Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
To purchase hard copies of this book, please contact the representative in India:
CBS Publishers & Distributors Pvt. Ltd.
www.cbspd.com
|
customercare@cbspd.com
This chapter delves into the multifaceted etiology of Buerger’s disease, also known as thromboangiitis obliterans (TAO), exploring a spectrum of factors contributing to its onset and the initiation of vascular inflammation. We comprehensively summarize our research findings regarding TAO’s pathogenesis, employing key indicators in our immune study, including cellular immunity, humoral immunization, and immunopathology. Our research unequivocally confirms TAO as an autoimmune disease characterized by multiple hypersensitivity reactions, primarily type III hypersensitivity, accompanied by type II, type IV, and type I reactions. Furthermore, our investigation uncovers a hypercoagulation state in the blood of TAO patients, shedding light on the intricate interplay between vascular immune dysregulation and thrombosis. These insights establish a robust foundation for implication diagnosis and treatment of this complex condition.
Department of Surgery, Ruijin Hospital Affiliated to Shanghai Jiao Tong University, School of Medicine, Shanghai, China
WanChao Wang
Shanghai Institute of Immunology, School of Medicine, Shanghai Jiao Tong University, Shanghai, China
*Address all correspondence to: portiazheng@gmail.com
1. Introduction
Buerger’s disease (thromboangiitis obliterans, TAO) was first meticulously described by Dr. Leo Buerger in 1908 and 1924. TAO is widely distributed worldwide but exhibits a remarkable variation in incidence worldwide [1]. In North America, it accounts for 0.75%, and in Western Europe, the prevalence ranges from 0.5% to 5.6% of peripheral vascular disease. While in Eastern Europe, the Middle East, the Mediterranean region, and Asia, it accounts for up to 60–80% of peripheral vascular diseases several years ago [1].
TAO is an inflammatory disease affecting the walls of small and medium-sized arteries and veins, accompanied by intraluminal thrombosis, mainly affecting the limbs. The excruciating pain it inflicts has, regrettably, driven some patients toward drug abuse and even limb amputation. In past decades, high-level amputations have soared to an alarming 20% [1]. The severity of the condition underscores its profound implications for public health. Nevertheless, the absence of specific diagnostic markers and the shortage of precise and effective treatment methodologies can be attributed to a limited comprehension of the disease’s etiology and pathogenesis. In response, our comprehensive and in-depth investigation into the disease’s pathogenesis aims to bridge these gaps in knowledge. We anticipate that our findings will serve as a critical cornerstone in advancing the field.
Given the uneven global distribution of the disease and its infrequent occurrence in certain regions, there remains a pressing need to acquaint medical professionals with its clinical manifestations and diagnosis.
The affected extremity may have abnormal sensations like tingling, numbness, or a sensation of burning. The skin color of the affected area can appear pale or purple.
2.2 Coolness
The skin of the affected extremity feels cool to the touch.
2.3 Hair loss or slow hair growth
There may be a loss of hair or reduced hair growth on the affected limb.
2.4 Dry skin and decreased sweating
The skin in the affected area may become dry, and exhibit decreased or no sweating.
2.5 Muscle relaxation, atrophy, and reduced circumference
The muscles in the affected limb may become relaxed, leading to muscle atrophy and a reduced circumference of the limb.
2.6 Migratory superficial phlebitis
More than 50% of cases recur early in TAO or throughout the course of the disease. Painful flushing nodular plaques or cords, mostly located in the superficial veins of the dorsum of the feet and calves, a few cases can extend to the thighs, one or several superficial veins are involved, and the length is several millimeters, several centimeters to several 10 centimeters, the duration of the attack is generally 1–3 weeks, after which the redness, swelling, and pain gradually subside, leaving traces of pigmentation. Some cases have recurrent outbreaks, one after another, more or less, protracted for several years.
2.7 Intermittent claudication
This is a common symptom of TAO. It refers to pain that occurs during physical activity, typically walking. The pain is usually felt in the calf muscles and is often described as a knife-like or colicky sensation. Walking aggravates the pain, and it is relieved by rest. The location of the pain can provide information about the specific arteries that are affected.
2.8 Pain at rest
As TAO progresses, the pain can occur even at rest. It is often more severe when lying down or during sleep. It indicates a severe blockage in the blood vessels, which is a warning of impending ulceration or gangrene in the extremities.
2.9 Ulcers and gangrene
In severe cases of TAO, complete ischemia (lack of blood flow) can lead to the development of ulcers and gangrene in the limb (Figure 1). Dry gangrene refers to tissue death without the presence of exudate or pus, while wet gangrene involves tissue infection, edema, and the production of exudate or pus. The pain during this stage is very severe.
Figure 1.
TAO foot gangrene.
2.10 The weakened or disappeared arterial pulses
Mostly in the small and medium arteries. The dorsalis pedis or posterior tibial arteries are the first to be affected by the weakened or disappeared arterial pulses, followed by popliteal and femoral. Iliac arteries and abdominal aorta were very rare. In the upper extremity, the pulsation of the ulnar and radial arteries weakened and disappeared most, followed by the brachial artery, and those involving the axillary artery were very rare.
2.11 Buerger’s test positive
The patient lays on his back, raises the lower limbs by 45 degrees for 3 minutes, and performs repeated stretching and flexing of the feet. It can be seen that the skin of the soles of the feet turns pale. Subsequently, the patient experiences increased numbness, coolness, and pain. Guide the patient to sit up and let the lower limbs hung down, resulting in a delayed return of normal skin color to the feet, taking 45–50 seconds (normally within 10 seconds). Additionally, the skin appears excessively flushed.
