Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
To purchase hard copies of this book, please contact the representative in India:
CBS Publishers & Distributors Pvt. Ltd.
www.cbspd.com
|
customercare@cbspd.com
Worldwide, the cumulative annual disabilities and deaths due to neglected tropical diseases (NTDs) are in the millions, with most cases found in the low-income countries. The World Health Organization (WHO) has proposed a road map to eliminate NTDs by the year 2030. Core interventions being implemented to achieve this target are vaccinations, chemotherapeutic treatments, vector control, and practicing hygiene. Whereas multiple successes have been registered so far, inadequacies or the complete absence of diagnostics for some of the diseases being targeted, are however hampering ongoing eradication campaigns. Current diagnostics for NTDs are costly, require sophisticated gadgets, depend on electricity, are time consuming and labor intensive, have low detection/discriminatory power, or require trained personnel for operation. For these reasons, the use of such diagnostics is limited to only well-equipped laboratories, often inaccessible to the poor who are the most affected by the NTDs. To increase accessibility to diagnostics by those who need it the most, Rapid Diagnostic Tests (RDTs) are being developed by translating existing diagnostic technologies, or by invention of new technologies. Here, we reviewed conventional diagnostics for NTDs as well as their RDT translated formats, and explored nanobodies (Nbs) as alternative reagents for the development of the RDTs.
Laboratory of Cellular and Molecular Immunology, Vrije Universiteit Brussel, Brussels, Belgium
Department of Biomedical Biochemistry and Microbiology, Ghent University, Ghent, Belgium
Magdalena Radwanska
Laboratory for Biomedical Research, Ghent University Global Campus, Incheon, South Korea
Department of Biomedical Molecular Biology, Ghent University, Ghent, Belgium
Stefan Magez
Laboratory of Cellular and Molecular Immunology, Vrije Universiteit Brussel, Brussels, Belgium
Department of Biomedical Biochemistry and Microbiology, Ghent University, Ghent, Belgium
Laboratory for Biomedical Research, Ghent University Global Campus, Incheon, South Korea
Steven Odongo*
Laboratory for Biomedical Research, Ghent University Global Campus, Incheon, South Korea
Department of Biotechnical and Diagnostic Sciences, College of Veterinary Medicine, Animal Resources and Biosecurity, Makerere University, Kampala, Uganda
Center for Biosecurity and Global Health, College of Veterinary Medicine, Animal Resources and Biosecurity, Makerere University, Kampala, Uganda
*Address all correspondence to: steven.odongo@ghent.ac.kr;, steven.odongo@mak.ac.ug
1. Introduction
According to data from the WHO, communicable diseases ranked among the top 10 causes of deaths in the low-income countries [1]. In contrast, high-income countries control these diseases through vigorous implementation of prevention and treatment campaigns, reinforced with timely diagnosis. Recently, the WHO has established a road map for eradication of the neglected tropical diseases NTDs, by the year 2030 [2]. Neglected tropical diseases are designated as “neglected” partly because they are frequently overlooked by health systems [2]. They include buruli ulcers, chagas disease, dengue, and chikungunya, dracunculiasis, echinococcosis, foodborne trematodiases (FBT), Human African trypanosomiasis (HAT), leishmaniasis, leprosy, lymphatic filariasis, mycetoma/chromoblastomycosis and other deep mycoses, onchocerciasis, rabies, scabies and other ectoparasitoses, schistosomiasis, soil-transmitted helminthiases (STH), snakebite envenoming, taeniasis and cysticercosis, trachoma, and yaws. A foreseen set-back to the WHO’s 2030 road map to elimination of NTDs, is the inadequate deployment of diagnostics for case finding, treatment follow-up, and surveillance. It should be noted that even COVID-19 test is not widely accessible, which has left the population in a precarious state.
The conventional methods for diagnosis of NTDs can be classified into eight groups: (i) nucleic acid amplification tests (NAATs), methods for detection of whole or part of a pathogen genome; (ii) immunoassays, methods for detection of a pathogen antigenic (Ag) component, or a pathogen-induced host antibodies (Abs); (iii) microscopy, methods for detection of a pathogen, or its pathological effect(s); (iv) culture, methods for isolating pathogen from clinical specimen using either in vitro or in vivo culture systems followed by either direct or indirect detection with other tests, or detection based on growth characteristics; (v) imaging, non-invasive visual methods for revealing a pathogen or gross deformities caused by a pathogen that are located in situ; (vi) chemical profiling, methods for analyzing chemical components and/or characteristics of a pathogen; (vii) entomological identification, methods for tracking a pathogen in its arthropod vector sentinel for human infections; and (viii) clinical manifestation, methods for detection of a pathogen by drawing inference from the accompanying pathognomonic behavioral changes and/or gross lesions. Each of these methods of diagnosis is further expounded in Section 2.1. Except for the clinical sign-based diagnosis, methods that rely on laboratory testing are not widely applied in impoverished communities due to high costs, absence of well-equipped laboratories, absence of electricity, lack of professionally trained machine operators and maintenance personnel, and complexities surrounding interpretation of assay results. To overcome the listed challenges, modifications of the conventional laboratory-based diagnostic tools and methods are needed. Such modifications include (i) miniaturization, (ii) elimination of multiple assay steps, (iii) multiplexing, and (iv) visual interpretation applications. Nowadays there are simplified diagnostic technologies with enhanced speed, popularly known as RDTs. Given that RDTs have led to effective management of malaria, tuberculosis, and HIV/AIDS in low-income countries, their integration in the NTD control panels is anticipated to yield a positive outcome.
While several authors have reported development of RDT prototypes for NTDs, only a few are so far being marketed [3]. One of the reasons for this is the technical limitations encountered by relatively low sensitivity and specificity. While antigen detecting diagnostics are specific with respect to their capacity to report active infection [4, 5], they usually have low sensitivity, especially when the pathogen load is low or immune complexes between target antigens and infection induced host antibodies are formed [6]. To tackle this, there is ongoing exploratory research involving the use of Nbs [7]. The invention of nanobody technology dates to the year 1993, when Hamers-Casterman et al. discovered heavy-chain only IgG antibodies (HCAbs) in the serum of Camelus dromedarius [8]. In the recent past, the application of Nb technology for the development of antigen detection RDTs for infectious diseases have tremendously increased [9, 10, 11], exploiting unique epitopes recognition potential of Nbs [12, 13]. Given that Nb epitopes can be located in ‘pockets’, such as invariant enzyme active sites, their use can ameliorate false negative test resulting from variant natures of surface exposed epitopes [14]. A second advantage of Nb technology is that due to the recombinant production of these molecules, they can easily be tailored [7]. These characteristics allow for Nbs to be used for the development of accessible, sensitive, and specific antigen RDTs.
In this chapter, we reviewed available diagnostics for NTDs focusing on conventional as well as commercialized RDTs and the ongoing efforts to develop rapid antigen RDT using Nbs.
2. Conventional methods for diagnosis of neglected tropical diseases
A plethora of diagnostic platforms are applied singly, or in combination, to achieve diagnosis of NTDs. In principle, each of the conventional diagnostic platforms is multi-spectrum based, being used for the detection of more than one NTD. There are circumstances where modifications were introduced to conventional diagnostics, yielding versions with higher sensitivities and specificities. While these newer versions may have better performance, some have become too complex, rendering them ineffective for field use. As earlier mentioned, most of these diagnostics do not operate as an entity but complement each other. In this section, therefore, the different classical diagnostic methods used either for screening or confirming NTDs, including their modified versions, are reviewed.
2.1 Nucleic acid amplification tests
Nearly 90% of the NTDs are diagnosed by nucleic acid amplification test (NAAT) methods (Table 1). The first-generation NAAT technology, the polymerase chain reaction (PCR), was invented in 1983 by Kary Mullis [15]. At present, PCR technology is widely applied in diagnosis and other fields of biosciences. The technology is used for diagnosis of NTDs including Buruli ulcers [16], Dengue [17], Chikungunya [18], HAT [19], leishmaniasis [20], Dracunculiasis [21], deep mycoses [22], onchocerciasis [23], rabies [24], STH [25], and yaws [26] among others. PCR lends itself as a sensitive pathogen detection tool owing to its ability to amplify a single copy of genome to billions of copies. The diagnostic scope of the original PCR was broadened by introducing several modifications. Popular versions of PCR used for diagnosis of NTDs are the reverse transcriptase (RT)-PCR, and real-time RT-PCR. Because it can copy RNA to DNA followed by amplification, RT-PCR is used for diagnosis of the two RNA viral NTDs, i.e., chikungunya [18] and dengue [17]. Real-time RT-PCR, for quantification of nucleic acid load, is used for diagnosis of viral, bacterial, parasitic as well as fungal NTDs. There are groups of pathogens that cannot be discriminated base on NAAT alone, because they have the same amplicon product size. A number of tricks were introduced to solved this challenge, and two examples are given here. Firstly, a second set of nested primers, in a technique call nested PCR, has been introduced to amplify the inner region of the first amplicon product, resulting in variant product sizes. Nested PCR is used for typing the agents for buruli ulcers [16], dengue [17], echinococcosis [27], and HAT [28]. Secondly, a restriction enzyme system, in a technique call restriction fragment length polymorphism (RFLP), was introduced to cut amplified PCR products into fragments producing distinct pathogen-specific restriction profiles. PCR-RFLP technique is used for typing the causative agents of trypanosomiasis [29], leishmaniasis [30], lymphatic filariasis [31] and STH [32].
