Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
To purchase hard copies of this book, please contact the representative in India:
CBS Publishers & Distributors Pvt. Ltd.
www.cbspd.com
|
customercare@cbspd.com
Chagas disease (CD) is an infectious illness with great socioeconomic impact. Historically, it has mainly affected the poor population in Latin America. However, globalization sets a new scenario, featuring an increasing CD incidence worldwide especially due to parasite transmission by infected blood in non-endemic countries. Noteworthily, CD is predominantly marked by a subclinical progression, so that for most cases, the correct diagnosis may take years, even decades, post-infection. Public actions such as active search of infected people and donors screening are imperative for both identification of individual health assistance and disease control. Nonetheless, the main affected areas lack laboratory infrastructure, resource, and specialized personnel, making the use of conventional immunoassays unfeasible. Moreover, parasite genetic variability and cross-reaction with close-related infectious diseases impose a stringent diagnosis algorithm. Thus, although rapid tests are a great option, its applicability is still restricted in the context of this disease. In this regard, this chapter will discuss the use of immunochromatographic-based assays for CD, their limitations, and perspectives. The performance of commercially available kits in comparison to the conventional serologic tests will be also debated, covering their antigen selection, origin of population studied, and type of samples.
Oswaldo Cruz Institute-Fiocruz, Rio de Janeiro, Brazil
Ana Luiza Barbosa Godart Cavalcante
Oswaldo Cruz Institute-Fiocruz, Rio de Janeiro, Brazil
Rubem Figueiredo Sadok Menna-Barreto*
Oswaldo Cruz Institute-Fiocruz, Rio de Janeiro, Brazil
*Address all correspondence to: rubemsadok@gmail.com
1. Introduction
Chagas disease (CD) is a systemic illness caused by the hemoprotozoan Trypanosoma cruzi [1]. Its classical infection route is vectorial, depending on the contact of the vertebrate host with triatomine bugs’ feces containing the parasite [1]. Nowadays, oral infection plays an important role in CD transmission, especially in the Amazon region. Such a route also comprises a vector-dependent pathway, and it may take place upon ingestion of food or beverage contaminated by an infected insect [2, 3]. Therefore, CD has mainly affected the low-income population of rural areas where the favorable conditions for the triatomines are usually found intra or peridomiciliary, hence contributing to its establishment as endemic in Latin America [4]. Notwithstanding, while its incidence has been historically close related to socioeconomic and cultural factors, immigration has set a new epidemiological scenario [4, 5, 6]. Consequently, the profile of the infected people and at risk of acquiring the infection currently also includes population in urban centers, especially those from non-endemic countries, where the transmission occurs mostly by blood transfusion, solid organ transplantation, and from mother-to-child [5, 6].
Its clinical manifestations generally take years, or even decades, to occur and are predominantly related to chronic cardiac and/or gastrointestinal tissue damages, which are commonly associated with fibrosis and ganglion impairment [7]. Noteworthily, although only 30–40% of those infected present chronic signs and/or symptoms, its severity and incapacitation are enough to cause a global annual cost ranging billions of dollars (US$) owing to healthcare assistance and loss of productivity [8, 9, 10]. Thus, the propagation control of Trypanosoma cruzi infection is imperative.
In this regard, it is important to stress out that initiatives from Latin American countries, mainly based on vector control and screening of donors and pregnant women, resulted in a reduction of at least 62% of T. cruzi infection over the past 30 years [4, 10, 11]. However, the low rate of successful CD diagnosis (<10%) persists as a major obstacle to the interruption of infection dissemination [12]. Notably, two main factors are associated with disease diagnosis hindrance: (i) education of healthcare workers and technical training concerning CD aspects and detection of infection—especially in non-endemic regions, and (ii) the subclinical and slow-paced disease progression [13, 14]. To put it another way, the risk of infection remains permanent, or even greater in the case of non-endemic countries, because most people are oblivious to their own infection status, either due to a long-lasting asymptomatic clinical state, incorrect diagnosis, or lack of T. cruzi screening policies. Ergo, the majority of CD carriers do not receive the correct treatment.
The CD chemotherapy is based on only two drugs: benznidazole and nifurtimox. The efficacy of both nitroderivatives is greatly influenced by patient’s age and disease phase, so the sooner the medicines are taken, the higher the chances of cure [15, 16]. This is extremely important, as both drugs present limited activity in the chronic phase, especially in the symptomatic stage, besides severe side effects that commonly result in treatment abandonment [15, 16]. Public health initiatives are crucial to improve and increase early diagnosis rate and, consequently, timely treatment. However, in the meantime, CD remains the predominant cause of infectious cardiomyopathy in Latin America and a great burden in non-endemic countries [6, 17].
2. Standard methods and protocols for CD diagnosis
CD is marked by an acute and chronic phase, each with specific aspects that reflect the diagnostic methods of choice. Given that the onset of infection is characterized by a high parasitemia, the techniques related to direct parasite detection on peripheral blood by light microscopy comprise the gold standard for diagnosis during the acute stage, including in cases of congenital infection [18, 19]. Thus, the methods mainly applied are thin, thick, or fresh blood films. Alternatively, concentration methods, such as Strout and microhematocrit, may be employed [18, 19]. These protocols are especially indicated for the diagnosis of congenital infection and can be performed with either umbilical cord or venous blood from neonates and infants [20]. Polymerase chain reaction (PCR) can also be used, however, it should preferably be carried out within the first and third months of life [20]. In addition, serological follow-up is indicated for infected infants as well as for those with negative direct parasite detection with an infected mother. This analysis should be performed from the eighth month of life, when maternal IgG is no longer detected [20, 21].
In contrast, the chronic phase features a subpatent parasite load. In this sense, indirect detection methods that rely on parasite amplification, such as hemoculture, xenodiagnosis, and PCR, may be performed [19]. However, these tests show low sensitivity at this stage, so that a negative result has poor conclusive value to discard infection [19]. As the end of the acute phase is accompanied by seroconversion, the chronic stage is characterized by a continuous production of IgG. Ergo, diagnosis of suspected cases of long-lasting infections is predominantly based on immunoassays. Nevertheless, there is no gold standard or reference test since none of the kits commercially available exhibit ideal performance regarding both sensitivity and specificity [19]. Consequently, at least two tests must be performed, so that infection is either confirmed or ruled out only if both assays present the same profile of reactivity (positive or negative, respectively) [18]. Hence, when inconclusive results are obtained, another test must be carried out [18]. The immunoassays applied must necessarily differ in terms of either detection principles or antigenic set and present complementary sensitivity and specificity [18]. Furthermore, in the absence of a biomarker for cure, conversion to non-reactive profile in subsequent tests in an interval of time has been considered a parameter to confirm the parasite elimination by trypanocidal treatment [22].
