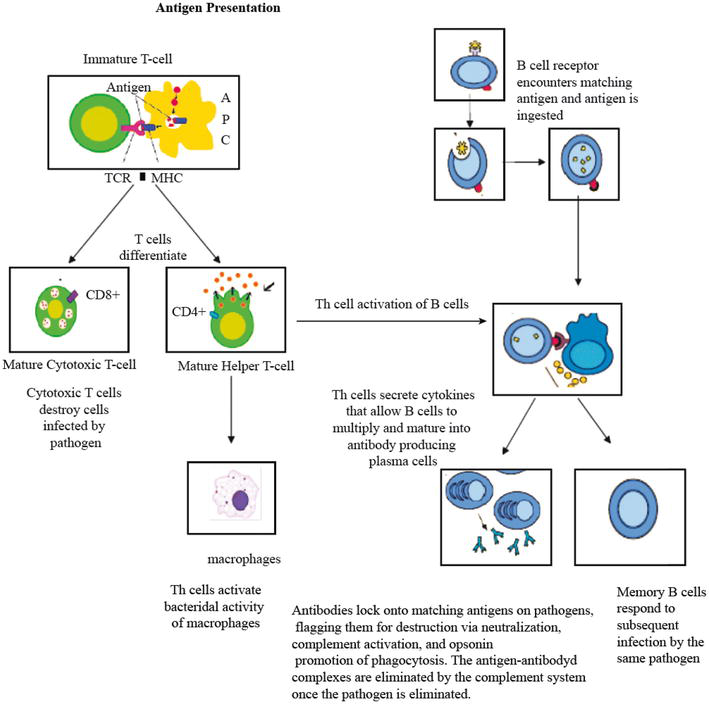
The adaptive immune responses are very specific to the individual pathogen that triggered them, in contrast to innate immune responses. Additionally, they can provide enduring defense. The adaptive immune system, for instance, provides lifelong immunity against measles for those who have recovered from the disease, but not to other common viruses like those that cause mumps or chickenpox. Recognition of particular “non-self” antigens and their distinction from “self” antigens; development of pathogen-specific immunologic effector pathways that destroy particular pathogens or pathogen-infected cells; and the formation of an immunologic memory that can quickly eradicate a specific pathogen should consequent infections occur are the three main functions of an adaptive immune response [9]. Adaptive immune responses are the basis for effective immunization against infectious diseases. The cells of the adaptive immune system include antigen-specific T cells, which are activated to proliferate through the action of APCs, and B cells which differentiate into plasma cells to produce antibodies. Effective immunization against infectious illnesses is based on adaptive immune responses. The cells of the adaptive immune system are antigen-specific T cells and B cells. T cells are activated to proliferate through the action of APCs, and B cells differentiate into plasma cells to produce antibodies. Activation and function of B cells and T cells are summarized in Figure 2 [10]. Apart from this, B cells play a major role in the humoral or antibody-mediated immune response and T cells play the cell-mediated immune response [9, 11].
Figure 2.
Adaptive immunity: T-cell and B-cell activation and function [10].
3.3 Antibody-mediated and cell-mediated immunity
3.3.1 Antibody-mediated immunity
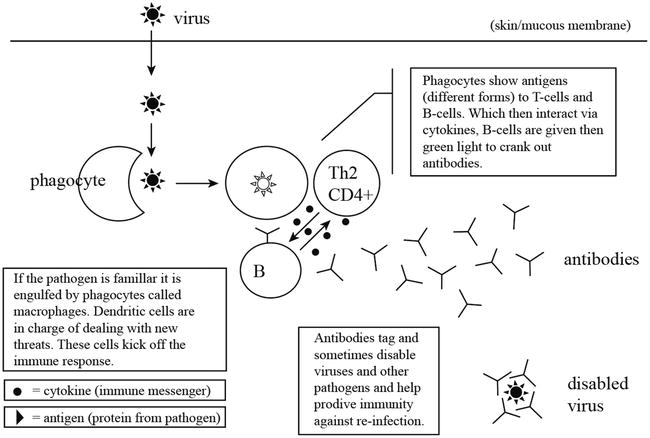
The immunity mediated by B-cell-antibody production in the extracellular body fluids in the responses of pathogen is known as antibody-mediated or humoral immunity. When the B cell’s antigen-binding receptor recognizes and attaches to antigen in its native form, the antibody production pathway begins. Local Th cells release cytokines that support B cell proliferation and direct the type of antibody generated. Certain cytokines, such as IL-6, aid in the maturation of B-cells into antibody-secreting plasma cells. Secreted antibodies attach to antigens on pathogen surfaces, signaling them for destruction via complement activation, opsonin-mediated phagocytosis, and pathogen elimination by immune effector cells. The complement cascade clears antigen-antibody complexes after the pathogen is eliminated. Therefore, antibody-mediated immunity plays an important role against pathogens that grow on extracellular spaces. The basic model of antibody-mediated immunity against pathogens (virus) is shown in Figure 3 [12].
Figure 3.
Basic model of antibody-mediated (Th2) immunity against pathogen [12].
B cells produce five major types of antibodies: IgA, IgD, IgE, IgG, and IgM. IgG antibodies can be further split into structurally diverse subclasses with a range of complement fixing, opsonin, and other functional properties. The major classes of antibodies recognize and neutralize specific pathogens that have substantially different biological functions [10].
During the acute stage of infection, antibodies are crucial in controlling viral growth. However, once a virus has been infected, they are typically unable to remove it.
3.3.2 Cell-mediated immunity
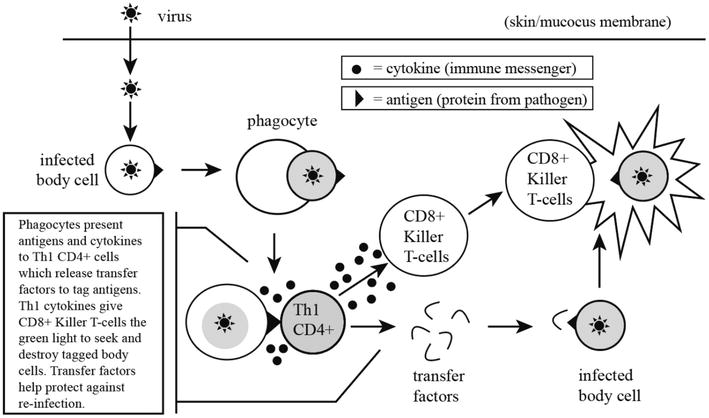
When an infection is established, cell-mediated immune mechanisms are significant in host defense against most intracellular pathogens. Cell-mediated immunity is other kind of adaptive immunity that generates mature T cells, macrophages, and cytokines against pathogens are proliferated. In addition, two types of lymphocytes are engaged in cell-mediated immunity: helper T cells and cytotoxic T cells. The cell-mediated immunity proceeds in three phases including T-cell activation by presenting antigens with MHC complexes, T-cell binding and activation, and differentiation of activated T cells into effector cells and memory T cells, which is illustrated in Figure 4 [12].