Conventional Diagnostic Methods
Diagnostic Formats
Neglected topical diseases
Buruli ulcers
Chagas disease
Dengue
Chikungunya
Dracunculiasis
Echinococcosis
FBT
HAT
Leishmaniasis
Leprosy
Lymphatic filariasis
Deep mycoses
Onchocerciasis
Rabies
Ectoparasitoses
Schistosomiasis
STH
Snakebite envenoming
Taeniasis/cysticercosis
Trachoma
Yaws
NAAT
cPCR
+
+
+
+
+
+
+
+
+
+
+
+
+
RT-PCR
+
nPCR
+
+
+
+
rRT-PCR
+
+
+
+
+
+
+
+
+
+
PCR-RFLP
+
+
+
+
+
Immunoassay
ELISA
+
+
+
+
+
+
+
+
+
+
+
+
+
+
+
IFA
+
+
+
+
+
+
VNT
+
+
Hypersensitvity test
+
+
+
+
MBA
+
WB
+
+
+
(Hem)Agglutination Assay
+
+
+
+
+
HI
+
CFT
+
+
Microscopy
Unstained smears
+
+
+
+
+
+
+
+
+
+
+
+
Stained smears
+
+
+
+
+
+
Histopathology
+
+
+
+
+
+
+
Culture
In vitro
+
+
+
+
+
In vivo
+
+
+
Imagine
Radiography
+
+
+
Ultrasonography
+
+
+
+
+
MRI
+
+
CT scan
+
+
Chemical profile analyses
MLEE
+
MALDI-TOF (MS)
+
+
Blood clot test
+
Xenodiagnoses
Animals
+
Insects
+
+
Clinical signs
Gross lesions
+
+
+
+
+
+
+
+
+
+
+
+
+
+
Behavioral
+
+
Others
Echocardiogram
+
Electrocardiogram
+
Table 1.
Summary of conventional test platforms used for diagnosis of the neglected tropical diseases.
(1) Symbols: positive-sign (+), diagnostic method is frequently applied for diagnosis of a given NTD; empty box (), scare or no reports showing application of the diagnostic method for diagnosis of that NTD.
(2) Abbreviations: FBT, foodborne trematodiases; HAT, Human African Trypanosomiasis; STH, Soil-transmitted helminths; NAAT, nucleic acid amplification test; PCR, polymerase chain reaction; cPCR, conventional PCR; RT-PCR, Reverse transcriptase PCR; nPCR, Nested PCR; rRT-PCR, real-time reverse transcriptase PCR; PCR-RFLP, PCR restriction fragment length polymorphism; IFA, Immunofluorescence assay; VNT, virus neutralization test; MBA, Multiplex bead assay; WB, Western blot; HI, Hemagglutination inhibition assay; CFT, Complement fixation test; MRI, Magnetic resonance imaging; MLEE, Multilocus Enzyme Electrophoresis; and MALDI-TOF (MS), Matrix assisted laser desorption/ionization time of flight mass spectrometry.
The NAAT technology revolutionized diagnosis of infectious diseases including NTDs by being robust, high throughput, none labor intensive, sensitive, and specific. Furthermore, NAAT technology allows for multi-pathogen detection through multiplexing [26, 33]. However, with all the desirable qualities, routine mass use of NAAT for diagnosis of NTDs is hampered by costs, its complexity, the requirement for trained operators, and the requirement for expensive equipment as well as a constant supply of electricity. Also, NAAT is sensitive to contaminants, leading to an increased risk for false negative or positive results. Recently introduced among the NAAT-based test panels, is the loop mediated isothermal amplification (LAMP) assay [34]. The LAMP assay has brought NAAT technology closer to its ideal status suitable for routine diagnosis of NTDs in a primary healthcare setting [35, 36]. The LAMP assay is rapid, and it requires less expensive reaction step incubation equipment making it adaptable to field conditions. However, in its current form LAMP is not yet fully furnished to service primary healthcare. At times, the assay still requires sample processing, incurring additional costs and posing contamination risk. The interpretation of LAMP result is subjective, the technique is not completely equipment free, and it still require invasive method of sample collection. Generally, NAAT technology does not yet meet the WHO requirements for an ideal test, which should be Affordable, Sensitive, Specific, User-friendly, Equipment-free and Deliverable to those who need it (ASSURED) [37]. Therefore, further investment is required to produce an ideal NAAT, which is superior to the current version of LAMP assay. Nevertheless, in its current form the LAMP assay has tremendously aided field diagnosis of some NTDs.
2.2 Immunoassays
Immunoassays are well-embedded in the diagnosis of NTDs. Undoubtedly, immunoassays form a large proportion of commercially available NTD diagnostics, and those undergoing development. According the literature reviewed, about 90% of the NTDs are diagnose by immunoassay. Versions of immunoassays exist for laboratory as well as field diagnosis of NTDs. Among others, dengue, chikungunya, echinococcosis, FBT, HAT, leishmaniasis, onchocerciasis, yaws, STH, schistosomiasis, and rabies diagnosis all rely on immunoassays. There are traditional as well as contemporary formats in the NTD diagnostic panels. The most popular classical immunoassay format used for diagnosis of NTDs is the enzyme-linked immunosorbent assay (ELISA). The ELISA technique was published in early 1970’s by Van Weemen and Schuurs [38]. This versatile technique is very instrumental in the diagnosis of several NTDs as shown in Table 1. As noted previously, ELISA is among those “dual-purpose” immunoassay methods in use either for antibody or antigen detection. Antibody detection ELISAs for diagnosis of NTDs are many but only a few examples are listed here; the Hemagen ELISA for chagas disease [39], MAC-ELISA for dengue [40], Em2-ELISA for echinococcosis [41], the anti-Mycobacterium leprae phenolic glycolipid I (PGL-I) IgM ELISA for leprosy [42], the Ov-16 ELISA for onchocerciasis [43], and the FAST-ELISA for schistosomiasis [44]. Unlike antibody detecting ELISA, fewer antigen detecting ELISAs for diagnosis of NTDs exist. An example of antigen detecting ELISA is the CA-ELISA for diagnosis of FBT [45] and Og4C3 ELISA for lymphatic filariasis [46]. Besides ELISA, other popular formats of immunoassay for diagnosis of NTDs are (in)direct immunofluorescence, virus neutralization assays, delayed-type hypersensitivity reaction skin tests, multiplex bead assay, western blot, in(direct) agglutination assays, hemagglutination inhibition assays, and complement fixation assays. Respective NTDs diagnosed by each of these immunoassay formats are listed in Table 1.
Like NAAT, classical immunoassay formats do suffer from limitations. In addition to some of the challenges shared with the NAAT, classical immunoassays are low- throughput, labor intensive, and often have lower sensitivity and specificity values. Efforts are underway to translate laboratory-based immunoassay formats to a field applicable point-of-care test (POC), which are suitable for primary health care settings where most of the NTD cases are frequently reported. The commonly encountered POC test frameworks are immunochromatographic test strips, and agglutination assays. The POC test immunoassays have largely solved challenges related to portability and speed. However, the sensitivity and specificity remain often suboptimal. Antibody detection tests, which form the bigger proportion of the current POC immunoassays for NTDs, commonly give false positive test results either due to cross-reactivity [47] or persistence of antibodies after the clearance of infections [48]. False negative test resulting from low pathogen load, sequestration of target in immune complex, and loss of antigen integrity following poor sample handling, characterize most antigen detecting POC tests. All these limitations demand that alternative options are sought to improve the specificity as well as sensitivity of the available immunoassay formats. Hence, this justifies the reason for Nb technology exploration in this area.
2.3 Microscopy
Microscopy is perhaps the most ancient diagnostic platform for the NTDs. The technology was developed by Antony van Leeuwenhoek, a Dutch microbiologist and microscopist, who lived in the fifteenth century in Delft, Holland [49]. For the different models and types of microscopes used for pathogen detection, standard microbiology text books can be consulted such as the Microbial Life [49], Brock Biology of Microorganism [50], and Jawetz, Melnick & Adelberg’s Medical Microbiology [51]. Essentially, diagnosis of all the NTDs, except snakebite envenoming, rely on direct or indirect microscopy. Originally the technique relies either on direct visualization of a magnified whole dead (or living) pathogen [52, 53, 54], a pathogen product like eggs [55], or a pathogen induced lesions [56]. When used for detection of viral NTDs, microscopy reveals infection-induced cellular changes known as cytopathic effects, such as rabies viral-induced inclusion bodies (Negri bodies) in the cytoplasm of neurons [57]. Dengue fever virus and chikungunya viruses are also detected based on characteristic inclusion bodies, which appear in the in vitro cell cultures.