Although indirect hemagglutination (IHA) and indirect immunofluorescence (IIF) are frequently used, enzyme-linked immunosorbent assay (ELISA) is the most employed method, once (i) it is better suited for large-scale analysis and (ii) presents a considerable variety in terms of antigenic preparations [23]. In addition, chemiluminescent microparticle immunoassay (CMIA) and western are also recommended, the latter mainly employed as a confirmatory assay and/or discriminatory test in inconclusive cases [18, 19].
ELISA kits are produced with either (i) whole parasite extract, (ii) semi-purified fractions, (iii) recombinant proteins (full-length or chimeras), or (iv) synthetic peptides—the latter two being commonly used as multiplexed formulations. Alternatively, combining purified homogenate with recombinant proteins is employed as well [23]. This flexibility is a major advantage given that test reactivity may vary according to sample origin due to host genetic background and/or differences among parasite strains. As a matter of fact, T. cruzi presents a wide genetic variability, so that populations are classified into six groups named discrete typing units (DTU) TcI-VI and Tcbat [24], which exhibit different geographical prevalence [25, 26]. Moreover, the diversity of ELISA kits also covers the necessary arrangement of sensitivity and specificity complementation. In this regard, the implementation of recombinant proteins and synthetic peptide have shown to improve test accuracy by reducing cross-reactivity with other diseases, especially leishmaniasis [19].
Noteworthily, the protocol for the screening process in blood banks and prenatal care—as a health policy measure to reduce T. cruzi infection dissemination—rely on the application of a single immunoassay, which must present a high sensitivity. In this context, ELISA and CMIA are the main recommended methods [18]. Nonetheless, in case of a positive result, another test must be carried out to confirm the diagnosis.
3. Applicability of rapids tests and its perspectives in CD context
Considering that those most affected by CD are from either remote areas or small towns with low resource in developing countries, the main immunoassays used for diagnosis and screening purposes do not meet the reality of local points of care, which commonly lack the needed infrastructure and the specialized personnel [27]. Furthermore, field studies are also hampered, as these tests are usually performed with plasma or serum obtained from venous blood extraction [28]. Thus, even if the assay is not carried out locally, transport of materials and equipment for sample adequate handling and storage are still required, as well as a trained team, which often translates in logistic complexity and, ultimately, in higher cost. More importantly, depending on the notification system applied, patient acknowledgment regarding their results is not safely guaranteed when the tests are performed latter on. Consequently, there is a patent demand for rapid tests [29], which have as basic concept a cheap and fast assay, with an easy development that ideally eliminates the necessity of specialized technicians, equipment, including in terms of sample manipulation, and cold storage, enabling their use on-site [30].
The World Health Organization and the Pan American Health Organization’s guidelines consider rapid tests as an alternative screening method for ELISA only in the context of seroepidemiological studies [18]. Their use is not recommended for clinical diagnosis or screening in hemotherapy services based on (i) the detection variation, (ii) the increased false negative rate (2–7 per 1000) in comparison to the association of two conventional serological methods for diagnosis of chronic patients and (iii) the cost-effectiveness, especially when there is a high demand, such as in blood banks [18].
Nonetheless, in 2005, the Chagas National Program of Bolivia incorporated the use of a specific rapid test (Chagas Stat-Pak, Chembio Inc.) as the frontline method in both clinical practice and seroepidemiological surveys [31]. Notably, Chagas Stat-Pak (CSP) has shown sensitivity and specificity ranging from 93.4 to 100.0% and from 97.3 to 99.3%, respectively, among Bolivian municipalities [28, 31, 32, 33]. However, to follow the recommended diagnosis algorithm, positive cases still must be confirmed by a conventional immunoassay [31]. In this sense, studies have shown promising results regarding the synchronous combination of two rapid tests with different antigen composition as an alternative strategy for definitive diagnosis in low-resources settings in Bolivia, Argentina, and Colombia [28, 31, 34, 35, 36, 37]. The association of two rapid tests displayed ≥93.3% of diagnostic efficiency when using results obtained by at least two conventional immunoassays as reference [28, 31, 35, 36]. This alternative protocol has a great advantage in speeding up the process of patient continued medical assistance, especially regarding the offer of trypanocidal drugs and, eventually, other necessary treatments. In line with that, the combination of rapid testing with electrocardiogram (ECG) performed by a mobile device was also evaluated in Bolivia [38]. Interestingly, out of the 25 people with ECG abnormalities compatible with chagasic chronic cardiomyopathy, 22 (88%) presented a positive profile on the rapid test. As per the current protocol, the diagnosis of these patients was later confirmed by ELISA. ECG was carried out in a device connected to a smartphone and processed by a medically certified app; the exams were performed by non-physicians in a remote area, however, within 24 h the data were analyzed, and results were reported by cardiologists located overseas [38]. Taking into account the lack of clinical tools for patient’s progression monitoring toward symptomatic stage [22, 39, 40, 41], the incorporation of already known potential protein markers for such questions, especially those for early cardiac impairment [42, 43], in rapid test is an appealing and strategical approach to improve the assistance of individuals infected and should be addressed in the near future.
In view of congenital transmission, rapid testing has also been evaluated in Latin American pregnant women, mainly at the time of delivery [44, 45, 46, 47, 48]. This practice has a great impact on disease control when the mother was not tested during prenatal care, once trypanocidal efficacy is high and well tolerated by infants [20, 48]. Surprisingly, reported data indicates that a rapid test outperformed ELISA assays [45, 46]. Furthermore, aiming to investigate the recovery time of newborns infected congenitally and submitted to trypanocidal treatment 1 day after birth, Chippaux et al. [21] monitored periodically the level of specific anti-T. cruzi antibodies by ELISA; newborns without infection, but with an infected mother were included as control. From the eighth month, the authors carried out rapid testing in parallel to the conventional assay. At the ninth month, none of the patients showed immunoreactivity in the rapid test, while 12% remained testing positive by ELISA. Within the following 7 months, all of these patients presented antibodies titres below the ELISA cut-off [21]. This delayed seronegativity may be related to the extended set of antigens and/or the different epitopes components of the ELISA kit in comparison to the rapid test used. Moreover, anti-T. cruzi IgG originally from the mother was not detected in the mentioned control group since the fifth month despite the continued breastfeeding [21]. Conversely to the observed in infants, Jackson et al. [49] still detected reactivity in 2 ELISA assays and in the same rapid test when applying sera from adults of endemic regions after 3 years of treatment with nifurtimox.