Figure 4.
Basic model of cellular-mediated (Th1) immunity with pathogen (virus) [12].
Furthermore, T cells are generated in the bone marrow and mature in the thymus. T cells are found in the blood and lymphoid tissue after entering the bloodstream. Antigen-presenting cells (APCs) present antigens to T lymphocytes together with major histocompatibility complexes (MHC). T cells proliferate and develop into armed effector cells when they come into contact with an antigen. Cytotoxic T cells kill infected cells by triggering apoptosis. T helper cells encourage the production of antibodies by plasma B cells.
In addition, IgG and IgM antibodies are the two main types of antibodies produced by T helper cells in response to plasma B cells. Memory T cells are developed T cells, but their action is dependent on antigen activation. Cellular immunity is most effective against virus-infected cells and cancer cells, but it can also help to guard against fungus, protozoa, malignancies, and intracellular bacteria. This type of immunity also plays a significant role in transplant rejection.
3.4 Active and passive immunity
3.4.1 Active immunity
When the immune system produces antibodies to a disease after being exposed to the disease organism is known as active immunity. Either natural immunity or vaccine-induced immunity can be used to build up active immunity.
Exposure to the disease agent and subsequent infection with the disease itself are the two ways that natural immunity is acquired.
Vaccine-induced immunity is acquired through the administration of a vaccine that can consist of attenuated (weakened) pathogens, inactivated organisms or specific proteins, or carbohydrates known to induce immunity.
In any case, if an immune individual later comes into contact with that disease, their immune system will instantly recognize it and produce the antibodies required to fight it. Active immunity lasts for a very long time—sometimes a lifetime.
3.5 Passive immunity
When an antibody against a disease is given to a person rather than the individual making them naturally through their immune system is called passive immunity.
Through the placenta, a newborn baby gains passive immunity from its mother.
By receiving immune globulin or other blood products containing antibodies, such as those used to treat specific diseases, people can potentially develop passive immunity.
The main benefit of passive immunity is that it provides protection immediately, in contrast to active immunity, which takes time (often several weeks) to develop. However, passive immunity only lasts a few weeks or months. Long-lasting can only be active immunity.
3.6 Immunopathology
Defects or malfunctions in either the innate or adaptive immune response can provoke illness or disease. Such disorders are generally caused by an overactive immune response (known as hypersensitivity reactions), ineffective immune responses (known as immunodeficiency), or an inappropriate reaction to self (known as autoimmunity).
3.6.1 Hypersensitivity reactions
An undesirable responses produced by the normal immune system are referred to as hypersensitivity reactions. There are four types of hypersensitivity reactions [13, 14].
Type I: immediate hypersensitivity
Type II: cytotoxic or antibody-dependent hypersensitivity
Type III: immune complex disease
Type IV: delayed-type hypersensitivity
3.6.2 Immunodeficiency
When the ability to fight against infectious disease is compromised or totally absent is known as immunodeficiency. Immunodeficiency can be caused by a mainly genetic defect (primary immunodeficiency), which can affect innate or acquired immune function by inhibiting specific immune cells or pathways, or they can develop as a result of a secondary cause (secondary immunodeficiency), such as bacterial or viral infections, malnutrition, autoimmunity, or medication that causes immunosuppression. Leukemia and multiple myeloma are immunodeficiency disorders that directly or indirectly impair the immune system. Immunodeficiency is also the hallmark of acquired immunodeficiency syndrome (AIDS), caused by the human immunodeficiency virus (IV). HIV directly infects Th cells and also weakens other immune system responses [15, 16].
3.6.3 Autoimmunity
Autoimmune disease is characterized by the activity of auto-reactive lymphocytes, which cause loss of normal immune homeostasis that react against host tissues, or effector T cells, which are specific for endogenous self-peptides [17]. The presence of self-reactive T cells, auto-antibodies, and inflammation are the main characteristics of autoimmunity. Autoimmune diseases can be classified as either systemic or organ-specific. In systemic disease, the immune system attacks self-antigen in several organs. For instance, in systemic lupus, erythematous inflammation occurs in several organs, such as the skin, joints, and kidneys, among other organs. In an organ-specific disease, the immune response is directed toward antigens in a single organ. For example, autoantibodies attack the adrenal cortex in Addison’s disease. Some common examples of autoimmune diseases are Celiac disease, type 1 diabetes mellitus, Addison’s disease, and autoimmune thyroiditis [18]. In autoimmune thyroiditis immune system attacks on the thyroid gland cause disorders in thyroid hormones consequences effects on the metabolic system, body temperature, and proteins synthesis, etc.
The thyroid gland is an endocrine gland located in the neck region, in front of the larynx and trachea. Leonardo Da Vinci was the first scientist to draw the thyroid gland as an anatomical organ [19]. Andreas Vesalius, an anatomist, published the first anatomic description and image of the gland in 1543. Thyroid Wharton, in 1656, used the term “thyroid” for the first time [20]. Thyroid is a Greek word to indicate the shape of a shield. In 1656, the thyroid gland was mentioned in Western medicine for the first time; before this, it was considered to have lubrication of trachea as its main function [21]. The thyroid gland contains numerous follicles, composed of epithelial follicle cells and colloids [22]. The main function of the thyroid gland is to make major hormones like T3 and T4 required for the maintenance and regulation of metabolic processes throughout the body. An endocrinal disease of thyroid gland leads to under or overproduction of these hormones due to adverse activity of the gland. AIDT is one of the major endocrinal diseases in which antibodies are produced against the own thyroid cells, i.e., thyrocytes, and inflammation of the thyroid gland occurs [23].