While microscopy remain a definitive test for some NTDs, poor detection limit often affects its usability. To improve performance, refinements of the methods as well as the tool were made. The modifications introduced to increase resolution power of microscopy for diagnosis of NTDs include the introduction of specimen staining with dyes (e.g., giemsa staining), or by chemical-labeled Abs (immunofluorescence). Thanks to the improvements the acid-fast Mycobacterium ulcerans, the agent of buruli ulcer, can now be easily detected upon specimen staining with Ziehl-Neelsen dye, and the rabies virus antigen in brain tissue section can be revealed upon immunofluorescent-labelling with the anti-rabies protein Abs. In other circumstances, the NTD reagent is amplified by growing in an in vivo (animal model) or in vitro (artificial media or cell line) culture system to a high density prior to detection by microscopy. For example, Trypanosoma and Leishmania are sometimes cultured in mouse model prior to detection by microscopy. Similar, M. ulcerans, M. leprae, chikungunya, and actinomycetoma are sometimes isolated in an in vitro culture system prior to detection. While much as the improvements cited enhance the diagnostic power of microscopy, these refined techniques still require electricity, and are time-consuming and labor intensive. In addition, interpretation of test result is often subjective with low discriminatory power. Integration of pathogen culture with microscopy also exposes assay operators to high-risk pathogens, and there is a possibility of introducing environmental contaminants, which could jeopardize assay results. Finally, advanced microscopes are unsuitable for routine clinical practice, and are limited to research purposes, as they are expensive and complex. Hence, some of the limitations of microscopy cited herein prevent its routine use in a primary healthcare.
2.4 Isolation of pathogen in a culture system
A definitive diagnosis for some the pathogens causing NTDs relies on their amplification in a culture system(s) to attain disease symptoms, or high pathogen density to ease detection [30]. In this instance, interpretation of the result is dependent on phenotypic characteristics including development of pathological changes in an in vitro or in vivo culture system. The cultured organisms may also be subjected to subsidiary confirmatory tests including biochemical assays, microscopy, NAAT, immunoassays among others. The diagnosis of M. leprae, for example, is based on culturing the organism, which usually takes up to 14 days. Thereafter, colonial morphologic characteristics are established, and other standard staining techniques, immunoassays and NAAT are implemented for characterization the agent. Culture as a diagnostic test is a long procedure given that it requires multiple steps. Where primary microbiological test results are general, secondary tests are employed to confirm the diagnosis. Pathogen isolation is not only time consuming but it is also prone to errors, which can occur at any of the assay steps. Often expensive materials are required from culturing the organisms until getting the test results subsequently increasing the overall costs of testing. Maintaining sterile conditions for pathogen isolation is huge challenge in the low-income countries. Furthermore, not all the pathogens can be isolated in an artificial in vitro culture system, and ethical issues impede the use of laboratory animals in diagnosis. Although microbiological culture system cannot be avoided altogether, a shift to RDTs would offer solution to some of these challenges.
2.5 Imaging
Imaging is a non-invasive technique for scanning the body of a pathogen or tissue deformities. The technique can be used for diagnosis of several diseases [58]. As tool for diagnosis of NTDs, imaging techniques are commonly applied for diagnosis of dracunculiasis [59], echinococcosis/hydatid cyst [60], FBT [61], onchocerciasis [62], and Taeniasis/neurocysticercosis [63]. The tool is also used for indirect diagnosis of chagas disease by indirectly inferring from the destruction of the myocardium [39]. A collection of imaging technique applied in the diagnosis of NTDs are radiography (employs ionizing radiations like x-rays and gamma rays), ultrasonography, magnetic resonance imaging (MRI), and computerized tomography (CT) scan. Radiography is used for the diagnosis of chagas disease, dracunculiasis, and deep mycoses; ultrasonography for echinococcosis, FBT, deep mycoses, onchocerciasis, and cysticercosis; and both MRI and CT scan for echinococcosis and cysticercosis. Although they may not perfectly fit here, it is worth mentioning that electrocardiogram and echocardiogram are valuable biosensing tools used for diagnosis of chagas disease. Imaging is a preferred technique because it is non-invasive. Routine application of imaging techniques in low resource settings is however impracticable. The most advanced imaging technique requires well-equipped laboratory employing highly qualified personnel for the operation as well as the interpretation of the test result. Additionally, continuous exposure to radioactive materials, which is a fundamental component of radiography, poses health-risks. With the availability of hand-held ultrasonography, the use of imaging is no longer restricted to a laboratory setting. However, the high cost of ultrasonographic equipment impedes it wide scale deployment in a primary healthcare. Miniaturizing the technique while eliminating the cost and complexity would popularize its use in remote settings such as the pastoral communities, where the cysticercosis is highly prevalent.
2.6 Chemical profile analysis
The analysis of the levels of toxins or metabolic by-products deliberately, accidentally, or unintentionally elaborated by foreign organisms into a patient or in the culture system can lead to a diagnosis. On the other hand, aberrant functions of the host’s physiological biochemicals such as enzymes and hormones, are sometimes measured during disease investigation process. A few situations standout to exemplify the chemical profiling analysis in disease diagnosis. For instance, the diagnosis of snake bites envenoming relies on coagulopathic tests, which is a 20-minute whole blood clotting test (WBCT20) POC test. There is also a thin layer chromatography tests for detection of M. ulcerans, the causative agent of buruli ulcers, which relies on testing for the elaborated mycolactone toxin [64]. Chemical assay tests are less specific, rendering it impossible to target treatment to a specific species or strains causing the disease where species-specific treatment is required. Some of the NTDs are detected based on their signature proteome profiles. Examples in this category are the Multilocus Enzyme Electrophoresis (MLEE) [65], which is used for typing leishmania, and the matrix assisted laser desorption ionization-time of flight-mass spectrometry (MALDI-TOF MS) for leishmania [30] and HAT [66]. The MALDI-TOF and MLEE analyses are not useful for routine diagnosis but rather for research purpose. Another form of chemical profiling analysis is the culture and sensitivity assays, which involve response to chemical drug treatment. This is not a more classical routine diagnosis method but rather applicable in a situation where a pathogen’s response to drug treatment is being investigated.
2.7 Entomological identification
The identification of pathogens in the arthropod vectors have been used to infer their presence in human hosts [67], wherein intermediate hosts are used as sentinels to monitor occurrence of the agents in a geographic location. Entomological survey involves catching a vector and testing with conventional molecular tool(s) to find whether they are infested with the pathogen under investigation. When vectors score positive, then deductions can be made about possible infection of humans living in that given locality. The entomological identification of agents has been applied to survey vector transmitted NTDs such as trypanosomiasis, onchocerciasis, leishmania, and dengue, in vectors including the tsetse fly, simulium fly, sandfly, and mosquitoes, respectively. The method is non-invasive for humans; hence, it reduces exposure of humans to pain associated with sample collection during disease investigation. However, the technique is only applicable to vector borne NTDs. It should also be noted that the absence of a pathogen capable of both human-to-human transmission as well as vector-to-human transmissions in a surveyed vector(s) may falsely show its absence of the in a human population if there are asymptomatic human carriers in that geographical region. Besides, where there are no vectors, it is impossible to declare absence of such infection, without conducting thorough screening of potential human reservoir. To alleviate the situation, rapid screening of potential human reservoir should be implemented concurrently. Another variant of the entomological disease investigation is performed in a confined setting where vectors are fed on a disease suspect(s), which normally present with low pathogen density with the hope of amplifying it to a detectable level in the fed vector. This method is like the isolation of pathogen by culturing techniques already reviewed in Section 2.4. Among other limitations, this method is costly considering that well-equipped infrastructure is required for maintaining vector colony for such purpose. The test result is not instant. Also, sterile vectors are fed on animal hosts, not humans, meaning that the method can only monitor vector transmitted zoonotic NTDs with known and easily accessible animal host.
2.8 Clinical manifestation
The first-line of disease investigation, in principle, is based on the detection and interpretation of symptoms to arrive at (tentative) diagnoses prior to involvement of other disease investigation methods. It is sufficed to say that clinicians in the primary healthcare often rely on disease symptoms to arrive at a diagnosis. Successful application of clinical signs to arrive at a precise diagnosis requires experience, and only works well for those diseases with cardinal signs. It should also be noted that disease detection based on symptom is usually conducted in the late stages of infection when severe damage has already occurred, making it impossible to achieve timely case management. Also, it cannot detect organisms involved in mixed infections, and latent infections often escape detection. Additionally, diseases presenting with similar signs are often impossible to discriminate. For this reason, except for a few diseases, diagnosis of NDTs based on clinical is often unreliable. Nevertheless, with all its imperfections, reliance on clinical signs is solely employed by the primary healthcare workers to diagnose tungiasis, scabies, rabies, and dracunculiasis.
3. Rapid diagnostic tests for neglected tropical diseases
Rapid diagnostic tests are characterized by their ability to give instant test result within a time span of 5 minutes to 2 hours. Such tests are essentially intended for a preliminary screening for example in resource-limited countries, where there is no easy access to healthcare [68]. Exceptionally, like during COVID-19 pandemic, they have even been used on a large scale in resource-rich countries, when the healthcare system risks of being overrun by a massive disease outbreak situation. The RDTs should meet ASSURED criteria. The commercial RDTs formats for diagnosis tests for NTDs are lateral flow immunochromatographic assays (LFIAs), agglutination-based assays, dot immunogold filtration assays (DIGFA) and LAMP. While the first three are immunoassay-based tests, and the fourth belongs is a molecular-based test. Nonetheless, many other formats of tests exist, both for the NTDs and other groups of diseases. Of recent there are also multiplex RDTs capable of detecting more than single infectious agent.