Up on the released data reporting rapid tests performance on endemic population, a health center in Geneva, Switzerland, sought to study its feasibility regarding the screening of Latin American immigrants [50]. The majority of infected individuals was from Bolivia, and as a result of the rapid testing agreement with the conventional immunoassays and reproducibility, it was incorporated at the hospital as a point-of-care test in both the primary care center and the maternity ward (testing at delivery) [50]. In Italy, a different test has shown high specificity and was used as a third assay for evaluation of samples with discordant results [51], while in Spain, a rapid test was applied to screen co-infection in Latin Americans immigrants diagnosed with HIV [52].
4. Performance of immunochromatographic rapid tests commercially available
As previously mentioned, parasite and/or host genetic background may be related to reactivity discrepancy. Thereby, it is strongly suggested that the rapid test is field validated in the area of interest before officially incorporating its use [31, 35]. This process should ideally be carried out at a national level by encompassing different sites [31], once circulating strains may vary from one region to another within the endemic countries [24, 25]. Thus, this topic is focused on the main marketed rapid tests with reported performance studies (Table 1).
Rapid test commercially available for CD diagnosis that present performance reports in the literature.
Studies performed at endemic regions that included samples from at least two different countries.
Studies that incorporated surveys of Latin American samples in non-endemic regions.
Type of sample, volume, and reaction time were informed as described in the respective reference.
Sensitivity (SS) and specificity (SP) ranges are displayed based on the overall results obtained in the studies mentioned. Vol: volume; RT: reaction time; S, P, and WB: serum, plasma, and whole blood, respectively; LATAM: Latin America; NS: not specified.
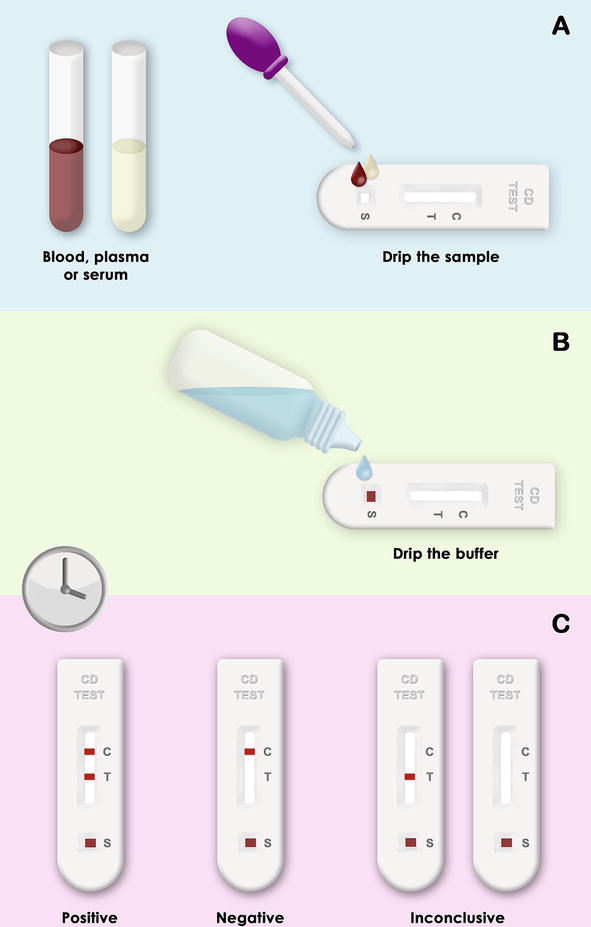
These assays are based on the detection of anti-T. cruzi antibodies circulating in the bloodstream upon recognition of recombinant proteins (Figure 1). In the absence of a gold standard immunoassay, conventional serology methods have been used as reference to evaluate rapid test performance (Table 2). Generally, the tests can be carried out with small volumes (5 to 100 μL) of either plasma, serum, or whole blood (Table 1). However, the latter comprises the best working sample type as it does not require further processing and, in the case of immediate testing, it may be obtained from fingertip puncture, perfect for the context of the field research. Moreover, the results are obtained within 10–35 min (Table 1).
Figure 1.
Rapid testing scheme. (A) Either plasma, serum or whole is placed onto the sample site (S) and after (B) the addition of buffer, the molecules flow laterally through the membrane by capillary. (C) Within minutes, the results are obtained and can be interpreted by naked eye. Those positive comprise at least two bands, referring to the control line and the antigen detected by the anti-Trypanosoma cruzi IgG. Notably, the test can have more than one epitope separated in different reaction areas. A result is stated as negative when only the control line is apparent, and an assay is determined as inconclusive when the control line is not detected.
Conventional immunoassay used as reference to evaluate rapid test performance.
Recombinant protein composed by Pep 2, TcD, TcE and SAPA antigens.
Methods without clear reference of a commercial kit were considered as in-house assays.
Those applied as confirmatory are also included [45, 57, 65, 69]. ELISA: enzyme-linked immunosorbent assay; E-CLIA: electrochemiluminescence immunoassay; GA: gel agglutination; IHA: indirect hemagglutination; IIF: indirect immunofluorescence; CSP: Chagas Stat-Pak; CDP: Chagas Detect Plus; TD: Trypanosoma detect; SSC: simple stick Chagas; SCWB: simple Chagas WB; SD Bioline: SD Bioline Chagas Ab; OnSite: OnSite Chagas Ab Combo; NS: not specified; TIIC: Tecnologia Imunológica Indústria e Comércio.
CSP detection capability relies on the recognition of the recombinant antigens B13, 1F8, and H49/JL7 [53]. Notably, it has been trending as the most evaluated rapid test in both field and clinical seroprevalence studies, including in non-endemic countries. By using serum as testing sample, CSP has shown sensitivity ranging from 97.1 to 100.0%, and specificity from 94.8 to 99.9% among populations from South and Central Americas [53, 54]. Surprisingly, reactivity of samples from Midwest and Northeast regions of Brazil resulted in 98.5 and 94.8% of sensibility and specificity, respectively [53], even though the epitope B13 is derived from a 140 kDa protein detected in the surface of Y strain trypomastigotes [55], which belongs to one of the predominant DTUs in the respective area [24, 25]. Furthermore, sera from El-Salvador displayed the lowest sensitivity (97.1%) [53]. In a multicenter study carried out by Sánchez-Camargo et al. [56] with sera tested in national reference laboratories for Chagas disease diagnosis located in Brazil, Argentina, Colombia, Costa Rica, Mexico, United States of America, France, Spain, and Japan, the CSP exhibited 87.2 and 93.2% of sensibility and specificity, respectively [56]. On average, 50 samples (ca. of 25 positive and 25 negative) per region were analyzed, however, neither the origin of the donors sorted by each facility in non-endemic areas nor the correspondent data per country was discriminated. The reduced performance was accounted to sera selection, which comprised samples stored for averagely 2 years and with moderate to low reactivity profiling. The later aspect is of major importance, once one cannot rule out that methods used for sample reactivity classification could vary among the laboratories enrolled [56]. Curiously, this study also reported a lower sensitivity when using plasma in comparison to serum, while two other studies have demonstrated high level of agreement (99.7–100.0%) among different sample types (sera stored with or without 50% glycerol, plasma, whole blood and/or eluates from filter paper containing dried whole blood) [50, 53]. In this regard, CSP exhibited outstanding results (100.0% for both sensitivity and specificity) in whole blood testing in Colombia [35].