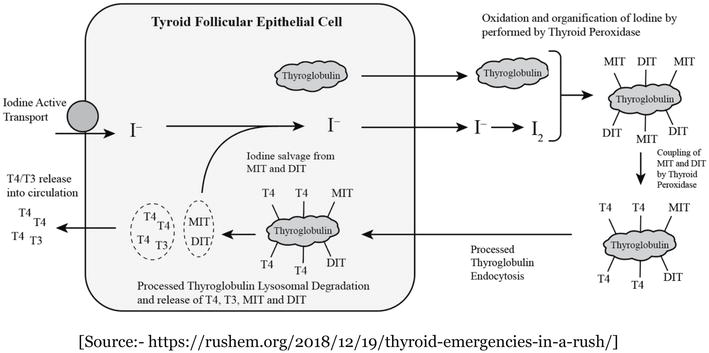
As shown in Figure 5, the thyroid gland produces mainly two hormones, T3 (tri-iodotyrosine) and T4 (tetra-iodotyrosine) [24]. The synthesis of these two hormones takes place in the follicular cells of the thyroid gland. The process is regulated by the hypothalamus, the master gland, and by feedback inhibition mechanism [25]. The mechanisms of biosynthesis of thyroid hormones are illustrated below:
Uptake of iodide by follicular cells.
Iodine organification by thyroperoxidase.
Combining of iodine and thyroglobulin.
MIT (Mono-Iodotyrosine) /DIT (Di-Iodotyrosine) store in follicular space.
Reabsorbing of MIT/DIT.
T3, T4 formation from MIT/DIT.
T3, T4 release into serum.
With the release of iodine T3, T4 break down.
Figure 5.
Synthesis of thyroid hormones [24].
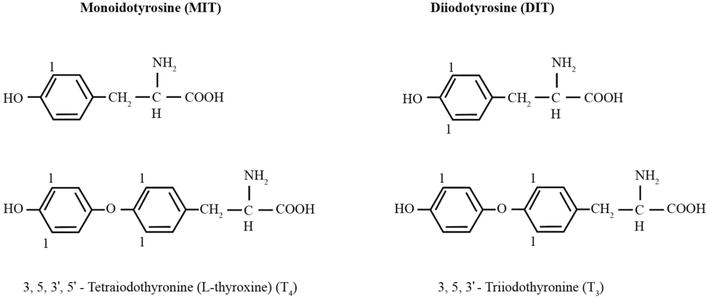
Biochemical structure of T3 and T4 is shown below in Figure 6 [26].
AITD is a complex and multifactorial disease in which the immune system attacks the thyroid gland by producing antibodies against thyroid antigens developed against a particular genetic background initiated by exposure to environmental factors. It is the most common endocrinal disease that occurs due to the formation of autoantibodies against thyroid-specific peroxidase and other receptor proteins, such as the thyrotropin receptor, present on thyrocytes [27]. These endocrinal diseases are characterized by the presence of antibodies such as TPO-Abs (thyroperoxidase antibodies) and thyroglobulin, produced by our own body system.
Silva et al. conducted a study of 89 Brazilian women, and they found that 90% of people with autoimmune thyroiditis have elevated anti-TPO [28]. Anti-TPO antibody was used more extensively by Lock et al. for clinical evaluation in subclinical hypothyroidism [29]. TPO antibody-positive people were found to be 13.3% in a study conducted in Delhi between 2007 and 2010 [30]. Similarly, an apparent increase in occurrence was observed in southern India. In two separate studies conducted in Kerala and Punjab, the comparable prevalence of anti-TPO positives was 16.7 and 36.5%, respectively [31, 32]. Jeena et al. reported that anti-TPO antibody estimates are useful in identifying the etiology of autoimmune thyroiditis. In that study, anti-TPO antibody titers were found to be elevated in 47 to 60% of patients with hypothyroidism [33].
Hashimoto characterized hypothyroidism and goiter as a result of thyroid lymphoid invasion in 1912. Anti-Tg (antithyroglobulin) antibodies were discovered in similar patients in 1956, revealing the autoimmune origin of these traits, and activating TSH receptor antibodies were discovered at the same period of time. Anti-TPO antibodies were first identified as thyroid microsomal antibodies in 1964 but were later renamed anti-TPO because of their auto-antigen identity [34].
AITD is considered the prototypical and most prevalent organ-specific endocrinal disease, affecting 2–5% of the iodine-sufficient population [35]. The first pathological features of AITD were described in 1912, when patients with goiter caused diffusion of lymphocyte infiltration and thyroid cellular atrophy in the clinical histological picture of thyroid tissue [36]. The incidence rate is 0.3–1.5 per 1000 persons per year, and it is 4–10 times higher in women than in men [2, 37, 38].
AITD is an organ-specific autoimmune disorder that is much more common in women than in men. About 1% of men are affected by this disease, whereas 2–4% women are suffering from it worldwide and with the advanced age, this trend is greater. In the USA and Canada, the prevalence rates are 5,873,102 and 6, 50,157, respectively. In China and India, the prevalence rates are 25, 976, 952 and 21,301,112, respectively. The annual incidence of Hashimoto’s thyroiditis is believed to be 0.3–1.5 cases per 1000 people worldwide, while Grave’s disease is expected to have five occurrences per 10,000 people. About 90% of AITDs are caused by Hashimoto’s thyroiditis [39].
As AITD is a multifactorial disease, the factors responsible for the initiation of AITD are mostly genetic, in which gene alteration occurs. Hormonal changes in females, medication adverse effects, smoking, aging, and iodine overconsumption are other endogenous and environmental factors that cause autoimmune thyroid disease [3, 4]. Environmental factors such as smoking, alcohol, iodine, stress, infections, and drugs are secondary etiological factors responsible for AITD. Female sex and parity are considered existential factors responsible for AITD because of certain sex hormonal imbalances, women are considered to be more prone to AITD as compared to men. Increased age has also been shown to be conclusively linked to AITD [40, 41, 42, 43, 44]. Certain gene alterations, such as TSH receptor, thyroglobulin, HLA, interleukins, and cytotoxic lymphocyte genes, are primary etiological factors responsible for causing AITD.
More than 30% of all organ-specific autoimmunity diseases are represented by thyroid autoimmune. About 3% of the population is affected by Hashimoto’s thyroiditis, the earliest and most prevalent organ-specific autoimmune disease. It serves as the prototypical T-cell-mediated degenerative disease among others such as multiple sclerosis and type 1 diabetes [45, 46, 47]. However, the theory of cytotoxic T lymphocyte (CTL)-mediated target destruction in thyroid autoimmunity has lately been challenged [48, 49, 50, 51]. A new theory of autoimmune target destruction in Hashimoto’s thyroiditis has been developed as a result of advancements in the study of apoptosis and investigations of Graves’ disease, a non-destructive type of thyroid autoimmunity.