Due to the effort invested in the development of novel treatments as well as novel diagnostic tests, ten countries have eliminated at least one RDT, resulting in 500 million fewer people needing to be treated than in 2010 [69]. While progress toward the development of RTDs has been made, few tests have reached the stage of commercialization. To-date, buruli ulcer, dracunculiasis, FBT, leprosy, scabies, schistosomiasis, STH, taeniasis, cysticercosis, snakebite envenoming, and yaws still do not have reliable commercial RDTs. Although new RDTs are being developed in direct collaboration with industry [70], there remains a clear lack of interest and funding for RDTs development. Generally, less than 5% of all funding available for NTD research and development is earmarked for diagnostic development projects [69].
3.1 Formats of rapid diagnostic tests for neglected tropical diseases
Despite the limited funding available for the improvement of NTD diagnostics, the WHO’s 2021–2030 road map to prevent, control, eliminate, or eradicate all 20 NTDs is enabling the development of new RDTs. At present, two formats of commercial RDTs exist; the immunoassay-based tests, and NAAT-based tests. Besides, there are hybrid tests having both immunoassay and NAAT features undergoing development [71].
3.1.1 Immunoassay-based tests
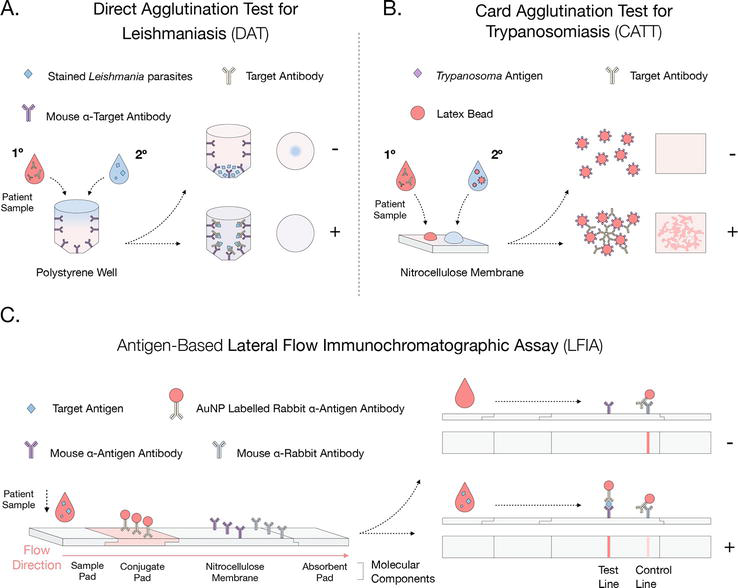
Agglutination-based tests, belonging to the immunoassay-based tests, have played a key role in the surveillance and control of leishmania and HAT in the field. Two commercial kits are commercially available through the Institute of Tropical Medicine Antwerp (Belgium) and the Academic Medical Centre Amsterdam (Netherlands) are the Card Agglutination Test for Trypanosomiasis (CATT) [72] and the Direct Agglutination Test (DAT) for leishmaniasis [73], respectively. CATT is a standard initial screening and diagnostic test for T. brucei gambiense HAT in the field [74, 75]. It is commercialized as a small paper sheet, for detection of parasite-induced host Abs in blood, plasma, or serum [72]. To perform the test, a sample is dispensed into the test paper, where the T. b. gambiense LiTat 1.3 and LiTat 1.5 VSG Ags are lyophilized attached to latex beads (Figure 1). When Abs recognizing these Ags are present in the test sample, they bind to multiple Ags resulting in visible agglutination [74, 76]. Similarly, DAT also detects the presence of Abs through agglutination; however, the commercial format differs. DAT is performed on 96-well plates with tip-ended wells, in which freeze-dried anti-human Abs are placed. The blood, plasma or serum sample is then applied. Right after, stained parasites are added. If Abs are present in the sample, layers of immune complex involving anti-human Ab, human anti-leishmania Ab and the leishmania Ag is formed, generating a homogenous color in the well surface [77]. In a negative test, the parasites will sink to the bottom of the wells, generating a distinct blue dot [77]. Despite their huge contribution toward the control of HAT and Leishmaniasis, CATT and DAT tests have some common drawbacks, which makes them less ideal for continued use in the field [73, 78]. Firstly, there is a problem of production robustness, resulting in the tests being mainly manufactured at research institutes. This limits the total available supplies, and requiring a cold chain to avoid spoilage [73, 75, 78]. Furthermore, both tests are not equipment free, and require electricity as well as well-trained technicians [73, 79]. In addition, the DAT has a relatively high price per test (costing about €8), and is time-consuming, requiring an incubation time of about 18 hours [73, 80]. Regarding the intrinsic properties of these tests, the sensitivity and specificity values are respectively 87–98% and 98% for CAAT, and 93–97% and 94–99% for DAT (Table 2). However, these values are clearly susceptible to factors such as low Ab titers, the presence of Abs from past infections, the cross-reactivity between different parasite species, or the hook effect where an excess of Abs impedes agglutination [115]. Given the low prevalence of both diseases, even a small change in specificity would result in a drastic drop in Positive Predictive Value (PPV) [2, 116]. In view of the afore-mentioned, CATT and DAT assays do not meet the ASSURED criteria, nor the recently implemented Real-time connectivity (R), and Ease (E) of specimen collection and environmental friendliness (RE)ASSURED criteria for POC diagnostic testing [117].
Figure 1.
Overview of the format and operating mechanism of the main commercially available immunoassay-based RDTs for the diagnosis of NTDs. A: Direct agglutination test for leishmaniasis (DAT), in which the patient sample is displayed in a polystyrene well, containing specific Abs against the target antibody. Then, stained leishmania parasites are added. In case of the presence of the target Abs, a sandwich will be formed between the capturing Abs and the stained parasites, resulting in a cloudy coloration of the well. Otherwise, a negative result will imply the parasites to sink into the well and form a clear dot. B: Card agglutination test for trypanosomiasis (CATT), in which the patient samples, and a solution with latex beads labeled with Trypanosoma antigens are displayed in a nitrocellulose membrane. In case of the presence of the target Abs, an agglutination phenomenon will be formed between the target Abs and the bead with the Ags. Otherwise, a negative result will imply the beads to be dispersed along the membrane without agglutination, resulting in a cloudy coloration of the paper. C: Antigen-based lateral flow immunochromatographic assay (LFIA), in which the patient sample is displayed in a nitrocellulose membrane, containing detecting AuNP labeled antibodies against the Ag, capturing Abs against the Ag and Abs against the detecting Abs. The sample will flow by capillary forces through the strip where, in case of the presence of the target Abs, a sandwich will be formed between the capturing and labeled detecting Abs, resulting in colored lines on the test and control lines. Otherwise, a negative result will imply the formation of a single-colored line at the control line.
A sample of commercially available rapid diagnostic tests being used for diagnosis of the neglected tropical diseases.
Point of Care applicability of RDTs has clearly been improved by the development of LFIAs for NTDs. This test format is commercially available for HAT [72], chagas disease [81, 82, 83, 84, 85], onchocerciasis [86], Trachoma [3, 87, 88], Dengue [3, 89, 90], Chikungunya [91, 92], lymphatic filariasis [3, 93, 94], leishmaniasis [95, 96, 97, 98, 99, 100, 101, 102], Echinococcosis [103, 104, 105, 106, 107], rabies [108, 109, 110], and schistosomiasis [111] (Table 2). These tests are based on the detection of target analytes contained in a liquid sample (i.e., body fluids such as serum, plasma, or whole blood). The analytes are displaced through capillary forces along a paper (nitrocellulose) strip, where molecules that detect the presence of the analytes are attached [118]. According to the target analyte, there are two types of LFIAs in existence: Ab-based (detecting Abs) and Ag-based (detecting Ags). LFIAs detecting Abs, upon a positive sample, will result in a sandwich formation between an Ag, adsorbed to the membrane, the target Ab, and a labeled-detection Ab. Despite the high sensitivity values usually achieved, specificity is usually limited, particularly due to the non-specific binding of non-targeted Abs with the Ags (especially when these are native antigens coming from a lysate) [119, 120]. Indeed, these tests are also inefficient when it comes to differentiating between current or past infections, as well as when performing post-treatment follow-ups [121]. In contrast, LFIAs detecting Ags, upon a positive sample, will result in a sandwich formation between the Ab, adsorbed to the membrane, the target Ag, and a labeled-detection Ab. This type of test is, in contrast to Ab-tests, able to differentiate between past and current infections, and can also be used as a test-of-cure, offering drastic improvements in the diagnosis performance of LFIAs. Moreover, their specificity values are normally much better than Ab-based tests; therefore, showing also better PPV. However, they generally have a lower sensitivity, which greatly depends on the amount of Ags in the sample [5]. This situation occurs when: (i) Ag concentration is lower than the test’s analytical sensitivity or LOD (e.g., due to the masking effect produced by host anti-Ag Abs) [122]; or (ii) Ag concentration is higher than the test’s concentration of detecting Abs (referred to as post-zone phenomenon of the Hook effect) [123]. Finally, it should be noted that in any LFIA, regardless of type, it is imperative to improve the method of sample extraction to make it minimally or non-invasive, thus further enhancing its applicability in the POC.