2.12 Clinical manifestations of visceral thromboangiitis obliterans
Visceral TAO is not uncommon [2]. Many scholars have confirmed from autopsy and pathology that the heart (coronary artery), brain (middle cerebral artery and its branches, etc.), and abdominal organs (mesenteric artery, gastroepiploic artery, renal artery, etc.) have the presence of TAO. Clinically, it is seen that some patients with thromboangiitis obliterans with physical symptoms have symptoms of insufficient blood supply to internal organs after several years of onset, such as patients with cerebral artery disease may have migraine, paroxysmal headache, transient hemianopia or amaurosis, transient hemiplegia, sensory impairment, speech impairment, disorientation, memory loss, etc. can also occur.
Patients with coronary artery disease may experience angina pectoris, myocardial infarction, and arrhythmia. Although some cases were confirmed as regressive myocardial infarction by electrocardiogram, the patients were asymptomatic. In some cases, chest tightness and even typical symptoms and signs of myocardial infarction appeared. We have also reported three cases of these kind of patients.
Patients with vascular lesions of the digestive tract may experience paroxysmal abdominal pain, vomiting, diarrhea, and even intestinal necrosis, perforation, and bleeding.
Patients with renal artery disease may experience edema and high blood pressure; urinalysis will show proteinuria, hematuria, and casts.
In short, the symptoms of visceral TAO vary according to the location of the lesion and the degree of obstruction.
3. Clinical diagnostic criteria for TAO of extremities
3.1 The clinical diagnostic criteria for TAO of extremities are as follows
3.1.1 Male predominance
The incidence is mainly in males, with few females. Females should be particularly cautious when diagnosing TAO.
3.1.2 Age of onset
The age of onset is typically between 20 and 40 years old.
3.1.3 Smoking history
The vast majority of patients have a history of smoking.
3.1.4 Superficial phlebitis
Migratory superficial phlebitis in the limbs with a history of recurrent attacks.
3.1.5 Weakening or disappearance of limb artery pulsation
The pulsation of the small arteries in the limbs weakens or disappears, often starting in one lower limb, accompanied by a series of ischemic symptoms such as cold extremities, intermittent claudication, and rest pain.
3.1.6 Exclusion of other vascular diseases
Other vascular diseases caused by different reasons, especially extremity arteriosclerotic occlusion (ASO) and diabetic foot (DF), should be excluded.
3.2 The key points for the diagnosis of visceral thromboangiitis obliterans
3.2.1 Thromboangiitis obliterans
The patient has a history of thromboangiitis obliterans affecting the limbs.
3.2.2 Gradual onset of persistent symptoms
The pathological features usually involve transient ischemic attacks at the onset, which gradually become persistent symptoms.
3.2.3 Rule out other causes of visceral vascular ischemia
Other causes of visceral vascular ischemia should be ruled out.
3.2.4 Arteriography resembling limb TAO arteriography
Visceral arteriography exhibits characteristics similar to limb TAO arteriography.
The etiology of Buerger’s disease can be attributed to several factors. Here is a summary of the potential causes identified:
4.1 Age
The onset of Buerger’s disease commonly occurs between the ages of 20 and 40, with a majority of cases (84%) falling within this range in our 876 case statistic. It is rare for individuals under the age of 20 to develop the disease. One case of the minimum age is 17 years old in our 876 cases [3].
4.2 Gender
In our analyzed cases, the majority of patients were men, accounting for 99% [3]. However, it is noted that some reports indicate a higher prevalence of the disease in women, potentially linked to an increase in female smokers [1].
4.3 Cold and damp exposure
A significant number of patients had a history of exposure to cold temperatures and humidity before the onset of Buerger’s disease. Factors such as sudden exposure to cold after heat during strenuous exercise, as well as exposure to fire after cold, were mentioned. According to our clinical data analysis of this disease, about 80% of the patients had a history of the above condition in 876 cases [3]. It seems that the factors of sudden exposure to cold (heat) and sudden exposure to heat (cold) are very important, which may easily cause vasomotor dysfunction or damage the blood vessels.
4.4 Trauma
While the role of trauma in the development of Buerger’s disease requires further clarification, approximately 29% of the patients in the analyzed 876 cases had a history of trauma. Other reports from China suggest a range of 10–35% for trauma-related cases.
4.5 Diet and nutrition
Diet and nutrition: certain dietary factors have been associated with the occurrence of Buerger’s disease. Studies have shown a relationship between chronic tobacco poisoning, lack of vitamin B1, and vitamin C deficiency in rats, which can induce vasculitis. Analysis of cases in Indonesia indicated that many patients lacked protein in their diet, particularly essential amino acids. Therefore, nutritional deficiencies may have a connection to the disease’s occurrence [4].
4.6 Infection
Some researchers have found dynamic Gram-negative bacilli in the arterial and venous tissue culture fluid of certain Buerger’s disease patients. However, the evidence supporting infection, particularly fungal infection, as a significant cause of the disease remains insufficient.