Interestingly, analysis of CSP in surveys of Latin Americans living in non-endemic countries showed a predominant seroprevalence in Bolivian immigrants [34, 50, 57]; sera testing presented low performance [34], while whole blood accused a sensibility and specificity of 95.2 and 99.9%, respectively, being 97.2% of the positive results from Bolivian origin [50]. By the time the CSP was implemented as a diagnostic tool by the Bolivian Ministry of Health, only one of the studies conducted so far had included samples from such region (n = 21) [53]. Therefore, since then, studies have been done to evaluate and field validate CSP performance in different Bolivian sites. Most of these works used whole blood for the CSP testing and either serum or plasma for conventional serological assays taken as reference. As previously mentioned, detection performance varied among municipalities, with sensibility and specificity ranging from 93.4 to 100.0% and from 97.3 to 99.3%, respectively [28, 31, 32, 33]. Noteworthily, lower sensitivities were obtained by Roddy et al. and Chippaux et al. when working with age groups ranging from 9 months to 17.9 years old (93.4%) and from 11 to 20 years old (89.2%), respectively [32, 33]. More worrisome, up to 7.6% of discrepancy between CSP and ELISA results was observed in women pregnant either at the moment or in the preceding 3 years at the time of the respective study [33]. Nevertheless, the same Chagatest v.3.0 (Wiener) failed to detect infection in 29.5% of women PCR-positive at delivery, while the overall CSP rate of false negative was 9.6% [45]. This research enrolled women from Argentina, Honduras, and Mexico, which displayed 97.3, 96.1, and 67.3% of CSP reactivity, respectively [45]. Although the detection in Mexican women was expressively reduced, CSP still outperformed the ELISA assay applied by 39.4% [45]. In a lower-prevalence scenario in Mexico, by taking western blot as confirmatory test, Gamboa-Léon et al. [46] demonstrated similar results between CSP and Chagatest v.3.0 (Wiener), especially in samples collected from umbilical cord.
Both the Trypanosoma Detect (TD) and Chagas Detect Plus (CDP) are based on the multiepitope recombinant protein ITC8.2 [58]. Produced by InBios, their main differences reside in product format and clearance by the U.S. Food and Drugs Administration agency. While TD is presented as a dipstick with application restricted to research [59], the CDP consists of an improved version [60], designed in cassette format—with the gold conjugate maintained in liquid solution—and is marketed for diagnostic use in the USA [60, 61].
TD evaluation in sera samples from Argentina, Ecuador, Mexico, and Venezuela resulted in 82.5, 84.3, 77.5, and 95.0% sensitivity, respectively. On the other hand, specificity was high, with the lower result detected in Ecuador (95.6%) and the greater in both Mexico and Venezuela (100.0%) [62]. In the work by Sánchez-Camargo et al. [56] previously mentioned, it presented an overall sensitivity and specificity of 92.9 and 94.0%, respectively. Similar sensitivity was observed in Bolivian women at delivery (92.7%), however, a higher specificity was shown (99.0%) [63]. In addition, regarding the same study performed with PCR-confirmed infected women with whole blood also collected at delivery in Argentina, Honduras and Mexico, TD testing resulted in more cases of seroreactivity in comparison to ELISA Wiener (v. 3.0) in samples from the latter two countries, while no difference was observed for those from Argentina [45]. Given that the ELISA kit used and the TD share 4 epitopes (peptides 1, 30, 36 and SAPA) between their sets of antigens [58], the TcF and Kmp-11 peptides included in the latter test may be related to the differential detection observed. Nonetheless, CSP still outperformed TD in both Honduras and Argentina [45]. In a survey of immigrants from endemic countries living in Spain that included an electrochemiluminescence immunoassay as reference, a lower sensitivity was obtained (89.6%) with whole blood, while excellent specificity was maintained (100.0%) [64]. Notably, such reference test (Elecsys Chagas, Roche Diagnostics) does not share any antigen with TD.
Aiming to increase sensitivity, the TD was modified, resulting in the CDP assay [60]. Its first performance evaluation was carried out with paired sets of whole blood and sera samples from Bolivian populations encompassing adults (with or without heart disease), pregnant women at delivery and children up to 17 years old. Tests results obtained with each type of sample displayed 90.3% of agreement, with whole blood showing a reduced sensitivity (96.2 vs. 99.3%) and higher specificity (98.8 vs. 96.9%) [60]. Following studies testing whole blood from individuals in different regions of Bolivia reported sensitivity of 92.1–100.0% and specificity of 87.1–99.3%, being the best results obtained in a high seroprevalence area [28, 31, 65]. In Colombia, CDP showed an outstanding performance with whole blood testing as CSP (≥ 99.1% for both parameters) [35]. Interestingly, reported data of Latin American CDP testing in the USA points to difference of performance between plasma and serum, with greater relevance for those from Mexico and Central America (mostly represented by El-Salvador) [34, 66]. More importantly, CDP showed superior sensitivity to samples from these same regions in comparison to three others conventional serological assays (two ELISAs and one IHA), whereas a lower specificity (87.5–92.3%) was observed in the overall analysis [66].
Simple Stick Chagas (SSC) and Simple Chagas WB (SCWB) also comprise rapid tests elaborated in two different formats that are based on the same antigen, a chimeric recombinant protein that englobes the peptide 2, TcD, TcE and SAPA epitopes [67] (Table 1). The former has a dipstick design and can be used with serum, while the latter is displayed as a cassette and can be carried out with either whole blood, plasma, or serum [67]. Studies that include these tests were mainly centered in evaluating their applicability as screening tool of Latin American immigrants and others with epidemiological background of risk living in Spain [67, 68, 69, 70]. Sera testing with SSC showed 92.4–100.0% of sensitivity and 97.9% of specificity, which is reduced to 91.6–92.4% when considering cross-reactivity [67, 68]. As for whole blood testing with SCWB, peripheral samples exhibited a 92.1 and 93.6% of sensitivity and specificity, respectively [67]. Interestingly, capillary samples obtained by finger prick displayed a performance of 86.4 and 95% for the respective parameters [67, 71]. In these works, the onsite results were confirmed latter on by conventional immunoassays carried out with samples collected and stored on filter paper [67, 71]. On the other hand, a 92.5% of sensitivity was observed by Chejade et al. [70] when working with capillary blood and confirmatory assays done with samples frozen until use. Poorer performance was observed by Sánchez-Camargo et al. [56] when testing sera with SCWB, which displayed an overall of sensitivity and specificity of 84.9% and 70.7%, respectively, and a variable response in the quality control evaluation among the laboratories. Authors also called attention to misguiding instructions in the manufacture datasheet, which reflected in the outcome. However, such errors were already corrected [72]. Finally, little to no cross-reactivity was observed for leishmania with SSC and SCWB, however, both assays showed relevant number of false-positives with samples from individuals infected with malaria [67, 68].