It is thought that the thyroid antigen-specific CD4 (helper) T lymphocytes are what triggers the autoimmune thyroid disease process. T cells with this antigen-specificity have been isolated from the thyroid tissue of Grave’s disease patients [47, 52]. Through the induction of activated T cells and subsequent production of gamma interferon, thyroid cells express MHC class II, which activates T-cell reticulation and sustains the autoimmune process [53, 54].
Since the thyroid itself encourages further expansion of the pertinent population of T cells; the mechanism underlying the initial activation of T cells may be less antigen-specific than in molecular mimicry. Self-reactive CD4 T cells promote auto-reactive B cells to enter the thyroid and secrete thyroid antibodies. Thyroglobulin, the storage protein for thyroid hormones, thyroperoxidase, and TSH receptors are the three main target antigens for thyroid autoantibodies. In autoimmune thyroiditis, Th1, Th2, and Th17 immune responses involve active participation. Antigen-presenting cells and CD4+ T helper cells play a role in the activation of effector T cells, and as a result, thyroid-specific antigens (TPO and Tg) CD8+ T cells are activated, which proliferate cytotoxic T lymphocytes (CTL) that destroy thyroid cells, and on the other hand, B cells might develop into plasma cells, generating thyroid-restricted antibodies, followed by antibody- or complement-restricted thyroid cell death. It is believed that Th17 cells are also involved in the destruction process. Increase the release of thyroid-specific antigens by the destroyed thyrocytes, which leads to an acceleration of the immune process. Inhibition of regulatory T cells (Treg) as well as secretion of inflammatory molecules (CXCL8, CXCL10, and interferon-g) by the thyroid itself could further enhance the autoimmune process [55, 56] CD8 (cytotoxic) T cells and B cells are drawn into the thyroid by activated CD4 T cells [57, 58]. It is thought that the primary mechanism causing hypothyroidism involves CD8 cells directly killing thyroid cells. Thyroid autoantibodies, however, might also play a pathogenic role [59].
11. Types of autoimmune thyroid diseases
There are the following types of autoimmune thyroid disease:
Hashimoto’s autoimmune thyroiditis (AITD), is atrophic and causes primary myxedema.
Grave’s disease hyperthyroidism.
Postpartum thyroiditis (PPT).
Thyroid-associated orbitopathy (TAO).
In Graves’ disease, thyroid-stimulating antibodies were found in 1956, and in 1957, thyroid antibodies were found in Hashimoto’s disease [60, 61]. Hypertrophic thyroiditis is the most prevalent autoimmune thyroid disease in Hashimoto’s disease. The immune system responds against the body’s own tissue and it show features such as diffuse goiter, lymphocytic infiltration in the presence of autoantibody, and the gradual degeneration of the follicular cells of thyroid gland resulting in a deficiency of thyroid hormones, which help in the diagnosis of Hashimoto’s thyroiditis [55, 57, 62]. Autoimmune thyroid disease results in two opposite pathogenic effects: hyperthyroidism in Grave’s disease and thyroid destruction in Hashimoto’s thyroiditis.
Hashimoto’s thyroiditis is caused by self-reactive CD4+ T cells attracting B cells and CD8+ T cells to the thyroid. Thyroid cell death and hypothyroidism are symptoms of disease progression. It has been suggested that autoimmune thyrocyte depletion is caused by both autoantibodies and thyroid-specific cytotoxic T lymphocytes (CTLs). In Grave’s disease, B cells release thyroid-stimulating immunoglobulins (TSI) against the thyroid-stimulating hormone receptor (TSHR), which is triggered by activated CD4+ T cells. This results in hyperthyroidism and unregulated thyroid hormone production [63].
Grave’s disease is characterized by elevated levels of thyroid-specific autoantibodies and circulating activated T cells. These anti-TSH receptor antibodies promote thyroid activity and cause hyperactivity of the gland [61]. While free T3 and free T4 hormone concentrations are within the normal range, subclinical Hashimoto’s thyroiditis is identified by a decreased serum TSH level (less than 0.3 mIU/ml). TSH and thyroid hormone levels are both decreased in clinically present (0ver) hypothyroidism [64]. In Grave’s disease, hyperthyroidism occurs, which leads to enlargement of the thyroid gland. In the case of Grave’s disease, anti-TPO antibodies do not play a major role but majorly cause Hashimoto’s thyroidism.
It is common to have subclinical hypothyroidism. The prevalence ranges from 3 to 8%, rising with age and affecting more women than men. Around 10% of men and women experience combined prevalence after the sixth decade. Anti-thyroid antibodies are present in 80% of these patients, and 80% of them have serum TSH levels that are less than 10 mIU/L [65]. Although a patient with subclinical hypothyroidism does not exhibit the appropriate signs and symptoms, there is a slight increase in TSH and anti-TPO levels, which are still within normal ranges for free T3 and free T4 levels.
About 2 to 5 percent of cases per year will progress from subclinical hypothyroidism to overt hypothyroidism. Early diagnosis and treatment help prevent the onset of overt hypothyroidism and its negative effects on the body’s system because subclinical hypothyroidism is more common than overt hypothyroidism [66]. High anti-TPO patient titers increase the risk of overt condition changes and increase symptom severity.
According to the National Health and Nutrition Examination Survey III (NHANES), over 10 percent of adults tested positive for either TPO-Ab or Tg-Ab, with a prevalence of 13% for TPO-Ab and 11.5% for Tg-Ab [67]. In a study conducted by Atieh Amouzegar et al., out of 5783 participants, 742 (12.8%) tested positive for TPO-Ab, with women more likely than men to do so. In the general population, TPO-Ab positivity was present in 11.9, 14.9, and 13.6% of the young, middle-aged, and elderly, respectively [68].
12. TPO introduction and role in body
TPO, previously known as thyroid microsomal antigen, was defined in 1985, responsible for the autoimmune response in AITD [69]. It is an enzyme that is present in microsomes of thyrocytes and expressed on the apical surface of thyroid cells. Thyroperoxidase is also called thyroid-specific peroxidases, as it is only present in thyrocytes and not in any other organ of the body. The secreted recombinant human TPO comprises 842 amino acids and has a predicted molecular mass of 93.8 kDa [70].