4.7 Smoking
Smoking has been recognized as a primary causative factor in Buerger’s disease. Animal experiments using tobacco extract have successfully produced vascular lesions in rats. Skin tests with tobacco extract showed a high positive rate of 78–87% in Buerger’s disease patients compared to the general population, which was only 16–46%. According to domestic data, smokers account for 50–95% of the disease, and most of them have a history of heavy smoking. Some patients can improve their condition after quitting smoking, and smoking again can aggravate the symptoms of superficial phlebitis. These show that the onset of the disease is closely related to smoking. Smoking is recognized as the main pathogenic factor of TAO. Not only can smoke be directly sensitized, but nicotine can also be used as a hapten, which binds to histone or DNA in cells, changes the composition of its own tissues, and leads to the production of autoantibodies. Moreover, smoking can also reduce the oxygenation of arterial blood, increase blood viscosity, slow down blood flow, and constrict blood vessels. These phenomena are factors that cannot be ignored in the occurrence and development of vasculitis [5, 6].
Among the 876 cases counted by our hospital, 82% were heavy smokers, but 18% of the cases had never smoked. It shows that smoking is the main factor rather than the only factor.
4.8 Occupation
Workers, peasants, and soldiers accounted for the highest proportion of the number of patients. According to our patients data, they account for about 71–90%.
4.9 Region and race
Initially, the disease was believed to predominantly affect Jews, leading to the term “Jewish disease.” Later, it was associated with Eastern European countries, referred to as “Slavic disease” or “Russian disease.” However, recent data indicates that Burger’s disease can occur in any region and among any nationality. However, the incidence rates vary globally. The prevalence rates among all patients with peripheral arterial diseases have been reported to range from as low as 0.5–5.6% in Western Europe to as high as 45–63% in India. 16–66% in Korea and Japan, and 80% among Ashkenazi Jews [6], Thailand, Indonesia, and Malaysia, all have relatively high incidence rates [1, 7] as well as in China [3]. Recently, the incidence has declined; some authors believe it is related to a decrease in tobacco use, and some authors think it is related to economic development. As for the regional distribution of the disease in China, the disease appears more prevalent in the cold north of China.
4.10 Genetic factors
Some scholars were tested for various HLA antigens. They found that the incidence of HLA-A9 and HLA-B5 was significantly greater among those with Buerger’s disease than healthy controls and patients with atherosclerosis [8]. Similarly, in the Merseyside area of the UK, TAO patients exhibited significantly increased levels of HLA-A9 and HLA-B6 antigens. Individuals possessing the HLA-B5 antigen were found to have a relative risk of developing TAO that increased to 78.2 times compared to those without this.
Some scholars observed that HL-A antigen J-1-1 was significantly higher (P < 0.001) in Japanese patients with thromboangiitis obliterans (TAO) than it was in a population of normal Japanese. Also, antigens HL-A9 and W10 showed an increased occurrence in TAO patients. However, antigen HL-A12 was not found in TAO patients, but it occurred with a frequency of 20% in the normal population [9]. Some scholars reported patients with TAO had a statistically significantly higher frequency of HLA-DR4 and a significantly lower frequency of the HLA-DRW6 antigen than had both control groups [5].
It is believed immune dysregulation and blood hypercoagulability are very important.
5.1 Autoimmune disease caused by immune regulation disorders
Buerger’s disease is an autoimmune disease. And what is the immunological pathogenesis? Over the past 50 years, some scholars have enabled people to have a clearer understanding of the immune pathogenesis of TAO.
In 1962, Pokorny reported that antiarterial antibodies were detected in the blood of TAO patients with superficial migratory phlebitis [10]. Later, some Japanese scholars (1970–1976) obtained results of antiartrial antibodies in almost 50% or more of the patients with TAO. In 1979, Author Ping Zheng postulated that TAO is closely related to the immune mechanism based on the clinical course and pathological manifestation [11]. Culati et al. reported that blood IgG, IgA, and IgM increased, complement CH50 and complement C3 decreased significantly, and the inhibition of leukocyte migration was strengthened in TAO [12]. Later, he reported using indirect fluorescence technology to observe and found anti-IgG, IgA, IgM, and C3 component deposits on the wall of diseased blood vessels—presence of autoantibodies and immune complex in the sera of TAO patients [13, 14]. Bollinger et al. reported that more than 50% of TAO patients had increased antielastin antibodies, decreased complement C4, and 23% of patients had increased blood immune complex CTC [15]; Smolen et al. studied 20 cases of TAO, and detected anticollagen antibodies in seven cases (35%) There was no such antibody in the normal control group [16]. Some scholars have found more antibodies in TAO: antiendothelial cell antibody (AECA), antineutrophil cytoplasmic antibody (ANCA), antiphospholipid antibody (APA), G protein receptor antibody (AAB), etc. [17, 18, 19, 20, 21], suggesting that there are many these antibodies attack blood vessel endothelial cells and blood vessel walls.
Also, it has been reported that the role of interleukins [22], cell adhesion molecules [23], and decreased red blood cell immunity [24] on the vascular immune response.
In our study, Since the end of the 1970s, we have conducted comprehensive and systematic research on TAO immunity. We used cellular immunity (T cell rosette test E-RFC, T suppressor cell Ts, peripheral B lymphocytes with SmIg and SmIgG on their surface; leukocyte migration inhibition test, LMIT); humoral immunization (γ-globulin, immunoglobulin IgG, IgA, IgM, IgE, complement CH50, C3, C4, immune complex CIC); and immunopathology (light microscopy, electron microscopy, immunofluorescence IF, immunoenzyme-labeled staining ABC, immune gold and silver staining IGSS), as indicators, systematically observed TAO patients and its immunological changes in acute, subacute, and stable states [25, 26, 27].