The last commercially available immunoassay-based test for RDTs (Echinococcosis) is DIGFA [103, 112]. It has a similar format to the Ab-based LFIA. However, the sandwich between the antigens on the membrane, the antibodies in the sample and the detection antibody occurs in a much similar way to an ELISA, where each reagent is added in steps, with washings in-between [112]. Although it is a test that provides a rapid result with high sensitivity and specificity values, its drawbacks remain the same as those of all the Ab-based tests mentioned above.
3.1.2 Nucleic acid-based tests
As a solution to further improve the intrinsic properties of agglutination tests, LFIA, and DIGFA (particularly for very low prevalence scenarios), the LAMP, belonging to molecular-based tests, can be used. Currently, there are commercially available LAMP assays for HAT [113], and for leishmaniasis [114]. This is a similar technique to PCR, however, enhanced for POC implementation due to the isothermal nature of the reaction (i.e., single constant temperature at around 58–65°C), only requiring a simple, low-cost heat source (e.g., a portable heat block or a water bath) [124]. Moreover, the reaction requires only 30–60 minutes to obtain a visible signal, halving that of a conventional PCR, generally without leading to non-specific amplifications [125]. Unlike PCR, LAMP amplification employs four specific primers, which can be extended to 6 by adding 2 loop primers, further reducing the reaction time [126]. In addition, it allows DNA amplification in clinical specimens (e.g., whole blood) without inhibition of their enzymes [125, 127]. LAMP readout is possible by fully quantitative techniques such as reaction tube turbidity due to magnesium pyrophosphate precipitate or color variations with pH-sensitive dyes, or by more qualitative and user-friendly methods such as LFIAs [126, 128, 129, 130]. Despite these features, LAMP reactions still have drawbacks. For instance, since it is a very sensitive technique, it is susceptible to even slight sample contaminations [127].
4. Research and development of rapid antigen tests for neglected tropical diseases
4.1 Translation of conventional immunoassays to rapid antigen tests
Conventional tests for NTDs will not be relegated completely from the disease investigation agendas, given that it is nearly impossible to develop an ideal diagnostic for each of the NTDs. Indeed, new diagnostic technologies shall only complement the existing classical assays. The current focus, therefore, should majorly aim at addressing the key limitations of the conventional tests. As such, contemporary rapid antigen detecting technologies should mainly address pitfalls bedeviling classical tests including costs, speed, portability, sensitivity, specificity, and ease of result interpretation. In recent years, conventional immunoassays have been modified to alter and/or reduce the numbers of steps, reagents, and equipment. This reduction has ultimately reduced costs, time, and risk of error often associated with multiple steps, and use of multiple reagents and equipment. Where multiple steps are involved, there are high chances of the target analyte leaching out at every step of the assays, consequently reducing the sensitivity. Non-standardized steps may also lead to high background readings, especially in ELISA when washing steps are performed sub-optimally due to time constraint. Hence, current designs of rapid Ag test are meant to minimize the factors affecting classical Ag detection test formats. Indeed, new rapid Ag tests do not require sample processing steps, use low sample volumes and some are even based on non-invasively sample collection, like saliva usage. There are also efforts being undertaken to introduce methodological modification that improve the sensitivity of RDTs. One example of this is the improvement of sensitivity of rapid Ag tests, by combining monoclonal Ag capturing antibodies with and detecting Nb reagents. Here, access and development of high affinity Nbs to a specific target antigen is important. Hence, utmost care should be exercised when screening Nb libraries, to ensure that only potent Nb molecule are selected. The most crucial activity at screening stage is to validate selected Nb molecules for interaction with their target (s) including binding affinity [131]; and, to ensure that there is no cross-reactivity with non-target antigens [4]. Authoritative protocols on Nb generation can be found elsewhere [132].
4.2 Re-designing rapid antigen diagnostic test to enhance capability using nanobodies, nanomaterials, and other technologies
Since 2003, RDTs for use in the POC had to follow the WHO-designated ASSURED criteria. However, in 2019 this term was modified to REASSURED [117]. To meet the new criteria, many improvements were introduced. Collectively, we have biosensors LFIAs, which are devices that detect the presence of an analyte present in a sample by means of a biological capture sensor (e.g., an Ab or Ag), a signal transducer (e.g., a chemically labeled-Ab), and a signal detector (e.g., absorbance or fluorescence detector) [133]. When improving, for example, the current LFIAs available for the detection of NTDs, further optimization and enhancement can be made to each of the different parts constituting the biosensor. In the following sections, some of the improvements that are undergoing investigation for future enhancement of the RDTs are discussed.
4.2.1 Nanobodies
Conventional Gamma (γ) immunoglobulin (IgG), have two heavy (H) and two light (L) chain polypeptides, inter-linked by inter-chain disulfide bonds [134]. Each of these chains consists of a constant domain (CH1, CH2, and CH3 for the heavy chain; and CL for the light chain), and a variable domain (VH for the heavy chain, and VL for the light chain) [135]. Generally, proteolytic cleavage of immunoglobulins (Igs) by papain and pepsin yields three and two distinct functional fragments, respectively. Products originating from digestion of Igs by papain are two fragment antigen binding (Fab) regions, which contain both complete L chains and the CH1 and VH of the H chains; and single fragment crystallizable (Fc). On the other hand, pepsin digestion of Igs products is one F(ab’)2 and may small pieces of the Fc fragment, the largest designated pFc’ fragment. The Fab fragments are responsible for the binding to the target Ags by their three hyper-variable regions (CDRs), located in the VH and VL domains [136]. The Fc region (whose name refers to its easy crystallization properties), which contains paired CH2 and CH3 domains of the heavy chains is responsible for the interaction with effector molecules and cells [137].
Overall, the use of Abs as detection molecules for the development of RDTs is widely known. However, the Ab technology still has certain limitations, which have led to the exploration of novel alternatives. As it was already introduced in Section 1, the Camelidae family including C. dromedarius, C. bactrianus, Lama glama, Lama guanicoe, Vicugna pacos, and V. vicugna possess ‘heavy chain-only’ IgGs (HCAbs) besides convention antibodies. The cloned and expressed variable region of such HCAb is referred to as a VHH, or ‘nanobody’ (Nb—due to its nanometer size) [135, 138]. Nbs possess certain desirable characteristics, preferred for many applications, including the development of RDTs [5, 139]. One of these characteristics consists of their small size, being ten times smaller (∼15 kDa) than conventional Abs (∼150 kDa), and around 3 time smaller than a Fab (∼50 kDa) [137, 140]. Despite their small size, Nbs possess the full antigen-binding potential of the parent HCAb molecule and are thereby considered to be the smallest naturally occurring intact Fabs [141]. The specific detection of antigen epitopes by Nbs primarily relies on the use of their CDR3, which unlike human Abs (with average 12 amino acids long) is commonly extended (with average 18 amino acids long) [141]. As a result, Nbs have a protruding loop that can bind to buried epitopes in the cavities (e.g., hydrophobic pockets in catalytic sites), generally inaccessible by regular Abs [142, 143]. The unique epitope preference by the Nbs and Abs partly addresses the low sensitivity problem of the Ag-based tests attributed to the immune complex masking effects [141].
Another major feature of Nbs lies in their lack of a VL region. This has resulted in natural substitutions among several of their residues, leading to a general decrease in hydrophobicity (excluding most lama spp. VHH). These amino acid substitutions are (VH-VHH): Leu12Ser, Val42Phe/Tyr, Gly49Glu, Leu50Arg/Cys, and Trp52Gly [144]. As a result, Nbs are generally: (i) more stable (resistant to high temperature-pH variations, proteolytic degradation, exposure to chemical denaturants, etc., without negatively affecting the Ag binding capacity); (ii) undergo more efficient refolding after a denaturing process, and (iii) are more soluble than conventional Abs [141]. In addition, Nbs are also easier to produce than Abs, lacking post-translational modifications and achieving higher production yields in diverse organisms (e.g., E. coli, Saccharomyces cerevisiae or Pichia pastoris) [141, 144, 145].
Together, these properties above have made the use of Nbs as an alternative reagent for Abs possible in many applications, including therapeutics. Examples of such applications that have been commercialized are Caplacizumab, for Thrombotic thrombocytopenic purpura [146], and Ozoralizumab, for Rheumatoid arthritis [147]. Nbs for diagnostics include NeutrobodyPlex (under development), for COVID-19 (SARS-CoV-2) [148], and Nano-IC, for acute gastroenteritis (Human Norovirus) [9]. In this regard, nanobodies have proved to be a great advantage, broadening the range of potential targets, and improving the intrinsic properties of previous tests (e.g., sensitivity of Ag-based tests). In line with diagnostics, Nb technology is being explored as a tool for development of tests for diseases caused by the Trypanosoma sp. There is ongoing development of antigen detection diagnostics including a specific Nb-based ELISA and LFIA for T. congolense infections [4, 5], a specific Nb-based ELISA for T. evansi, T. brucei, and T. equiperdum infections [149], and a Nb-based ELISA for T. evansi, T. brucei, T. congolense, T. vivax infections [150]. In addition, a Nb-based ELISA has been developed for the diagnosis of Plasmodium falciparum infections [151], as well as for the diagnosis of Taenia solium infections [152]. The relevance of Nb detection technology for the generation of new and improved RDTs for NTDs is therefore clear.