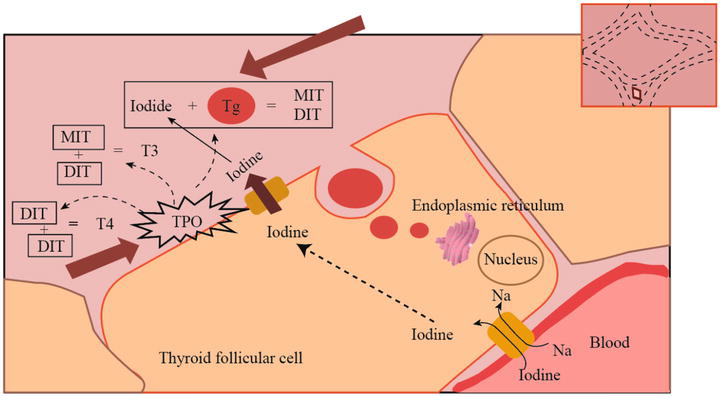
TPO plays a key enzyme role in the biosynthesis of thyroid hormone. This process takes place in thyrocytes at the apical membrane colloid interface and requires thyroglobulin, iodine, and hydrogen peroxide. Iodide is actively transported into the follicular cells through the sodium iodide support system. In follicular cells, the process of deiodination occurs when iodine is used to create the active ionic form of iodide. TPO oxidizes iodide by using hydrogen peroxide created in the cell’s peroxisomes, which cause covalent bonds to form with the thyroglobulin residue, that is, tyrosyl. MIT (monoiodotyrosine) and DIT (di- iodotyrosine) are produced as a result. Two DIT combine to form T4 (thyroxine) and one MIT and one DIT combine to form T3 (tri-Iodothyronine), which is illustrated in Figure 7 [71]. The coupling reaction is also catalyzed by TPO in the presence of hydrogen peroxidase [72]. So, in addition to working in concert with thyroglobulin, the TPO enzyme is crucial for the iodination of L-tyrosine and the chemical coupling of mono- and di-iodotyrosine to produce thyroid hormones [5, 73].
Figure 7.
Function of Thyroperoxidase in thyrocytes, coupling of MIT and DIT, synthesis of T3 and T4 [71].
13. Role of TPO antibodies in AITD (autoimmune thyroid disease)
In cases of autoimmune thyroid disorders, the body’s autoantibodies start to produce antibodies against the thyroperoxidase enzyme, called as anti-thyroperoxidase antibodies [74]. These antibodies mistakenly attack normal tissue, such as thyrocytes in the thyroid gland. Due to the attack of anti-TPO antibodies, there is inflammation and impaired function of the thyroid gland [75]. Several studies report that antibody-dependent cell-mediated cytotoxicity could be induced by thyroperoxidase antibodies. TPO-Ab is frequently found in the general population and has more specificity than other antibodies; this antibody directly involves thyroid cellular damage and is positively correlated with the activity of chronic thyroiditis [76]. Autoantibodies to TPO are more common in the euthyroid population. Elevated serum titers of antibodies to TPO are found in several forms of thyroiditis caused by autoimmune disorders [77]. Inflammation or destruction of the thyroid gland, like in Hashimoto’s disease, may be indicated by the presence of TPO antibodies. Whereas other forms of thyroiditis, such as postpartum thyroid dysfunction (PPTD), are less commonly associated with TPO antibodies [78].
Anti-TPO antibodies are more sensitive in diagnosing thyroid autoimmune diseases. Some patients have mildly elevated levels of anti-TPO antibodies but do not show sign or symptoms. The presence of TPO antibodies increases the risk of future thyroid disorders. In such patients, the doctor recommends periodic checkups to monitor the prognosis of thyroid ailments.
In the HUNT study, positive TPO-Ab was found in 2.8% of men and 13.9% of women, aged over 40 years [79]. Similarly positive TPO-Ab status was found in 8.6% of men and 18.5% of women in the study of Hoogendoorn et al. [80]. Furthermore, TPO-Ab titers >200 kU/l were reported in 16.9% of women and 6.6% of men in a study conducted in Denmark [81].
14. Signs and symptoms of AITD
Signs and symptoms of autoimmune thyroid disease depend on thyroid gland function, whether the patient is suffering from hyperthyroidism or hypothyroidism. In the case of hyperthyroidism, the symptoms will be sweating, rapid heart rate, tremors, weight loss, fatigue, anxiety, sleeping difficulty, etc. In the case of hypothyroidism, symptoms will include weight gain, dry skin, hair loss, cold intolerance, constipation, fatigue, etc. The signs and symptoms will vary as per the severity of the disease, which is illustrated in Table 2. This could be permanent if AITD is at a chronic stage. Symptoms may come and go depending on whether the person receives treatment, and whether the treatment takes effect.
Common sign and symptoms in hyperthyroidism and hypothyroidism.
15. Laboratory diagnosis of AITD
For laboratory diagnosis, the doctor recommends thyroid function testing along with thyroid antibody testing. In a thyroid function test, the following parameters are checked:
TSH (Thyroid-stimulating hormone) testing.
Free T3 (Tri-iodotyrosine)
Free T4 (Tetra-iodotyrosine)
Anti TPO Ab testing.
Free T3 and free T4 are both biologically active forms, and they are free in circulation, so their value remains constant and is not affected by the concentration of circulatory proteins. So, free T3 and free T4 are preferred over total T3 and T4.
In thyroid antibody testing, TG antibodies and TPO antibodies are determined, as these are commonly found autoantibodies that are frequently present in serum. Anti-TPO is more sensitive and has more specificity for the diagnosis of thyroid autoimmune disease and hence is preferred.
16. Normal reference values
The following Table 3 shows the reference range of thyroid parameters:
Parameter
Normal range
Anti-TPO (Thyroperoxidase) U/ml
5.0–35.0
TSH (uIU/ml)
0.27–4.20
Free T3 (pg/ml)
2.0–4.4
Free T4(ng/dl)
0.93–1.73
Table 3.
Normal reference ranges of thyroid function test for ATD diagnosis.
17. Interpretations
Subclinical hypothyroidism occurs when patients have no signs or symptoms as such, mildly elevated values of anti-TPO antibodies and TSH, but normal levels of other thyroid hormones such as free T3 and free T4. If subclinical thyroid is left untreated for a long time, it can switch over to an overt hypothyroidism condition, and the patient becomes symptomatic. In overt hypothyroidism, the levels of anti-TPO antibody titer and TSH are markedly elevated, along with mildly variably elevated levels of other thyroid hormones, such as free T3 and free T4.