5.1.1 A summary of our observed immunological changes in TAO patients
5.1.1.1 Cellular immunity
There is a significant decrease in T cells and Ts (P < 0.01), suggesting impaired cellular immune response.
B cells are increased (P < 0.01), indicating an immune response involving antibody production.
Lymphocytes show degeneration due to aorta antigen sensitization by LMIT.
LMIT demonstrates enhanced inhibition of leukocyte migration, indicating an immune response.
Under light microscopy, a large number of lymphocytes, as well as a few monocytes and neutrophils, are observed in all layers of the involved vessels (Figure 2).
Figure 2.
TAO patient’s vein wall thickening and edema, multifocal neutrophil, lymphocytes and a few monocytes, infiltration in the muscle layer, and intravascular thrombus beginning to organize (HE 125×).
5.1.1.2 Humoral immunity
There is a significant increase in the levels of γ-globulin (P < 0.01), indicating an immune response.
Elevated levels of immunoglobulins IgG and IgE are observed (P < 0.01).
The presence of elevated immune complexes CIC is detected (P < 0.05), particularly in the acute stage of TAO (P < 0.01), suggesting immune system activation.
Deposition of immune complexes (CIC) is observed in the blood vessel walls of TAO patients, as confirmed by electron microscopy (Figure 3) and three immunolabeling techniques (DIF, ABC, IGSS) (Figures 4-6).
Antivascular autoantibodies are found to directly bind with damaged vascular collagen, as demonstrated by three immunolabeling techniques (Figures 7-9).
The presence of antivascular autoantibodies in the serum of TAO patients is detected by three immunolabeling techniques, accounting for 72–89% (P < 0.01) (Table 1).
Figure 3.
Deposited with high electronic density lump substance in media corresponding to the area of immunofluorescence deposit in TAO (7490×).
Figure 4.
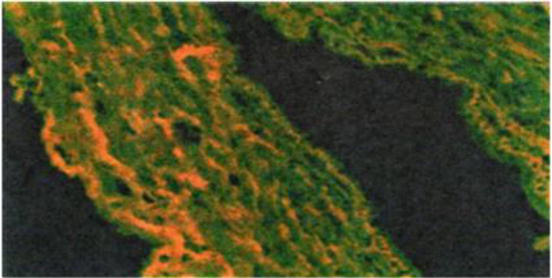
The deposition of yellow-green striped, plaque-like, and granular immune complex fluorescent substances can be seen in the intima, middle layer, and outer layer of blood vessels of TAO (DIF 400×).
Figure 5.
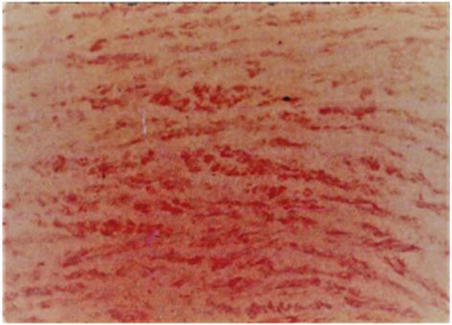
Streaky and massive brown-yellow immunoenzyme-labeled staining substances deposited on the vessel wall of TAO (ABC 400×).
Figure 6.
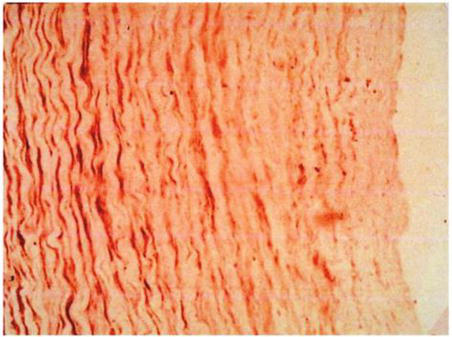
Black stripes and granular immune gold and silver staining substances were deposited on blood vessels of TAO (IGSS 400×).
Figure 7.
Antivascular antibodies are present in the sera of TAO patients, showing that the secondary antibody yellow-green FITC-antibody binds to the vessel wall of TAO (DIF 200×).
Figure 8.
Antivascular antibodies are present in the sera of TAO patients, showing that the second antibody brown-red antibody binds to the vessel wall of TAO (ABC 200×).
Figure 9.
Antivascular antibodies are present in the sera of TAO patients, showing secondary antibody dark brown gold-antibody bound to the vessel wall of TAO (IGSS 200×).
Patient group
Normal group
P value
Items
Number of cases
Positive
%
Number of cases
Positive
%
IF
32
23
72
13
2
18
<0.001
ABC
28
21
75
13
3
23
<0.001
IGSS
28
24
86
11
0
0
<0.001
Table 1.
Detection of antivascular autoantibodies in serum of TAO patients.
5.1.2 Conclusions drawn from the provided information
5.1.2.1 Type III hypersensitivity reaction
The presence of antigen-antibody complexes deposited on the vessel wall, confirmed by three immunolabeling techniques and electron microscopy, suggests a type III hypersensitivity reaction in TAO.
5.1.2.2 Type II hypersensitivity
The observation of antivascular autoantibodies directly binding to damaged vascular collagen indicates the existence of type II hypersensitivity in TAO, which was also confirmed by three immunolabeling techniques.