The SD Bioline Chagas Ab rapid test relies on the recognition of recombinant antigens H49 and 1F8 (Table 1). Although Sánchez-Camargo et al. [56] reported 90.4 and 94.0% of sensitivity and specificity, respectively, in Colombia, this assay presented a great potential value for diagnosis confirmation when using sera (100.0% specificity), but not as a screening tool [73]. Nonetheless, in Argentinean adult population, sera and whole blood testing presented satisfactory sensitivity (97.6–100%), whereas better specificity was achieved with the latter type of sample (93.8 vs. 97.7%) [36, 37]. WL Check Chagas (WLC) was used in parallel in both studies, which reported similar results [36, 37]. Adding up to other works, WLC is more suitable as a confirmatory test regardless of the type of sample used, especially in Argentina (≥ 98.8% of specificity) [36, 37, 56, 74].
Performance data of Chagas Instantest, OnSite Chagas Ab Combo, and TR Chagas is scarce, beginning with the antigenic formulations (Table 1). Except for the last one, all rapid tests were analyzed by Sánchez-Camargo et al. [56], which—for the best of our knowledge—consists of the only independent source of information for Chagas Instantest. This assay showed sensitivity of 76.6% along with a specificity of 79.0% [56]. A moderate agreement was detected between the obtained and expected results, besides a bad profile and reproducibility on the quality control evaluation [56]. Moreover, authors reported a high frequency of invalid tests and a strong background color, making a clearer interpretation difficult [56]. As for the OnSite Chagas Ab Combo, sera testing presented 90.1–95.5% of sensitivity and 91.0–96.9% of specificity and displayed cross-reactivity with samples from individuals with either leishmaniasis or malaria [56, 68]. At last, a prototype version of TR Chagas was evaluated in a small sampling group formed by sera from Brazilians (n = 32). In this context, densitometry analysis of bands signaling reactivity toward the chimeric recombinant proteins IBMP-8.1 and/or − 8.4 led to excellent results (100.0% for both parameters) [75]. Apart from the small quantity of samples tested, the study also portraits an analysis assessment opposite to reality in point-of-care settings and field study. In addition, there are no surveys done with the final formulation. Finally, we emphasize that TR Chagas is currently only at disposal of Brazilian Ministry of Health.
Many rapid tests were elaborated and evaluated for the detection of T. cruzi infection, however, only a few are commercially available. This is particularly worrisome for those populations with poor performance results, such the Mexicans. Conversely to some authors’ assertion, these data clearly demonstrate that is still a general demand for improvements (notably assays with higher sensitivity) and development of rapid tests with different antigenic preparations to enhance populational cover with different origins. Furthermore, more studies are required to evaluate if the outperformance detected for two rapid tests is restricted to one ELISA kit or if other immunoassays taken as reference may lead to rapid testing underestimated data. Attending these needs will probably trend an increase of rapid tests use in the frontline diagnosis algorithm given its advantages in both clinical and field practices. In sum, validated rapid testing campaigns and seroprevalence studies have a major role in identifying the areas that require more effective public health actions, besides broaden the diagnosis reach, especially regarding those in asymptomatic phase. In clinical practices, its application in points-of-care and emergency services stands out, as in the case of organ transplantation and women at delivery. In view of the higher rate of early CD diagnosis that can be achieved by rapid testing, it may represent a cost-effective approach in the overall socioeconomic gain. We also stress out that the assistance of those patients remotely located would also benefit from an on-site rapid testing that provides a simultaneous detection of disease progression monitoring marker.
1.Chagas C. Nova tripanozomiase humana: estudos sobre a morfolojia e o ciclo evolutivo do Schizotrypanum cruzi n. gen., n. sp., ajente etiolojico de nova entidade morbida do homem. Memórias do Instituto Oswaldo Cruz. 1909;1:60
3.Silva-dos-Santos D, Barreto-de-Albuquerque J, Guerra B, Moreira OC, Berbert LR, Ramos MT, et al. Unraveling Chagas disease transmission through the oral route: Gateways to Trypanosoma cruzi infection and target tissues. PLoS Neglected Tropical Diseases. 2017;11:e0005507. DOI: 10.1371/journal.pntd.0005507
4.Coura JR, Viñas PA, Junqueira AC. Ecoepidemiology, short history and control of Chagas disease in the endemic countries and the new challenge for non-endemic countries. Memórias do Instituto Oswaldo Cruz. 2014;109:856-862. DOI: 10.1590/0074-0276140236
5.Coura JR. The main sceneries of Chagas disease transmission. The vectors, blood and oral transmissions–a comprehensive review. Memórias do Instituto Oswaldo Cruz. 2015;110:277-282. DOI: 10.1590/0074-0276140362
6.Lidani KCF, Andrade FA, Bavia L, Damasceno FS, Beltrame MH, Messias-Reason IJ, et al. Chagas disease: From discovery to a worldwide health problem. Frontiers in Public Health. 2019;7:166. DOI: 10.3389/fpubh.2019.00166
7.Pérez-Molina JA, Molina I. Chagas disease. The Lancet. 2018;391:82-94. DOI: 10.1016/S0140-6736(17)31612-4
8.Lee BY, Bacon KM, Bottazzi ME, Hotez PJ. Global economic burden of Chagas disease: A computational simulation model. The Lancet Infectious Diseases. 2013;13:342-348. DOI: 10.1016/S1473-3099(13)70002-1