18. Role of TPO-Ab in disease pathogenesis
TPO-Ab is uncommon in healthy children and adolescent is low, but the prevalence increases with age and especially predominant in females [32, 82]. Anti-TPOs are detected mostly in patients with autoimmune hypothyroidism. The presence of TPO-Ab contributes to the confirmation of the autoimmune nature of thyroid failure. In patients with “borderline” thyroid function test, TPO-Ab status can be used for treatment decisions. Furthermore, even in people with normal TSH and thyroid hormone levels, the presence of TPO-Ab, particularly in younger age groups, can predict the development of future thyroid dysfunction. Evidence suggests that antibody status can determine the clinical course of autoimmune hypothyroidism.
19. Conclusion
This organ-specific endocrinal disease is becoming a major and challenging disease worldwide. Autoimmune thyroid diseases occur due to immune-mediated alterations in the thyroid gland, which produce functional alterations in thyroid hormone status. Proper diagnosis helps with better treatment of this disease.
Thyroid hormone synthesis significantly relies on the TPO enzyme. In order to diagnose autoimmune thyroid disease and forecast its clinical course, measuring the levels of anti-TPO autoantibodies has been reported to be important. In order to identify the cause of hypothyroidism and the likelihood that a patient’s subclinical condition will progress to overt hypothyroidism, serum TSH and anti-TPO analyses are crucial. TSH, free T3, and free T4 levels also aid in the diagnosis of autoimmune thyroid disease and help distinguish between overt and subclinical hypothyroidism.
Acknowledgments
I would like to thank Jasjot Singh for his help in writing, and I would also like to thank Asso. Prof. Pitambar Lamichane and Resham Shrestha for their help in drawing. I am eternally grateful to all of you for this.
Conflict of interest
The author declares no conflict of interest.
Abbreviations
AIDS
acquired immunodeficiency syndrome
AITD
autoimmune thyroid disease
Anti-Tg
anti-thyroglobulin
APCs
antigen presenting cells
ATP
amino triphosphate
CLT
cytotoxic T lymphocyte
DIT
di-iodotyrosine
HIV
human immunodeficiency virus
HLA
human leucocyte antigen
LPS
lipopolysaccharides
MHC
major histocompatibility complex
MIT
mono-iodotyrosine
NHANES
National health and nutrition examination survey III
PAMPs
pathogens that have similar molecular patterns
PPT
postpartum thyroiditis
PPTD
postpartum thyroid dysfunction
PRR
pattern recognition receptors
RNA
ribonucleic acid
TAO
thyroid-associated orbitopathy
TCR T
cell receptor
Tg
thyroglobulin
TPO
thyroperoxidase
TPO-Abs
thyroperoxidase antibodies
TSH
thyroid stimulating hormone
T3
tri-iodotyrosine
T4
tetra-iodotyrosine
References
1.Swain M, Swain T, Mohanty BK. Autoimmune thyroid disorders-an update. Indian Journal of Clinical Biochemistry. 2005;20(1):9-17
2.Canaris GJ, Manowitz NR, Mayor G, Ridgway EC. The colorado thyroid disease prevalence study. Archives of Internal Medicine. 2000;160(4):526-534
3.Holt PG. Immune and inflammatory function in cigarette smokers. Thorax. 1987;42(4):241-249
4.Nelson JLSA. In: Berczi IKK, editor. Sex Steroids, Autoimmunity and Autoimmune Disease. London, Lancaster: MTP Press; 1987. pp. 93-119
5.Gey A, Diallo A, Seneschal J, Léauté-Labrèze C, Boralevi F, Jouary T, et al. Autoimmune thyroid disease in vitiligo: Multivariate analysis indicates intricate pathomechanisms. The British Journal of Dermatology. 2013;168(4):756-761
6.Turnbridge WMG, Evered DC, Hall R, Appleton D, Brewis M, Clark F, et al. The spectrum of thyroid disease in a community: The whickham survey.Clinical Endocrinology. 1977;7:481-493. DOI: 10.1111/j.1365-2265.1977.tb01340.x
7.Parham P, Janeway C. The Immune System. 5th ed. New York: Garland Science, Taylor & Francis; 2021
8.Alberts B, Heald R, Johnson A, Morgan DO, Raff MC, Roberts K, et al. Molecular Biology of the Cell. 7th ed. New York: W. W. Norton & Company; 2022
9.Bonilla FA, Oettgen HC. Adaptive immunity. The Journal of Allergy and Clinical Immunology. 2010;125(2 Suppl. 2):S33-S40
10.Marshall JS, Warrington R, Watson W, Kim HL. An introduction to immunology and immunopathology. Allergy, Asthma & Clinical Immunology. 2018;14(2):49
11.Murphy K, Weaver C. Janeway’s Immunobiology. 9th ed. New York: Garland science; 2016
12.White AM. A Guide to Transfer Factors and Immune System Health. 2nd ed. North Chasleston, SC: BookSurge; 2009
14.Rajan TV. The Gell-Coombs classification of hypersensitivity reactions: A re-interpretation. Trends in Immunology. 2003;24(7):376-379
15.Notarangelo LD. Primary immunodeficiencies. The Journal of Allergy and Clinical Immunology. 2010;125(2 Suppl. 2):S182-S194
16.Chinen J, Shearer WT. Secondary immunodeficiencies, including HIV infection. The Journal of Allergy and Clinical Immunology. 2010;125(2 Suppl. 2):S195-S203
17.Sinha AA, Lopez MT, McDevitt HO. Autoimmune diseases: The failure of self tolerance. Science. 1990;248(4961):1380-1388
18.Castro C, Gourley M. Diagnostic testing and interpretation of tests for autoimmunity. The Journal of Allergy and Clinical Immunology. 2010;125(2 Suppl. 2):S238-S247
19.Gley E. Sur les fonctions du corps thyroid. Comptes rendus des séances de la societe de biologie et de ses Filiales. 1891;43:841-842
20.Graves RJ. Newly observed affection of the thyroid gland in females. Medical-Surgical Nursing Journal. 1835;7:516
21.Jr HR. Thyroid and antithyroid drugs. In: Gilman AG, Rall TW, Nies AS, et al., editors. The Pharmacological Basis of Therapeutics. 8th ed. New York: Pergamon Press; 1990. pp. 1361-1383