4.2.2 Nanomaterials
Since their development, LFIAs have been the preferred format for RDTs at the POC and this has been clearly confirmed after their extended use during COVID-19 pandemic. While the basic components of LFIAs technology were developed many decades ago, the integration of new nanomaterials has further improved the intrinsic properties of these tests in the recent years. These include sensitivity, specificity, PPV) and NPV. Even so, sensitivity remains the characteristic where most effort has been put into improvement, as it is often impaired in LFIAs due to low analyte concentrations in the sample [153]. Nanomaterial-based sensitivity enhancements mainly focus on: (i) improving signal transducers, or (ii) improving signal amplification.
The most used signal transducers are gold nanoparticles (AuNPs) and dyed beads, usually linked to capture antibodies. They present a low molar absorptivity, which implies that in cases of low target analyte concentration, insufficient accumulation of these nanoparticles will occur to generate a measurable optical signal [154]. Consequently, the LFIAs’ sensitivity is significantly diminished. In response, research into new signal transducers has led to improvements in the LOD of the test, thereby improving sensitivity. Some of these new nanomaterials base their readability, in the same way as AuNPs or dyed beads, on their absorptivity. However, they generally have higher absorbances and more available binding sites for the detecting Abs, thus generating an overall greater contrast with the nitrocellulose strip, thereby improving the assay readout. Among these new materials are carbon nanoparticles and multi-walled carbon nanotubes, which have respectively yielded 3.8 times lower LODs and 10 times lower LODs compared to standard AuNP-based LFIAs [155, 156]. Other signal transducer improvements are based on the use of materials that allow a fluorescence-based readout. Thus, switching from a bright background readout (absorbance) to a dark background, enabling detection of minimum light levels [154]. Among these new materials are Quantum dots (QDs) and fluorescent nanodiamonds, which have respectively yielded a 78 times higher sensitivity and 105 times higher sensitivity compared to standard AuNP-based LFIAs [157, 158]. However, it is vital for fluorescence-based readout to choose a suitable strip material (e.g., nitrocellulose, or glass). If the strip materials produce auto-fluorescence at the same/near wavelength as the chosen fluorophore molecule, this will result in an intrinsic background that will impair the test performance [159].
Despite the remarkable improvements in the sensitivity of fluorescence-based readout signal transducers, the need for extra instrumentation to perform the test poses a clear drawback to its applicability in the POC [154]. A direct example of the use of these new signal transducers for the diagnosis of NTDs can be found in Dutta et al., where a test for the detection of Dengue Virus DNA with a femtomolar LOD is described [160].
Above-mentioned signal transducers are widely used in LFIAs. However, other types of diagnostic tests such as electroanalytical diagnostic methods are also under research. These typically use transistors acting as signal transducers, upon which a biological capture sensor is functionalized. When a certain voltage is applied across the transistor, if the target analyte binds to the sensor, an electrical signal is produced. This can be directly monitored by an electronic device connected to the detector. There are different approaches for such tests, which can use Abs (or even Nbs) as biological sensors, or even enzymes (e.g., Cas9) [161, 162]. Generally, these tests possess a sensitivity directly comparable to that of NAAT-based tests. However, these tests are still under development, and require further improvements to be able to directly compete with LFIAs, which are more intuitive, cost-effective, and are built with environmentally friendly materials. A few examples of this technology can be found for NTDs, for example, targeting Dengue infections [163, 164].
The enhancement of signal amplification also allows further LFIA sensitivity improvement. Several methods are available, but the most common approach is the AuNP enlargement. This involves the enhancement of the contrast produced between the AuNP color and the strip background color by bonding AuNPs to other molecules, for example silver (Ag), or platinum (Pt) metals. In this context, Ag staining occurs when this metal is released from nanofibers (contained in the strip itself) and reduced around the AuNPs. This results in 10 times more sensitivity than using AuNPs alone, and without compromising the POC properties of the LFIA [165]. The use of Pt as a sensitivity enhancement works slightly different. This metal is directly coated to AuNPs when manufacturing the strip, and has a unique feature that makes it ideal for this type of use: it has horseradish peroxidase-like catalytic activity, i.e., in the presence of 3,3′,5,5′-Tetramethylbenzidine substrate, it leads to its oxidation and generating a bluish color. This allows for up to a 100-fold increase in sensitivity, as compared to when using AuNPs alone [166].
4.2.3 Other new molecular technologies
Alternative approaches being used to improve RDTs include the use of biological capture sensors (e.g., aptamers), or the use of new strategies based on signal amplification (e.g., CRISPR-Cas). Notwithstanding the widespread use of biological capture sensors such as Abs/Nbs or Ags, it is also possible to use aptamers, nucleic acid sequences (i.e., short-stranded DNA or RNA) or peptides, which are capable of specifically binding to analytes of interest thanks to their three-dimensional conformations. Their selection and performance are comparable to that of common Abs, obtaining a robust and specific binding [167]. In addition, the low molecular weight, chemical composition, and selection process make these sensors a reliable tool with low non-specific interactions, whether with proteins, nucleic acids, or other targets [154]. Furthermore, they are more stable at high temperature conditions than Abs, thus being ideal for use in a POC setting [168, 169]. However, these tests are not yet fully optimized, meaning they are not yet cost-effective for commercialization [170].
The use of the CRISPR-Cas recognition systems as a signal amplification strategy for RDTS has been reported to increase both sensitivity and specificity, a critical requirement where disease prevalence is low, such as in HAT or leishmaniasis [116, 154]. The technology is based on the use of the RNA-guided DNA endonuclease Cas, which can be programmed to target a specific DNA/RNA sequence using a synthetic guide-RNA fragment.
Some Cas family members (e.g., Cas12, Cas13, and Cas14) remain active after cleavage of target DNAs, and execute an additional non-specific, collateral, or trans-cleavage activity [171]. By adding to the test sample ssDNA/RNA molecular probes containing a reporter, in case of the presence of the target DNA/RNA, Cas protein will start with this non-specific cleavage of surrounding probes, releasing the reporter molecules, easily detected with a LFIA [172]. In addition, this method can be coupled to RDTs such as LAMP, resulting in considerable improvements in sensitivity and specificity [173], at a reduced price per test (as low as $0.61 USD) [174, 175]. Although not yet commercially available, mainly due to the lack of pre-amplification optimization prior to the use of this technology, there are already examples of reported use for diagnosis of NTDs such as for HAT [71], Zika and Dengue [157].
There is hope of overcoming the burdens of NTDs and other diseases, currently contributing to the development challenges facing low-income countries. Effective ways to contain these diseases are early detection, case management, periodic surveillance, and implementation of preventive measures including regular sensitization of the masses through community awareness campaigns. In the recent past the WHO has drawn attention for the need to combat the scourge of NTDs. Although there are positive gains following the ongoing WHO campaign, it is important to realize that some of the NTDs cannot be diagnose effectively due to the lack of proper diagnostics. Therefore, new technologies should be developed to improve or complement the existing diagnostic platforms. Preferably, these new diagnostic inventions should be REASSURED. With all its desirable attributes, Nb technology is a new technology not yet maximally explored in the fields of NTD diagnostics. Except for prototypes—developed for only a few NTDs including cysticercosis and animal trypanosomiasis—there are no commercial Nb-based RDTs for NTDs. There is need to deeply investigate the potentials of Nbs for diagnosis of NTDs currently left unattended. As a first step to this approach, researchers should dedicate efforts to finding suitable biomarker(s) for each of the NTDs where applicable. Thereafter, Nbs should be generated against each of these target profiles followed by assay development and proper validation. For this to succeed, there is urgent need for cooperation among relevant stakeholders including the WHO, development agencies including non-governmental organizations, commercial companies, industries, research scientists, clinicians, policy makers, economists, research and/or education institutions, as well as community leaders.
A 2 × 2 table showing how to analyze diagnostic test parameters. The information presented in the table originated from [176].
New diagnostic test result
Reference standard true diagnosis
Total
Positive
Negative
Positive
a (True positive)
b (False negative)
a + b
Negative
c (False positive)
d (True negative)
c + d
Total
(a + c)
(b + d)
(N)
(i) Diagnostic Accuracy:[(a + d)/N]; (ii) Sensitivity: the test’s ability to obtain a positive test when the target condition is really present, or the true positive rate [a/(a + c)]; (iii) Specificity: the test’s ability to obtain a negative test when the condition is really absent, or the true negative rate [d/(b + d)]; (iv) False positive rate (1 - specificity): the probability of an incorrect positive test in those who do not have the target condition [b/(b + d)]; (v) False negative rate (1 - sensitivity): the probability of obtaining an incorrect negative test in patients who do have the target disorder [c/(a + c)]; (vi) Positive Predictive Value (PPV): the proportion of the true positive in those samples that scored positive by the test [a/(a + b)]; (vii) Negative Predictive Value (NPV): the proportion of true negative in those sample that scored negative by test [d/(c + d)]; (viii) Prevalence: the number of cases of a condition existing in each population at any one time [(a + c)/N]; (ix) Positive likelihood ratio: tell us how many times more likely a positive test will be seen in those with the disorder than in those without the disorder [Sensitivity/1 – Specificity]; and (x) Negative likelihood ratio: tell us how many times more likely a negative test will be seen in those with the disorder than in those without the disorder [1 - Sensitivity/Specificity].