5.1.2.3 Type I hypersensitivity
Elevated levels of IgE and the presence of repeated acute attacks in TAO patients, triggered by factors like tobacco, weather, trauma, and malnutrition, suggest the involvement of type I hypersensitivity. This indicates that the patients may be in a sensitized condition.
5.1.2.4 Type IV delayed hypersensitivity
The results of LMIT show that lymphocytes of TAO patients can be degenerated by aorta antigen sensitization. In light microscopy, lymphocyte infiltration is mainly shown. This, combined with the clinical manifestation of repeated attacks of superficial phlebitis with nodules accompanied by skin inflammation and swelling, suggests the involvement of type IV delayed hypersensitivity. The release of lymphokines by sensitized lymphocytes may contribute to the observed symptoms.
According to clinical studies, patients with TAO have recurrent episodes of superficial phlebitis nodules. The skin on the surface of the nodules is inflammatory and edematous, which may be caused by the release of lymphokines by sensitized lymphocytes. According to light microscopy, lymphocyte infiltration is mainly shown and combined with the results of LMIT. It has also been shown that the lymphocytes of TAO patients can indeed be sensitized by the antigens of the denatured aorta, and the inhibition of leukocyte movement is strengthened.
In summary, TAO appears to involve a combination of type III, type II, type I, and type IV hypersensitivity reactions [25, 26, 27].
5.1.3 TAO exhibits characteristics commonly associated with autoimmune diseases
5.1.3.1 Hyperglobulinemia
In TAO, an increase γ-globulin is detected in the blood. γ-globulin is responsible for antibody production, and elevated levels can be observed in various autoimmune diseases.
5.1.3.2 Presence of autoantibodies and sensitized lymphocytes
Autoantibodies are antibodies that mistakenly target and attack the body’s own tissues. The presence of autoantibodies and sensitized lymphocytes indicates an immune response against self-antigens, which is a hallmark of autoimmune diseases.
5.1.3.3 Antigen-antibody complexes deposit in damaged tissues
In autoimmune diseases, immune complexes formed by the binding of antigens and antibodies can accumulate in tissues, leading to inflammation and tissue damage.
5.1.3.4 Infiltration of immune cell in target organs
Autoimmune diseases often involve the infiltration of immune cells, such as lymphocytes and monocytes, into the affected organs or tissues.
5.1.3.5 Variety of autoantibodies in TAO patients
The presence of multiple autoantibodies further supports the autoimmune nature of TAO.
5.1.3.6 Genetic predisposition
Like many autoimmune diseases, TAO is also believed to have a genetic component, indicating that certain genetic factors may contribute to its development.
5.1.4 The clinical characteristics of TAO associated with autoimmune diseases
5.1.4.1 Recurrent attacks and chronic protracted process
In our patients with TAO have number of recurrences: one to six times and attack episode duration 1–10 months.
5.1.4.2 Response to immunoadsorption and immunosuppressants during acute attacks
Some researchers have reported that the use of immunoadsorption can help control the progression of TAO disease [28]. Additionally, the author has found that compounds containing immunosuppressive and anticoagulant medications can also effectively manage the development of TAO disease.
5.1.4.3 Presence of TAO in both limbs and internal organs
More and more scholars have reported that TAO not only invades the limbs but also invades visceral blood vessels [29].
5.1.4.4 Association with certain triggering factors
Smoking is recognized as the main pathogenic factor of TAO. Not only can smoke be directly sensitized, but nicotine can also be used as a hapten, which binds to histone or DNA in the cell, changes the composition of its own tissue, and leads to the production of autoantibodies.
5.1.4.5 Changes in sex hormones and autoimmune diseases
Changes in sex hormones can lead to autoimmune diseases [30]. In our cases, 94.5–99% of TAO patients are young and middle-aged men.
5.1.5 In conclusion
Combined, our study identified TAO as an autoimmune disease involving multiple hypersensitivity reactions. Mainly, type III hypersensitivity, in addition to type IV hypersensitivity, also has type II hypersensitivity, and there is the involvement of type I hypersensitivity [25, 26, 27].