9.Abuhab A, Trindade E, Aulicino GB, Fujii S, Bocchi EA, Bacal F. Chagas’ cardiomyopathy: The economic burden of an expensive and neglected disease. International Journal of Cardiology. 2013;168:2375-2380. DOI: 10.1016/j.ijcard.2013.01.262
10.Olivera MJ, Buitrago G. Economic costs of Chagas disease in Colombia in 2017: A social perspective. International Journal of Infectious Diseases. 2020;91:196-201. DOI: 10.1016/j.ijid.2019.11.022
11.Dias JCP. Evolution of Chagas disease screening programs and control programs: Historical perspective. Global Heart. 2015;10:193-202. DOI: 10.1016/j.gheart.2015.06.003
12.DNDi. Chagas disease facts 2022 [Internet]. 2022. Available from: https://dndi.org/diseases/chagas/facts/
13.Iglesias-Rus L, Romay-Barja M, Boquete T, Benito A, Blasco-Hernández T. The role of the first level of health care in the approach to Chagas disease in a non-endemic country. PLoS Neglected Tropical Diseases. 2019;13:e0007937. DOI: 10.1371/journal.pntd.0007937
14.West HM, Milliren CE, Manne-Goehler J, Davis J, Gallegos J, Perez JH, et al. Effect of clinician information sessions on diagnostic testing for Chagas disease. PLoS Neglected Tropical Diseases. 2022;16:e0010524. DOI: 10.1371/journal.pntd.0010524
15.Sales Junior PA, Molina I, Fonseca Murta SM, Sánchez-Montalvá A, Salvador F, Corrêa-Oliveira R, et al. Experimental and clinical treatment of Chagas disease: A review. The American Journal of Tropical Medicine and Hygiene. 2017;97:1289-1303. DOI: 10.4269/ajtmh.16-0761
16.Jackson Y, Wyssa B, Chappuis F. Tolerance to nifurtimox and benznidazole in adult patients with chronic Chagas’ disease. Journal of Antimicrobial Chemotherapy. 2020;75:690-696. DOI: 10.1093/jac/dkz473
17.Pino-Marín A, Medina-Rincón GJ, Gallo-Bernal S, Duran-Crane A, Arango Duque ÁI, Rodríguez MJ, et al. Chagas cardiomyopathy: From Romaña sign to heart failure and sudden cardiac death. Pathogens. 2021;10:505. DOI: 10.3390/pathogens10050505
18.PAHO. Guidelines for the Diagnosis and Treatment of Chagas Disease. Washington, D. C.: PAHO; 2019
19.López-Monteon A, Dumonteil E, Ramos-Ligonio A, López-Monteon A, Dumonteil E, Ramos-Ligonio A. More than a Hundred Years in the Search for an Accurate Diagnosis for Chagas Disease: Current Panorama and Expectations. Rijeka: IntechOpen; 2019. DOI: 10.5772/intechopen.86567
20.Carlier Y, Altcheh J, Angheben A, Freilij H, Luquetti AO, Schijman AG, et al. Congenital Chagas disease: Updated recommendations for prevention, diagnosis, treatment, and follow-up of newborns and siblings, girls, women of childbearing age, and pregnant women. PLoS Neglected Tropical Diseases. 2019;13:e0007694. DOI: 10.1371/journal.pntd.0007694
21.Chippaux J-P, Clavijo ANS, Santalla JA, Postigo JR, Schneider D, Brutus L. Antibody drop in newborns congenitally infected by Trypanosoma cruzi treated with benznidazole. Tropical Medicine & International Health. 2010;15:87-93. DOI: 10.1111/j.1365-3156.2009.02431.x
22.Ruiz-Lancheros E, Chatelain E, Ndao M. Chagas disease treatment efficacy biomarkers: Myths and realities. In: Altcheh JM, Freilij H, editors. Chagas Disease: A Clinical Approach. Cham: Springer International Publishing; 2019. pp. 323-349. DOI: 10.1007/978-3-030-00054-7_16
23.Santos FLN, de Souza WV, da Barros MS, Nakazawa M, Krieger MA, de Gomes YM. Chronic Chagas disease diagnosis: A comparative performance of commercial enzyme immunoassay tests. The American Journal of Tropical Medicine and Hygiene. 2016;94:1034-1039. DOI: 10.4269/ajtmh.15-0820
24.Zingales B, Miles MA, Campbell DA, Tibayrenc M, Macedo AM, Teixeira MMG, et al. The revised Trypanosoma cruzi subspecific nomenclature: Rationale, epidemiological relevance and research applications. Infection, Genetics and Evolution. 2012;12:240-253. DOI: 10.1016/j.meegid.2011.12.009
25.Magalhães LMD, Gollob KJ, Zingales B, Dutra WO. Pathogen diversity, immunity, and the fate of infections: Lessons learned from Trypanosoma cruzi human–host interactions. The Lancet Microbe. 2022;3(9):E711-E722. DOI: 10.1016/S2666-5247(21)00265-2
26.Zingales B. Trypanosoma cruzi genetic diversity: Something new for something known about Chagas disease manifestations, serodiagnosis and drug sensitivity. Acta Tropica. 2018;184:38-52. DOI: 10.1016/j.actatropica.2017.09.017
27.Balouz V, Agüero F, Buscaglia CA. Chagas disease diagnostic applications: Present knowledge and future steps. Advances in Parasitology. 2017;97:1-45. DOI: 10.1016/bs.apar.2016.10.001
28.Lozano D, Rojas L, Méndez S, Casellas A, Sanz S, Ortiz L, et al. Use of rapid diagnostic tests (RDTs) for conclusive diagnosis of chronic Chagas disease – field implementation in the Bolivian Chaco region. PLoS Neglected Tropical Diseases. 2019;13:e0007877. DOI: 10.1371/journal.pntd.0007877
29.Médecins Sans Frontières. International meeting: New diagnostic tests are urgently needed to treat patients with Chagas disease. Revista da Sociedade Brasileira de Medicina Tropical. 2008;41:315-319. DOI: 10.1590/S0037-86822008000300020
30.Anfossi L. Rapid Test - Advances in Design, Format and Diagnostic Applications. Ed.; London, UK: IntechOpen; 2018. DOI: 10.5772/intechopen.70916
31.Egüez KE, Alonso-Padilla J, Terán C, Chipana Z, García W, Torrico F, et al. Rapid diagnostic tests duo as alternative to conventional serological assays for conclusive Chagas disease diagnosis. PLoS Neglected Tropical Diseases. 2017;11:e0005501. DOI: 10.1371/journal.pntd.0005501
32.Roddy P, Goiri J, Flevaud L, Palma PP, Morote S, Lima N, et al. Field evaluation of a rapid immunochromatographic assay for detection of Trypanosoma cruzi infection by use of whole blood. Journal of Clinical Microbiology. 2008;46:2022-2027. DOI: 10.1128/JCM.02303-07