References
1.WHO. The Top 10 Causes of Death [Internet]. 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death. [Accessed: November 28, 2022]
2.Ntuli MM, editors. Ending the neglect to attain the Sustainable Development Goals: A Road Map for Neglected Tropical Diseases 2021–2030. World Health Organization; 2020. 196 p. ISBN: 978 92 4 001035 2. Available from: https://www.who.int/publications/i/item/9789240010352. [Accessed: December 11, 2022]
3.Bioline. Rapid Diagnostic Test Infectious Diseases, Bioline TM Product Catalogue [Internet]. 2022. Available from: https://content.veeabb.com/1d09429b-8373-419f-8f1a-d28f9586863a/87c102d8-0a11-45f2-925f-c3ffae2d2345/87c102d8-0a11-45f2-925f-c3ffae2d2345_source__v.pdf [Accessed: November 28, 2022]
4.Odongo S et al. An anti-proteome nanobody library approach yields a specific immunoassay for Trypanosoma congolense diagnosis targeting glycosomal aldolase. PLoS Neglected Tropical Diseases. 2016;10(2):e0004420. DOI: 10.1371/journal.pntd.0004420
5.Torres JE et al. Development of a nanobody-based lateral flow assay to detect active Trypanosoma congolense infections. Scientific Reports. 2018;8(1):9019. DOI: 10.1038/s41598-018-26732-7
6.Büscher P. Diagnosis of African trypanosomiasis. In: Magez S, Radwanska M, editors. Trypanosomes and Trypanosomiasis. Wien: Springer; 2014. pp. 189-216. DOI: 10.1007/978-3-7091-1556-5_8
7.Muyldermans S et al. Camelid immunoglobulins and nanobody technology. Veterinary Immunology and Immunopathology. 2009;128(1–3):178-183. DOI: 10.1016/j.vetimm.2008.10.299
8.Hamers-Casterman C et al. Naturally occurring antibodies devoid of light chains. Nature. 1993;363(6428):446-448. DOI: 10.1038/363446a0
9.Doerflinger SY et al. Development of a nanobody-based lateral flow immunoassay for detection of human norovirus. mSphere. 2016;1(5):e00219-16. DOI: 10.1128/mSphere.00219-16
10.Zhang C et al. Development of nanobody-based flow-through dot ELISA and lateral-flow immunoassay for rapid detection of 3-phenoxybenzoic acid. Analytical Methods. 2021;13(14):1757-1765. DOI: 10.1039/d1ay00129a
11.Salvador JP, Vasylieva N, Gonzalez-Garcia I, Jin M, Caster R, Siegel JB, et al. Nanobody-based lateral flow immunoassay for the rapid detection of aflatoxin B1 in almond milk. ACS Food Science & Technology. 2022;2(8):1276-1282. DOI: 10.1021/acsfoodscitech.2c00118
12.Desmyter A et al. Crystal structure of a camel single-domain VH antibody fragment in complex with lysozyme. Nature Structural Biology. 1996;3(9):803-811. DOI: 10.1038/nsb0996-803
13.De Genst E et al. Molecular basis for the preferential cleft recognition by dromedary heavy-chain antibodies. Proceedings of the National Academy of Sciences of the United States of America. 2006;103(12):4586-4591. DOI: 10.1073/pnas.0505379103
14.Crowther JR. Methods in Molecular Biology: The ELISA Guidebook. 2nd ed. New York: Springer Science; 2009. p. 413. DOI: 10.1385/1592590497
15.Mullis KB. The unusual origin of the polymerase chain reaction. Scientific American. 1990;262(4):56-61, 64-5. DOI: 10.1038/scientificamerican0490-56
16.Stinear T et al. Identification and characterization of IS2404 and IS2606: Two distinct repeated sequences for detection of Mycobacterium ulcerans by PCR. Journal of Clinical Microbiology. 1999;37(4):1018-1023. DOI: 10.1128/JCM.37.4.1018-1023.1999
17.Lanciotti RS et al. Rapid detection and typing of dengue viruses from clinical samples by using reverse transcriptase-polymerase chain reaction. Journal of Clinical Microbiology. 1992;30(3):545-551. DOI: 10.1128/jcm.30.3.545-551.1992
18.Van Den Bossche D, Cnops L, Meersman K, Domingo C, Van Gompel A, Van Esbroeck M. Chikungunya virus and West Nile virus infections imported into Belgium, 2007-2012. Epidemiology and Infection. 2015;143(10):2227-2236. DOI: 10.1017/S0950268814000685
19.Radwanska M et al. The serum resistance-associated gene as a diagnostic tool for the detection of Trypanosoma brucei rhodesiense. The American Journal of Tropical Medicine and Hygiene. 2002;67(6):684-690. DOI: 10.4269/ajtmh.2002.67.684
20.Hijjawi N et al. Molecular diagnosis and identification of leishmania species in Jordan from saved dry samples. BioMed Research International. 2016;2016:6871739. DOI: 10.1155/2016/6871739
21.Coker SM et al. Development and validation of a quantitative PCR for the detection of Guinea worm (Dracunculus medinensis). PLoS Neglected Tropical Diseases. 2022;16(10):e0010830. DOI: 10.1371/journal.pntd.0010830
22.Rodrigues AM, de Hoog GS, de Camargo ZP. Molecular diagnosis of pathogenic Sporothrix species. PLoS Neglected Tropical Diseases. 2015;9(12):e0004190. DOI: 10.1371/journal.pntd.0004190
23.Biamonte MA et al. Onchocerciasis: Target product profiles of in vitro diagnostics to support onchocerciasis elimination mapping and mass drug administration stopping decisions. PLoS Neglected Tropical Diseases. 2022;16(8):e0010682. DOI: 10.1371/journal.pntd.0010682
24.Mani RS, Anand AM, Madhusudana SN. Human rabies in India: An audit from a rabies diagnostic laboratory. Tropical Medicine & International Health. 2016;21(4):556-563. DOI: 10.1111/tmi.12669
25.Ngcamphalala PI, Lamb J, Mukaratirwa S. Molecular identification of hookworm isolates from stray dogs, humans and selected wildlife from South Africa. Journal of Helminthology. 2019;94:e39. DOI: 10.1017/S0022149X19000130
26.Chi KH et al. Molecular differentiation of Treponema pallidum subspecies in skin ulceration clinically suspected as yaws in Vanuatu using real-time multiplex PCR and serological methods. The American Journal of Tropical Medicine and Hygiene. 2015;92(1):134-138. DOI: 10.4269/ajtmh.14-0459
27.Dinkel A et al. Detection of Echinococcus multilocularis in the definitive host: Coprodiagnosis by PCR as an alternative to necropsy. Journal of Clinical Microbiology. 1998;36(7):1871-1876. DOI: 10.1128/JCM.36.7.1871-1876.1998
28.Cox A et al. A PCR based assay for detection and differentiation of African trypanosome species in blood. Experimental Parasitology. 2005;111(1):24-29. DOI: 10.1016/j.exppara.2005.03.014
29.Delespaux V et al. PCR-RFLP using Ssu-rDNA amplification: Applicability for the diagnosis of mixed infections with different trypanosome species in cattle. Veterinary Parasitology. 2003;117(3):185-193. DOI: 10.1016/j.vetpar.2003.08.004
30.Reimao JQ et al. Laboratory diagnosis of cutaneous and visceral leishmaniasis: Current and future methods. Microorganisms. 2020;8(11):1632. DOI: 10.3390/microorganisms8111632
31.Thanomsub BW et al. Differential diagnosis of human lymphatic filariasis using PCR-RFLP. Molecular and Cellular Probes. 2000;14(1):41-46. DOI: 10.1006/mcpr.1999.0283
32.Mulinge E et al. Molecular identification of zoonotic hookworms in dogs from four counties of Kenya. Journal of Helminthology. 2019;94:e43. DOI: 10.1017/S0022149X1900018X
33.Fyfe JA et al. Development and application of two multiplex real-time PCR assays for the detection of Mycobacterium ulcerans in clinical and environmental samples. Applied and Environmental Microbiology. 2007;73(15):4733-4740. DOI: 10.1128/AEM.02971-06
34.Notomi T et al. Loop-mediated isothermal amplification of DNA. Nucleic Acids Research. 2000;28(12):E63. DOI: 10.1093/nar/28.12.e63
35.Kuboki N et al. Loop-mediated isothermal amplification for detection of African trypanosomes. Journal of Clinical Microbiology. 2003;41(12):5517-5524. DOI: 10.1128/JCM.41.12.5517-5524.2003
36.Chen X et al. Nanoparticle-based lateral flow biosensor integrated with loop-mediated isothermal amplification for rapid and visual identification of chlamydia trachomatis for point-of-care use. Frontiers in Microbiology. 2022;13:914620. DOI: 10.3389/fmicb.2022.914620
37.Mabey D et al. Diagnostics for the developing world. Nature Reviews. Microbiology. 2004;2(3):231-240. DOI: 10.1038/nrmicro841