5.2 TAO blood in hypercoagulable state
In the 1980s, we systematically studied and measured blood hypercoagulation indicators in patients with TAO, including blood coagulation, anticoagulation, platelet function, and blood rheology. We found that out of 14 indicators, 10 exhibited abnormalities [31]:
Platelet aggregation (PAgT) increased (P < 0.05, P < 0.01)
Whole blood and plasma viscosity increased (P < 0.01)
Red blood cell electric pulse time prolonged (P < 0.01)
Fibrinogen increased in the disease state (P < 0.01)
Thromboelastography (TEG) abnormalities
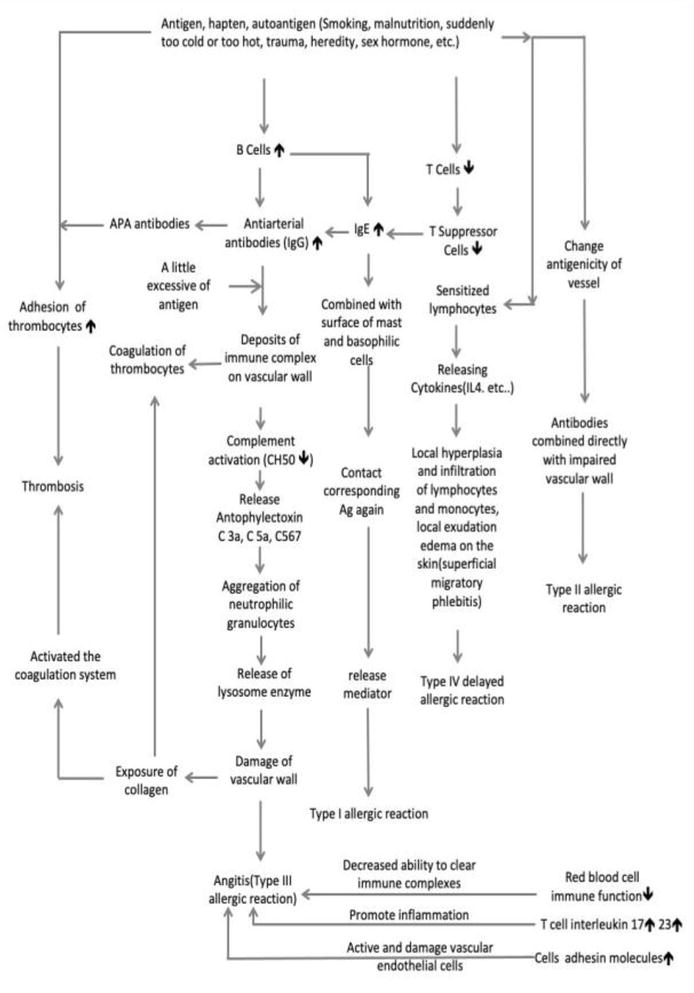
These abnormalities collectively indicate a state of blood hypercoagulability in patients with Buerger’s disease, rendering them more susceptible to the formation of thrombi within affected blood vessels. Regarding the relationship between thrombosis and immune-vasculitis in Buerger’s disease, it is believed that immune-vasculitis plays a dominant role, and the consequences of various hypersensitivity reactions lead to blood hypercoagulability and thrombosis within the vascular (Figure 10).
Figure 10.
Conceptual diagram of the pathogenesis of thromboangiitis obliterans (designed by Ping Zheng and Wanchao Wang in 1985, revised in 2020).
6. Implications for diagnosis and treatment of TAO
In the final section of this chapter, we discuss the far-reaching implications of our findings for the diagnosis and treatment of Buerger’s disease. Our research provides a solid foundation for the development of diagnostic tools and therapeutic interventions, ultimately improving the outlook for individuals afflicted by this challenging autoimmune disorder.
6.1 Cellular and humoral markers and targeted diagnosis of TAO
The understanding of TAO as a distinct disease separate from other vascular disorders (there is basically no debate among scholars) is relatively recent, dating back about 50 years. Its regional characteristics and varying prevalence in different parts of the world have contributed to slower progress in research. Although the disease is very painful and the amputation rate is high.
In the past four decades, research on the immune pathogenesis of TAO has shifted from scattered detection methods to more comprehensive and in-depth investigations. Scientists have discovered certain cellular and humoral markers associated with the disease.
6.1.1 Cellular markers
Cellular markers refer to specific types of immune cells that are involved in the inflammatory process of TAO. The presence of certain immune cells, such as neutrophils and T lymphocytes, within the affected blood vessels, suggests their role in the disease pathogenesis. Detecting and analyzing these cellular markers can provide insights into the immune response.
6.1.2 Humoral markers
Humoral markers, on the other hand, refer to molecules present in the blood circulation that are associated with the disease. As mentioned earlier, markers such as antivascular antibodies and antigen-antibody complexes have been found to deposit on the walls of blood vessels in TAO. These humoral markers indicate an immune response targeting the vascular endothelium and contribute to the inflammatory process and vessel occlusion seen in the disease.
Furthering efforts to the identification and detection of TAO-specific diagnostic markers from blood circulation are crucial for improving the diagnosis of the disease. By developing reliable and specific tests to detect these markers in the blood circulation, healthcare professionals can potentially diagnose TAO earlier, leading to timely interventions and a reduction in the high amputation rates associated with the disease.
6.2 Treatment of TAO
6.2.1 Avoid triggers of vascular inflammation
Avoid factors that can trigger vascular inflammation, such as nicotine, exposure to sudden cold and sudden heat, and trauma. Smokers should quit smoking immediately and take measures to prevent exposure to temperature extremes and trauma.
6.2.2 Blocking vascular inflammation and thrombus formation
Appropriate amounts of hormones and anticoagulant drugs can be applied. The author created this kind of compound medicine that has shown promising results without significant side effects. The author has used large doses of anisodamine to treat TAO in subacute and chronic states, with positive outcomes due to its immune regulation function and ability to reduce blood hypercoagulation [32].
6.2.3 Effective pain relief methods
Effective pain relief is crucial, as severe pain in the affected limb is a major reason for amputation. Anesthesia methods created by the author using a small dose of Traditional Chinese medicine have shown good analgesic effects. This method also promotes blood circulation and regulates immune function. Thereby increasing skin temperature, eliminating limb edema, and improving knee joint flexion deformity [33].
6.2.4 Electroacupuncture
For patients in the subacute or chronic stable stage of TAO, high-frequency electroacupuncture on the affected limbs can improve limb circulation and regulate immune function, leading to increased skin temperature and improved intermittent claudication [34].