33.Chippaux J-P, Santalla JA, Postigo JR, Romero M, Salas Clavijo NA, Schneider D, et al. Sensitivity and specificity of Chagas Stat-Pak test in Bolivia. Tropical Medicine & International Health. 2009;14:732-735. DOI: 10.1111/j.1365-3156.2009.02288.x
34.Castro-Sesquen YE, Saldaña A, Patino Nava D, Paulette Evans D, Bayangos T, DeToy K, et al. Evaluation of 2 lateral flow rapid tests in the diagnosis of Chagas Disease in the Washington Metropolitan Area. Open Forum Infectious Diseases. 2021;8:ofab096. DOI: 10.1093/ofid/ofab096
35.Suescún-Carrero SH, Salamanca-Cardozo LP, Pinazo M-J, Armadans-Gil L. Sensitivity and specificity of two rapid tests for the diagnosis of infection by Trypanosoma cruzi in a Colombian population. PLoS Neglected Tropical Diseases. 2021;15:e0009483. DOI: 10.1371/journal.pntd.0009483
36.Mendicino D, Colussi C, Moretti E. Simultaneous use of two rapid diagnostic tests for the diagnosis of Chagas disease. Tropical Doctor. 2019;49:23-26. DOI: 10.1177/0049475518813792
37.Lopez-Albizu C, Danesi E, Piorno P, Fernandez M, García Campos F, Scollo K, et al. Rapid diagnostic tests for Trypanosoma cruzi infection: Field evaluation of two registered kits in a region of endemicity and a region of nonendemicity in Argentina. Journal of Clinical Microbiology. 2020;58:e01140-20. DOI: 10.1128/JCM.01140-20
38.Spinicci M, Fumagalli C, Maurizi N, Guglielmi E, Roselli M, Gamboa H, et al. Feasibility of a combined mobile-health electrocardiographic and rapid diagnostic test screening for chagas-related cardiac alterations. Microorganisms. 2021;9:1889. DOI: 10.3390/microorganisms9091889
39.Pinho RT, Waghabi MC, Cardillo F, Mengel J, Antas PR. Scrutinizing the biomarkers for the neglected Chagas disease: How remarkable! Frontiers in Immunology. 2016;7:306. DOI: 10.3389/fimmu.2016.00306
40.Chatelain E. Chagas disease research and development: Is there light at the end of the tunnel? Computational and Structural Biotechnology Journal. 2017;15:98-103. DOI: 10.1016/j.csbj.2016.12.002
41.Requena-Méndez A, López MC, Angheben A, Izquierdo L, Ribeiro I, Pinazo MJ, et al. Evaluating Chagas disease progression and cure through blood-derived biomarkers: A systematic review. Expert Review of Anti-Infective Therapy. 2013;11:957-976. DOI: 10.1586/14787210.2013.824718
42.Caminha MA, de Lorena VMB, de Oliveira JW, Perales J, Carvalho PC, Lima DB, et al. Trypanosoma cruzi immunoproteome: Calpain-like CAP5.5 differentially detected throughout distinct stages of human Chagas disease cardiomyopathy. Journal of Proteomics. 2019;194:179-190. DOI: 10.1016/j.jprot.2018.11.019
43.Rabelo MMN, Larocca TF, Macêdo CT, Torreão JA, de Souza BSF, Vasconcelos JF, et al. Evaluation of Galectin-3 as a Novel Biomarker for Chagas Cardiomyopathy. 2017;136(1):33-39. DOI: 10.1159/000447529
44.Buekens P, Cafferata ML, Alger J, Althabe F, Belizán JM, Bustamante N, et al. Congenital transmission of Trypanosoma cruzi in Argentina, Honduras, and Mexico: An observational prospective study. The American Journal of Tropical Medicine and Hygiene. 2018;98:478-485. DOI: 10.4269/ajtmh.17-0516
45.Truyens C, Dumonteil E, Alger J, Cafferata ML, Ciganda A, Gibbons L, et al. Geographic variations in test reactivity for the serological diagnosis of Trypanosoma cruzi infection. Journal of Clinical Microbiology. 2021;59:e0106221. DOI: 10.1128/JCM.01062-21
46.Gamboa-León R, Gonzalez-Ramirez C, Padilla-Raygoza N, Sosa-Estani S, Caamal-Kantun A, Buekens P, et al. Do commercial serologic tests for Trypanosoma cruzi infection detect Mexican strains in women and newborns? The Journal of Parasitology. 2011;97:338-343. DOI: 10.1645/GE-2545.1
47.Bern C, Verastegui M, Gilman RH, LaFuente C, Galdos-Cardenas G, Calderon M, et al. Congenital Trypanosoma cruzi transmission in Santa Cruz, Bolivia. Clinical Infectious Diseases. 2009;49:1667-1674. DOI: 10.1086/648070
48.Messenger LA, Gilman RH, Verastegui M, Galdos-Cardenas G, Sanchez G, Valencia E, et al. Toward improving early diagnosis of congenital Chagas disease in an endemic setting. Clinical Infectious Diseases. 2017;65:268-275. DOI: 10.1093/cid/cix277
49.Jackson Y, Chatelain E, Mauris A, Holst M, Miao Q , Chappuis F, et al. Serological and parasitological response in chronic Chagas patients 3 years after nifurtimox treatment. BMC Infectious Diseases. 2013;13:85. DOI: 10.1186/1471-2334-13-85
50.Chappuis F, Mauris A, Holst M, Albajar-Vinas P, Jannin J, Luquetti AO, et al. Validation of a rapid immunochromatographic assay for diagnosis of Trypanosoma cruzi infection among Latin-American migrants in Geneva, Switzerland. Journal of Clinical Microbiology. 2010;48:2948-2952. DOI: 10.1128/JCM.00774-10
51.Pane S, Giancola ML, Piselli P, Corpolongo A, Repetto E, Bellagamba R, et al. Serological evaluation for Chagas disease in migrants from Latin American countries resident in Rome, Italy. BMC Infectious Diseases. 2018;18:212. DOI: 10.1186/s12879-018-3118-5
52.Llenas-García J, Hernando A, Fiorante S, Maseda D, Matarranz M, Salto E, et al. Chagas disease screening among HIV-positive Latin American immigrants: An emerging problem. European Journal of Clinical Microbiology & Infectious Diseases. 2012;31:1991-1997. DOI: 10.1007/s10096-011-1531-4
53.Luquetti AO, Ponce C, Ponce E, Esfandiari J, Schijman A, Revollo S, et al. Chagas’ disease diagnosis: A multicentric evaluation of Chagas Stat-Pak, a rapid immunochromatographic assay with recombinant proteins of Trypanosoma cruzi. Diagnostic Microbiology and Infectious Disease. 2003;46:265-271. DOI: 10.1016/s0732-8893(03)00051-8
54.Ponce C, Ponce E, Vinelli E, Montoya A, de Aguilar V, Gonzalez A, et al. Validation of a rapid and reliable test for diagnosis of Chagas’ disease by detection of Trypanosoma cruzi-specific antibodies in blood of donors and patients in Central America. Journal of Clinical Microbiology. 2005;43:5065-5068. DOI: 10.1128/JCM.43.10.5065-5068.2005