22.Vanderpump MPJ, Tunbridge WMG. Epidemiology and prevention of clinical and subclinical hypothyroidism. Thyroid. 2002;12(10):839-847
23.Wiersinga WM. Subclinical hypothyroidism and hyperthyroidism. I. Prevalence and clinical relevance. The Netherlands Journal of Medicine. 1995;46(4):197-204
25.Tortora GJ, Derrickson BH. Principles of Anatomy and Physiology [Internet]. 12th ed. Philadelphia: John Wiley & Sons; 2008. Available from: https://books.google.com.np/books?id=uNwfOPPYgKAC
26.Satyanarayana U, Chakrapani U. Biochemistry. 6th ed. New Delhi: Elsevier; 2021
27.McIntosh RS, Asghar MS, Weetman AP. The antibody response in human autoimmune thyroid disease. Clinical Science. 1997;92:529-541
28.Silva LM, Chavez J, Canalli MHB, Zanetti CR. Determination of IgG subclasses and avidity of antithyroid peroxidase antibodies in patients with subclinical hypothyroidism - a comparison with patients with overt hypothyroidism. Hormone Research. 2003;59(3):118-124
29.Lock RJ, Marden NA, Kemp HJ, Thomas PH, Goldie DJ, Gompels MM. Subclinical hypothyroidism: A comparison of strategies to achieve adherence to treatment guidelines. Annals of Clinical Biochemistry. 2004;41(Pt 3):197-200
30.Unnikrishnan AG, Kalra S, Sahay RK, Bantwal G, John M, Tewari N. Prevalence of hypothyroidism in adults: An epidemiological study in eight cities of India. Indian Journal of Endocrinology and Metabolism. 2013;17(4):647-652
31.Marwaha RK, Tandon N, Ganie MA, Kanwar R, Sastry A, Garg MK, et al. Status of thyroid function in Indian adults: Two decades after universal salt iodization. The Journal of the Association of Physicians of India. 2012;60:32-36
32.Singh J, Prabhakar PK, Neupane N. Hospital-based clinical study on prevalence of TPO antibodies in association to autoimmune thyroid diseases in tertiary care hospital. Asian Journal of Pharmaceutical and Clinical Research [Internet]. 2020;13:186-189; Available from: https://api.semanticscholar.org/CorpusID:234539770
33.Jeena E, Malathi M, Sudeep K. A hospital-based study of anti-TPO titer in patients with thyroid disease. Muller Journal of Medical Sciences and Research [Internet]. 2013;4(2):74-77. Available from: https://www.mjmsr.net/article.asp?issn=0975-9727
34.Saravanan P, Dayan CM. Thyroid autoantibodies. Endocrinology and Metabolism Clinics of North America. 2001;30(2):315-337, viii
35.Sgarbi JA, Maciel RMB. Pathogenesis of autoimmune thyroid diseases. Arquivos Brasileiros de Endocrinologia e Metabologia. 2009;53(1):5-14
36.Hashimoto H. Zur Kenntniss der lymphomatosen Veranderung der Schilddruse (struma lymphomatosa). Arch Klin Chir. 1912;97(219):219-248
37.Huber A, Menconi F, Corathers S, Jacobson EM, Tomer Y. Joint genetic susceptibility to type 1 diabetes and autoimmune thyroiditis: From epidemiology to mechanisms. Endocrine Reviews. 2008;29(6):697-725
38.Iddah MA, Macharia BN, Ng'wena AG, Keter A, AVO O. Thryroid hormones and hematological indices levels in thyroid disorders patients at moi teaching and referral hospital, Western Kenya. ISRN Endocrinology. 2013;2013:385940
39.Vanderpump MP, Tunbridge WM, French JM, Appleton D, Bates D, Clark F, et al. The incidence of thyroid disorders in the community: A twenty-year follow-up of the Whickham survey. Clinical Endocrinology. 1995;43(1):55-68
40.Ghoraishian SM, Hekmati Moghaddam SH, Afkhami-Ardekani M. Relationship between anti-thyroid peroxidase antibody and thyroid function test. Iranian Journal of Immunology. 2006;3(3):146-149
41.Nagataki S, Yamashita S, Tamai H. Immunogenetics of autoimmune endocrine disease. In: Volpe R, editor. Autoimmune Diseases of Endocrine System. Boca Raton: CRC Press; 1990. pp. 51-72
42.Schleusener H, Bogner U, Peters H, Kotulla P, Schmieg D, Grüters A, et al. The relevance of genetic susceptibility in Graves’ disease and immune thyroiditis. Experimental and Clinical Endocrinology. 1991;97(2-3):127-132
43.Plotnikoff NP, Murgo AJ, Faith RE. Stress and Immunity [Internet]. Boca Raton: Taylor & Francis; 1991
44.Glaser R, Kiecolt-Glaser JK. Handbook of Human Stress and Immunity. St Louis, Missouri, USA: Elsevier Science; 2014
45.Wucherpfennig KW, Eisenbarth GS. Type 1 diabetes. Nature Immunology. 2001;2:767-768
46.Steinman L. Multiple sclerosis: A two-stage disease. Nature Immunology. 2001;2:762-764
47.Weetman AP, McGregor AM. Autoimmune thyroid disease: Further developments in our understanding. Endocrine Reviews. 1994;15(6):788-830
48.Giordano C, Stassi G, De Maria R, Todaro M, Richiusa P, Papoff G, et al. Potential involvement of Fas and its ligand in the pathogenesis of Hashimoto’s thyroiditis. Science. 1997;275(5302):960-963
49.De Maria R, Testi R. Fas-FasL interactions: A common pathogenetic mechanism in organ-specific autoimmunity. Immunology Today. 1998;19(3):121-125
50.Stassi G, Todaro M, Bucchieri F, Stoppacciaro A, Farina F, Zummo G, et al. Fas/Fas ligand-driven T cell apoptosis as a consequence of ineffective thyroid immunoprivilege in Hashimoto’s thyroiditis. Journal of Immunology. 1999;162(1):263-267
51.Stassi G, Di Liberto D, Todaro M, Zeuner A, Ricci-Vitiani L, Stoppacciaro A, et al. Control of target cell survival in thyroid autoimmunity by T helper cytokines via regulation of apoptotic proteins. Nature Immunology. 2000;1(6):483-488
52.Bottazzo GF, Pujol-Borrell R, Hanafusa T, Feldmann M. Role of aberrant HLA-DR expression and antigen presentation in induction of endocrine autoimmunity. Lancet (London, England). 1983;2(8359):1115-1119