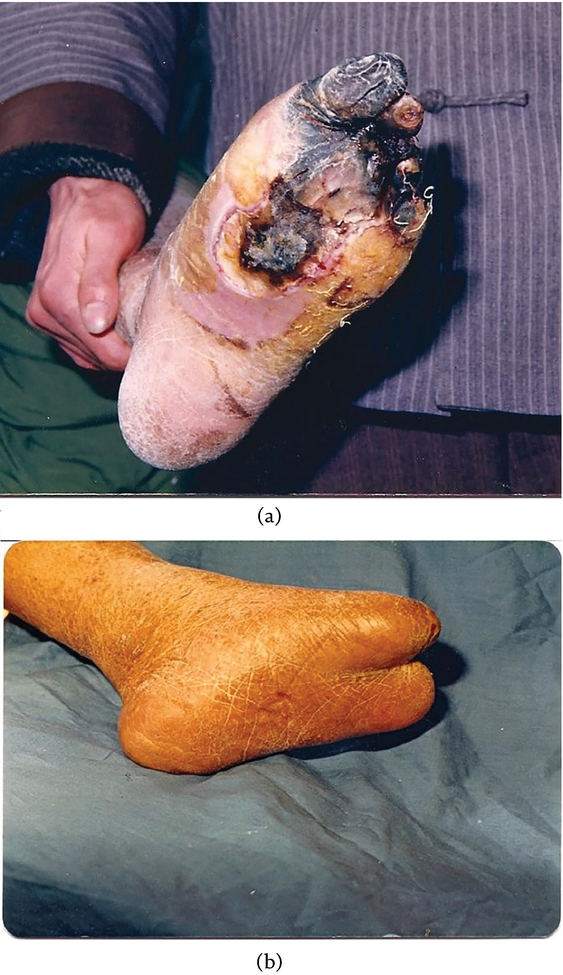
Comprehensive treatment combining these above methods can significantly improve therapeutic outcomes, reduce patient pain, and decrease the amputation rate (Figures 11 and 12).
Figure 11.
(a) Before treatment: The patient had lower limb ischemia causing All toes necrosis, extending to the plantar region. (b) After our treatment: Gangrene progression is controlled, and major amputation was avoided, preserving the heel and plantar region.
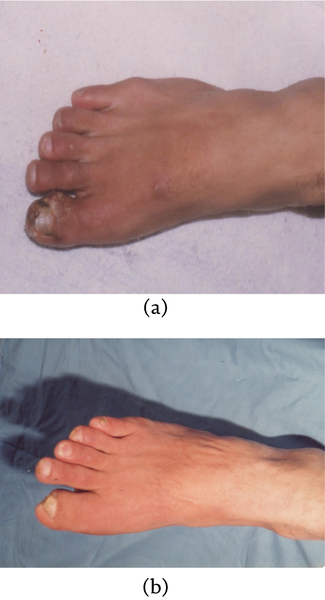
Figure 12.
(a) Before treatment: The patient experienced lower limb ischemia resulting in a painful ischemic ulcer on the big toe. (b) After our Treatment: improved limb blood circulation controlled the ulcer’s progression, ultimately leading to its complete resolution.
Of the 1200 cases we treated, the amputation rate of the thigh and legs above the ankle was 1.2%, and the mortality rate was 0% [35].
This chapter’s comprehensive exploration of the autoimmune nature of thromboangiitis obliterans (TAO), its intricate involvement of the immune system and secondary blood coagulation pathways, as well as the influences of genetics and the environment, collectively lays a solid foundation for future research endeavors. Moreover, these insights hold significant promise for the advancement of diagnostic techniques and the development of potential therapeutic interventions.
We are sincerely grateful to Li Li and YaLi X of the Shanghai Institute of Immunology for their collaboration in some immunological techniques; Professor BaoLi M for her instruction; Professor SaiJuan C of Rui-jin Hospital for TAO blood test cooperation; Professor XueMin T for observing vasseles under eletron microscopy; Professor BinHua S for statistical processing. Dr.JinMing G for assisting in organizing original data.
The authors declares that they have no competing interests.