55.Gruber A, Zingales B. Trypanosoma cruzi: Characterization of two recombinant antigens with potential application in the diagnosis of Chagas’ disease. Experimental Parasitology. 1993;76:1-12. DOI: 10.1006/expr.1993.1001
56.Sánchez-Camargo CL, Albajar-Viñas P, Wilkins PP, Nieto J, Leiby DA, Paris L, et al. Comparative evaluation of 11 commercialized rapid diagnostic tests for detecting Trypanosoma cruzi antibodies in serum banks in areas of endemicity and nonendemicity. Journal of Clinical Microbiology. 2014;52:2506-2512. DOI: 10.1128/JCM.00144-14
57.Da Costa-Demaurex C, Cárdenas MT, Aparicio H, Bodenmann P, Genton B, D’Acremont V. Screening strategy for Chagas disease in a non-endemic country (Switzerland): A prospective evaluation. Swiss Medical Weekly. 2019;149:w20050. DOI: 10.4414/smw.2019.20050
58.Houghton RL, Stevens YY, Hjerrild K, Guderian J, Okamoto M, Kabir M, et al. Lateral flow immunoassay for diagnosis of Trypanosoma cruzi infection with high correlation to the radioimmunoprecipitation assay. Clinical and Vaccine Immunology. 2009;16:515-520. DOI: 10.1128/CVI.00383-08
59.InBios. Trypanosoma detect rapid test [Internet]. 2023. Available from: https://inbios.com/trypanosoma-detecttm-rapid-test-intl/
60.Shah V, Ferrufino L, Gilman RH, Ramirez M, Saenza E, Malaga E, et al. Field evaluation of the InBios Chagas detect plus rapid test in serum and whole-blood specimens in Bolivia. Clinical and Vaccine Immunology. 2014;21:1645-1649. DOI: 10.1128/CVI.00609-14
61.InBios. Chagas detect Plus rapid test [Internet]. 2023. Available from: https://inbios.com/chagas-detecttm-plus-rapid-test-intl-fda-cleared/
62.Reithinger R, Grijalva MJ, Chiriboga RF, Alarcón de Noya B, Torres JR, Pavia-Ruz N, et al. Rapid detection of Trypanotsoma cruzi in human serum by use of an immunochromatographic dipstick test. Journal of Clinical Microbiology. 2010;48:3003-3007. DOI: 10.1128/JCM.02474-09
63.Brutus L, Schneider D, Postigo J, Romero M, Santalla J, Chippaux JP. Congenital Chagas disease: Diagnostic and clinical aspects in an area without vectorial transmission, Bermejo, Bolivia. Acta Tropica. 2008;106:195-199. DOI: 10.1016/j.actatropica.2008.03.009
64.Silgado A, Gual-Gonzalez L, Sánchez-Montalvá A, Oliveira-Souto I, Goterris L, Serre-Delcor N, et al. Analytical evaluation of dried blood spot and rapid diagnostic test as a new strategy for serological community screening for chronic Chagas disease. Frontiers in Cellular and Infection Microbiology. 2021;11:736630. DOI: 10.3389/fcimb.2021.736630
65.Hopkins T, Gonçalves R, Mamani J, Courtenay O, Bern C. Chagas disease in the Bolivian Chaco: Persistent transmission indicated by childhood seroscreening study. International Journal of Infectious Diseases. 2019;86:175-177. DOI: 10.1016/j.ijid.2019.07.020
66.Whitman JD, Bulman CA, Gunderson EL, Irish AM, Townsend RL, Stramer SL, et al. Chagas disease serological test performance in U.S. blood donor specimens. Journal of Clinical Microbiology. 2019;57:e01217-e01219. DOI: 10.1128/JCM.01217-19
67.Flores-Chavez M, Cruz I, Nieto J, Gárate T, Navarro M, Pérez-Ayala A, et al. Sensitivity and specificity of an operon immunochromatographic test in serum and whole-blood samples for the diagnosis of Trypanosoma cruzi infection in Spain, an area of nonendemicity. Clinical and Vaccine Immunology. 2012;19:1353-1359. DOI: 10.1128/CVI.00227-12
68.Flores-Chávez M, Cruz I, Rodríguez M, Nieto J, Franco E, Gárate T, et al. Comparison of conventional and non-conventional serological tests for the diagnosis of imported Chagas disease in Spain. Enfermedades Infecciosas y Microbiología Clínica. 2010;28:284-293. DOI: 10.1016/j.eimc.2009.07.005
69.Roca C, Pinazo MJ, López-Chejade P, Bayó J, Posada E, López-Solana J, et al. Chagas disease among the Latin American adult population attending in a primary care center in Barcelona, Spain. PLoS Neglected Tropical Diseases. 2011;5:e1135. DOI: 10.1371/journal.pntd.0001135
70.Chejade PL, Saumell CR, Posada E, Pinazo MJ, Brustenga JG, Vynieta MP. Utilidad de un test inmunocromatográfico para el cribado de la enfermedad de Chagas en asistencia primaria. Enfermedades Infecciosas y Microbiología Clínica. 2010;28:169-171
71.Navarro M, Perez-Ayala A, Guionnet A, Pérez-Molina JA, Navaza B, Estévez L, et al. Targeted screening and health education for Chagas disease tailored to at-risk migrants in Spain, 2007 to 2010. Eurosurveillance. 2011;16(38):19973. DOI: 10.2807/ese.16.38.19973-en
72.Operon. Simple Chagas WB [Internet]. 2023. Available from: https://operondx.com/wp-content/uploads/pdf/090509_CHAGASWB_web.pdf
73.Duarte LF, Flórez O, Rincón G, González CI. Comparison of seven diagnostic tests to detect Trypanosoma cruzi infection in patients in chronic phase of Chagas disease. Colombia Médica (Cali). 2014;45:61-66
74.Mendicino D, Stafuza M, Colussi C, del Barco M, Streiger M, Moretti E. Diagnostic reliability of an immunochromatographic test for Chagas disease screening at a primary health care centre in a rural endemic area. Memórias do Instituto Oswaldo Cruz. 2014;109:984-988. DOI: 10.1590/0074-0276140153
75.Silva ED, Silva ÂAO, Santos EF, Leony LM, Freitas NEM, Daltro RT, et al. Development of a new lateral flow assay based on IBMP-8.1 and IBMP-8.4 chimeric antigens to diagnose Chagas disease. BioMed Research International. 2020;2020:1803515. DOI: 10.1155/2020/1803515
Written By
Marcelle Almeida Caminha, Ana Luiza Barbosa Godart Cavalcante and Rubem Figueiredo Sadok Menna-Barreto
Submitted: 06 January 2023Reviewed: 07 January 2023Published: 10 February 2023
 Open access peer-reviewed chapter
Open access peer-reviewed chapter