53.Londei M, Bottazzo GF, Feldmann M. Human T-cell clones from autoimmune thyroid glands: Specific recognition of autologous thyroid cells. Science. 1985;228(4695):85-89
54.Dayan CM, Londei M, Corcoran AE, Grubeck-Loebenstein B, James RF, Rapoport B, et al. Autoantigen recognition by thyroid-infiltrating T cells in Graves disease. Proceedings of the National Academy of Sciences of the United States of America. 1991;88(16):7415-7419
55.Mooij P, de Wit HJ, Bloot AM, Wilders-Truschnig MM, Drexhage HA. Iodine deficiency induces thyroid autoimmune reactivity in Wistar rats. Endocrinology. 1993;133(3):1197-1204
56.Ehlers M, Schott M. Hashimoto’s thyroiditis and papillary thyroid cancer: Are they immunologically linked? Trends in Endocrinology and Metabolism. 2014;25(12):656-664. DOI: 10.1016/j.tem.2014.09.001. Epub 2014 Oct 9
57.Dayan CM, Daniels GH. Chronic autoimmune thyroiditis. The New England Journal of Medicine. 1996;335(2):99-107
58.Schott M, Scherbaum WA. Autoimmune thyroid disease. Dtsch Arztebl. 2006;103(45):A3023-A3032
59.Eguchi K. Apoptosis in autoimmune diseases. Internal Medicine. 2001;40(4):275-284
60.Adams DD. Abnormal response in the assay of thyrotropin. Proceedings of the University of Otago Medical School. 1956;34:11-12
61.Doniach D, Roitt IM. Auto-immunity in Hashimoto’s disease and its implications. The Journal of Clinical Endocrinology and Metabolism. 1957;17(11):1293-1304
62.Neupane N, Kaur M, Prabhakar PK. Treatment of Hashimoto’s thyroiditis with herbal medication. International Journal of Green Pharmacy. 2017;11(3):S343- S347
63.Stassi G, De Maria R. Autoimmune thyroid disease: New models of cell death in autoimmunity. Nature Reviews. Immunology. 2002;2:195-204. DOI: 10.1038/nri750
64.Hueston WJ. Treatment of hypothyroidism. American Family Physician. 2001;64(10):1717-1724
65.Fatourechi V. Subclinical hypothyroidism: An update for primary care physicians. Mayo Clinic Proceedings. 2009;84(1):65-71
66.Cooper DS. Subclinical hypothyroidism. JAMA. 1987;258:246-247
67.Pedersen IB, Knudsen N, Jørgensen T, Perrild H, Ovesen L, Laurberg P. Thyroid peroxidase and thyroglobulin autoantibodies in a large survey of populations with mild and moderate iodine deficiency. Clinical Endocrinology. 2003;58(1):36-42
68.Amouzegar A, Gharibzadeh S, Kazemian E, Mehran L, Tohidi M, Azizi F. The prevalence, incidence and natural course of positive antithyroperoxidase antibodies in a population-based study: Tehran thyroid study. PLoS One. 2017;12(1):e0169283
69.Czarnocka B, Ruf J, Ferrand M, Carayon P, Lissitzky S. Purification of the human thyroid peroxidase and its identification as the microsomal antigen involved in autoimmune thyroid diseases. FEBS Letters. 1985;190(1):147-152
70.Ruf J, Carayon P. Structural and functional aspects of thyroid peroxidase. Archives of Biochemistry and Biophysics. 2006;445(2):269-277
71.Balucan FS, Morshed SA, Davies TF. Thyroid autoantibodies in pregnancy: Their role, regulation and clinical relevance. Journal of Thyroid Research. 2013;2013:182472, 15 pages. DOI: 10.1155/2013/182472
72.Song Y, Driessens N, Costa M, De Deken X, Detours V, Corvilain B, et al. Roles of hydrogen peroxide in thyroid physiology and disease. The Journal of Clinical Endocrinology and Metabolism. 2007;92(10):3764-3773
73.Il SJ, Kim MJ, Lee JS. Graves’ disease, rheumatoid arthritis, and anti-tumor necrosis factor-alpha therapy. The Journal of Rheumatology. 2009;36:449-450; author reply 450
74.Volpe R. Autoimmune Diseases of the Endocrine System. Boca Raton: CRC Press, Taylor & Francis; 1990. ISBN: 9780849368493
75.Beever K, Bradbury J, Phillips D, McLachlan SM, Pegg C, Goral A, et al. Highly sensitive assays of autoantibodies to thyroglobulin and to thyroid peroxidase. Clinical Chemistry. 1989;35(9):1949-1954
76.Li Y, Teng D, Shan Z, Teng X, Guan H, Yu X, et al. Antithyroperoxidase and antithyroglobulin antibodies in a five-year follow-up survey of populations with different iodine intakes. The Journal of Clinical Endocrinology and Metabolism. 2008;93(5):1751-1757
77.Pfannenstiel P, Hotze LSBS. Schilddrüsenkrankheiten Diagnose und Therapie. 2nd ed. Berlin: Berliner Medizinische Verlagsanstalt; 1995. pp. 28-30, 141, 169 – 172, 200 – 201 p
78.Swelam EESA, Bakr HG, Mansour MAE-A. Postpartum thyroid dysfunction: A state of immunological dysregulation. Clinical Laboratory. 2011;57(9-10):731-739
79.Bjoro T, Holmen J, Krüger O, Midthjell K, Hunstad K, Schreiner T, et al. Prevalence of thyroid disease, thyroid dysfunction and thyroid peroxidase antibodies in a large, unselected population. The health study of Nord-Trondelag (HUNT). European Journal of Endocrinology. 2000;143(5):639-647
80.Hoogendoorn EH, Hermus AR, de Vegt F, Ross HA, Verbeek ALM, Kiemeney LALM, et al. Thyroid function and prevalence of anti-thyroperoxidase antibodies in a population with borderline sufficient iodine intake: Influences of age and sex. Clinical Chemistry. 2006;52(1):104-111
81.Knudsen N, Jorgensen T, Rasmussen S, Christiansen E, Perrild H. The prevalence of thyroid dysfunction in a population with borderline iodine deficiency. Clinical Endocrinology. 1999;51(3):361-367
82.Roti E, Gardini E, Minelli R, Bianconi L, Braverman LE. Prevalence of anti-thyroid peroxidase antibodies in serum in the elderly: Comparison with other tests for anti-thyroid antibodies. Clinical Chemistry. 1992;38(1):88-92
Written By
Nurakant Neupane
Submitted: 17 July 2023Reviewed: 06 September 2023Published: 15 January 2024
 Open access peer-reviewed chapter
Open access peer-reviewed chapter