References
1.Joseph L, Sr M. Buerger's disease in the 21st century: Diagnosis, clinical features, and therapy. Seminars in Vascular Surgery. 2003;16:179-189
2.Faeze F, Fi B. Visceral bed involvement in thromboangiilis obliterans: A systematic review. Vascular Health and Risk Management. 2019;15:317-353
3.Ping Z. Etiology and pathogenesis of thromboangiitis obliterans (TAO). North Medicine (Chinese). 1983;5:13-15
4.JiaJu W, Zao Wenguang Z, Siqiaoun S, Yang Z. Changes in the incidence of thromboangiitis obliterans. Chinese Journal of Vascular Surgery. 2009;1:9-12
5.Papa M, Bass A, Adar R, Halperin Z, Schneiderman J, Becker CG, et al. Autoimmune mechanisms in thromboangiitis obliterans (Buerger's disease): The role of tobacco antigen and the major histocompatibility complex. Surgery. 1992;111(5):527-531
8.McLoughlin GA, Helsby CR, Evans CC, Chapman D. Association of HLA—A9 and HLA—B5 with Buerger's disease. British Medical Journal. 1976;2:1165-1166
9.Ohtawa TT, Kawano N, Mishima Y, Tohyama H, Ishikawa K. HLA antigens in thromboangiitis obliterans. Journal of the American Medical Association. 1974;230(8):1128
10.Pokorny J, Jezkova Z. Significance of immunological studies in peripheral obliterating vascular diseases. Circulation Research. 1962;11(6):961
11.Ping Z. Treatment and prevention on TAO with Chinese traditional medicine combine with Western medicine. Compiled per TAO Experience Exchange Symposium (Chinese). Ji Nan China. 1976:125-133
12.Gulati SM, Madhar K, Thusoo TK, Nair SK, Saha K. Immunological studies in thromangiitis obliterans (Buerger's disease). The Journal of Surgical Research. 1979;27:287
13.Gulati SM, Madhar TK, Nair SK, Saha K. Autoantibidies in thromboangiitis obliterans (Buerger's disease). Angiology. 1982;33(10):642-651
14.Gulati SM, Saha K, Kant L, Thsoo TK, Prakash A. Significance of circullatory immune complexes in thromboangiitis obliterans (Buerger's disease). Angiology. 1984;35(5):276-281
15.Bollinger A, Piquerez MJ, Largiader J, Schneider E. Buerger's disease present diagnostic and therapeutic method. Annales de Médecine Interne. 1983;134(5):436-440
16.Adar R, Papa MZ, Halpern Z. Cellular sensitivity to collagen in thromboangiitis obliterans. New England Medicine. 1983;308(19):1113-1123
17.Eichhorn J, Sima D, Lindschau C, Turowski A, Schmidt H, Schneider W, et al. Antiendothelial cell antibodiin thromboangiitis obliterans. The American Journal of the Medical Sciences. 1998;315:17-23
18.Halacheva KS, Manolova IM, Petkov DP, Andreev AP. Study of anti-neutrophil cytoplasmic antibodies in patients with thromboangiitis obliterans (Buerger’s disease). Scandinavian Journal of Immunology. 1998;48:544-550
20.de Godoy JM, Braile DM. Buergerʼs disease and anticardiolipin antibodies. Journal of Cardiovascular Medicine. 2009;10:792-794
21.Klein-Weigel PF, Bimmler M, Hempel P, Schöpp S, Dreusicke S, Valerius J, et al. G-protein coupled receptor auto-antibodies in thromboangiitis obliterans (Buerger's disease) and their removal by immunoadsorption. VASA. 2014;43:347-352
22.Dellalibera-joviliano R, Joviliano EE, Silva JS, Evora PR. Activation of cytokines corroborate with development of inflamation and autoimmunity in thromboangiitis oblierans patients. Clinical & Experimental Immunology. 2012;170:28-35
23.Zheng W, Wenjing J, Hengzhen W, Li H, Bo T, Bing L, et al. The IL-6/Stat3 pathway regulates adhesion molecules and cytoskeleto endothelial cell in throboangiitis obliterans. Cellular Signalling. 2016;44:118-126. DOI: 10.1016/j.cellsig.2018.01.015
24.Xiangmao F, Zaiping J, Feng G. Erythrocyte immune function and regulatory factors in patients with thromboangiitis obliterans (Chinese). Shanghai Medicine. 1987;20:403-404
25.Ping Z, PeiBing F, Wang W, WunYu X, Ton XM, Ming Y, et al. Observation on the immune function status of thromboangiitis obliterans (Chinese). Journal of Shanghai Immune. 1985;5(3):146-150
26.Ping Z, PeiBin F, Wang W, WenYu X, XueMing T, Ming Y, et al. Immunological studies on thromboangiitis obliterans. Chinese Medical Journal. 1989;102(2):129-136
27.Ping Z, Wang W. Buerger's disease: Autoimmune disease involving multiple hypersensitivity types. Journal of Clinic Research. 2022;6:S1
28.Bauman G, Verena S, Peter KW, Karl S. Successful treatment of throboangiitis obliterans (Buerger's disease) with immunoadsorption: Results of a pilot study. Clinical Research in Cardiology. 2011;100:683-690
29.Ping Z, LiNian Z. Thromboangiitis obliterans with myocardial infarction in 3 case. Cardiovascular Diseases. 1978;6:19-21
30.Sun K, Feng Q , Dou K. The relationship between the immunomodulatory effects of sex hormones and the occurrence of diseases (Chinese). Chinese Journal of Preventive Medicine. 2002;36(6):421-423
31.Ping Z, SaiJuan C, HaiZheng C. Studies on hypercoagulation state in Buerger’s disease. Chinese Medical Journal. 1989;102(1):67-71
32.Ping Z. High-dose anisodamine in the treatment of 62 cases of thromboangiitis obliterans (Chinese). Chinese Emergency Medicine. 1990;10(1):3-6
33.Ping Z. Traditional Chinese medicine anesthesia in severe thromboangiitis obliterance. Chinese Medical Journal. 1988;101(3):221-224
34.Ping Z. Thromboangiitis obliterans (Chinese). In: Zhenyi W, editor. Thrombosis and Hemostasis. Shanghai of China: Shanghai Science and Technology Press; 1988. pp. 246-254. ISBN:7-5323-0346-2
35.Ping Z. Comprehensive treatment of thromboangiitis obliterans with integrated Traditional Chinese and Western medicine (Chinese). In: The Ninth National Surgery Academic Conference. Wu Han, China 1978 Proceedings of Abstract. p. 19
Written By
Ping Zheng and WanChao Wang
Submitted: 10 July 2023Reviewed: 07 August 2023Published: 05 January 2024
 Open access peer-reviewed chapter
Open access peer-reviewed chapter