39.Forsyth CJ et al. Recommendations for screening and diagnosis of chagas disease in the United States. The Journal of Infectious Diseases. 2022;225(9):1601-1610. DOI: 10.1093/infdis/jiab513
40.CDC. Centers for Disease Control and Prevention: Serologic Tests for Dengue Virus. 2019. Available from: https://www.cdc.gov/dengue/healthcare-providers/testing/serologic-tests.html
41.Gottstein B et al. Serological (Em2-ELISA) and parasitological examinations of fox populations for Echinococcus multilocularis infections. Zentralblatt für Veterinärmedizin. Reihe B. 1991;38(3):161-168. DOI: 10.1111/j.1439-0450.1991.tb00858.x
42.Romero-Montoya M, Beltran-Alzate JC, Cardona-Castro N. Evaluation and monitoring of mycobacterium leprae transmission in household contacts of patients with Hansen’s disease in Colombia. PLoS Neglected Tropical Diseases. 2017;11(1):e0005325. DOI: 10.1371/journal.pntd.0005325
43.Shintouo CM et al. Tandem use of OvMANE1 and Ov-16 ELISA tests increases the sensitivity for the diagnosis of human onchocerciasis. Life (Basel). 2021;11(12). DOI: 10.3390/life11121284
44.Hancock K, Tsang VC. Development and optimization of the FAST-ELISA for detecting antibodies to Schistosoma mansoni. Journal of Immunological Methods. 1986;92(2):167-176. DOI: 10.1016/0022-1759(86)90162-6
45.Shalaby SI et al. Detection of coproantigens by Sandwich ELISA in rabbits experimentally infected with Fasciola gigantica. Iranian Journal of Parasitology. 2014;9(3):374-381
46.Wattal S et al. Evaluation of Og4C3 antigen ELISA as a tool for detection of bancroftian filariasis under lymphatic filariasis elimination programme. The Journal of Communicable Diseases. 2007;39(2):75-84
47.Wanji S et al. Further evidence of the cross-reactivity of the Binax NOW(R) filariasis ICT cards to non-Wuchereria bancrofti filariae: Experimental studies with Loa Loa and Onchocerca ochengi. Parasites & Vectors. 2016;9:267. DOI: 10.1186/s13071-016-1556-8
48.Espino AM, Millan JC, Finlay CM. Detection of antibodies and circulating excretory-secretory antigens for assessing cure in patients with fascioliasis. Transactions of the Royal Society of Tropical Medicine and Hygiene. 1992;86(6):649. DOI: 10.1016/0035-9203(92)90174-b
50.Madigan MT, Bender KS, Buckley DH, Brock TD, Sattley MW, Stahl DA. Biology of Microorganisms. 15th ed. Pearson; 2018. p. 1058. ISBN 1292235101, 9781292235103
51.Riedel S, Morse S, Mietzner T, Miller S. Jawetz Melnick & Adelbergs Medical Microbiology. 28th ed. McGraw Hill/Medical; 2019. ISBN10: 1260012026 | ISBN13: 9781260012026
52.Roepstorff A et al. Helminth parasites in pigs: New challenges in pig production and current research highlights. Veterinary Parasitology. 2011;180(1–2):72-81. DOI: 10.1016/j.vetpar.2011.05.029
53.WHO/Expert Committee on the Control of human African trypanosomiasis editors. Control and surveillance of human African trypanosomiasis: WHO TRS N°984: Report of a meeting of the WHO Expert Committee. 2013. p. 247. ISBN: 978 92 4 120984 7. Available from: https://www.who.int/publications/i/item/WHO-TRS-984 [Accessed: January 01, 2023]
54.Hay R et al. The diagnosis of fungal neglected tropical diseases (fungal NTDs) and the role of investigation and laboratory tests: An expert consensus report. Tropical Medicine and Infectious Disease. 2019;4(4):122. DOI: 10.3390/ tropicalmed4040122
55.Speich B et al. Comparative cost assessment of the Kato-Katz and FLOTAC techniques for soil-transmitted helminth diagnosis in epidemiological surveys. Parasites & Vectors. 2010;3:71. DOI: 10.1186/1756-3305-3-71
56.Dofitas BL et al. Yaws in the Philippines: First reported cases since the 1970s. Infectious Diseases of Poverty. 2020;9(1):1. DOI: 10.1186/s40249-019-0617-6
58.Rodriguez Carnero P et al. Unexpected hosts: Imaging parasitic diseases. Insights Into Imaging. 2017;8(1):101-125. DOI: 10.1007/s13244-016-0525-2
59.Barry SK, Schucany WG. Dracunculiasis of the breast: Radiological manifestations of a rare disease. Journal of Radiology Case Reports. 2012;6(11):29-33. DOI: 10.3941/jrcr.v6i11.1137
60.Caglar YS et al. Spinal hydatid cyst disease : Challenging surgery—An institutional experience. Journal of Korean Neurosurgical Association. 2019;62(2):209-216. DOI: 10.3340/jkns.2017.0245
61.Brown JD. Human fascioliasis (liver fluke disease) in Hawai’i: Case report and review of human fascioliasis acquired in the United States. Hawaiʻi Journal of Health & Social Welfare. 2021;80(9):212-217
62.Mand S et al. Frequent detection of worm movements in onchocercal nodules by ultrasonography. Filaria Journal. 2005;4(1):1. DOI: 10.1186/1475-2883-4-1
63.Garcia HH, Gonzalez AE, Gilman RH. Taenia solium cysticercosis and its impact in neurological disease. Clinical Microbiology Reviews. 2020;33(3):e00085-19. DOI: 10.1128/CMR.00085-19
64.Converse PJ et al. Accelerated detection of mycolactone production and response to antibiotic treatment in a mouse model of mycobacterium ulcerans disease. PLoS Neglected Tropical Diseases. 2014;8(1):e2618. DOI: 10.1371/journal.pntd.0002618
65.Van der Auwera G, Dujardin JC. Species typing in dermal leishmaniasis. Clinical Microbiology Reviews. 2015;28(2):265-294. DOI: 10.1128/CMR.00104-14
66.Papadopoulos MC et al. A novel and accurate diagnostic test for human African trypanosomiasis. Lancet. 2004;363(9418):1358-1363. DOI: 10.1016/S0140-6736(04)16046-7
67.Cameron MM, Ramesh A. The use of molecular xenomonitoring for surveillance of mosquito-borne diseases. Philosophical Transactions of the Royal Society of London. Series B, Biological Sciences. 1818;2021(376):20190816. DOI: 10.1098/rstb.2019.0816
68.Gashaw T, Hagos B, Sisay M. Expected impacts of COVID-19: Considering resource-limited countries and vulnerable population. Frontiers in Public Health. 2021;9:614789. DOI: 10.3389/fpubh.2021.614789
69.FIND. Marginalized populations. 2022. Available from: https://www.finddx.org/marginalized-populations/
70.Wadagni A et al. Simple, rapid Mycobacterium ulcerans disease diagnosis from clinical samples by fluorescence of Mycolactone on thin layer chromatography. PLoS Neglected Tropical Diseases. 2015;9(11):e0004247. DOI: 10.1371/journal.pntd.0004247
71.Sima N et al. SHERLOCK4HAT: A CRISPR-based tool kit for diagnosis of human African trypanosomiasis. eBioMedicine. 2022;85:104308. DOI: 10.1016/j.ebiom.2022.104308
72.Bottieau E, Clerinx J. Human African trypanosomiasis: Progress and stagnation. Infectious Disease Clinics of North America. 2019;33(1):61-77. DOI: 10.1016/j.idc.2018.10.003
73.Kuhne V, Buscher P. The unknown nature of the antigen in the direct agglutination test for visceral leishmaniasis hampers development of serodiagnostic tests. The American Journal of Tropical Medicine and Hygiene. 2019;100(2):246-255. DOI: 10.4269/ajtmh.18-0740
74.Magnus E, Vervoort T, Van Meirvenne N. A card-agglutination test with stained trypanosomes (C.A.T.T.) for the serological diagnosis of T. B. gambiense trypanosomiasis. Annales de la Société Belge de Médecine Tropicale. 1978;58(3):169-176
75.Lejon V et al. The separation of trypanosomes from blood by anion exchange chromatography: From Sheila Lanham’s discovery 50 years ago to a gold standard for sleeping sickness diagnosis. PLoS Neglected Tropical Diseases. 2019;13(2):e0007051. DOI: 10.1371/journal.pntd.0007051
76.Penchenier L et al. Evaluation of LATEX/T.b.gambiense for mass screening of Trypanosoma brucei gambiense sleeping sickness in Central Africa. Acta Tropica. 2003;85(1):31-37. DOI: 10.1016/s0001-706x(02)00232-2
77.Farahmand M et al. Assessment of recombinant A2-latex agglutination test (RA2-LAT) and RA2-ELISA for detection of canine visceral leishmaniasis: A comparative field study with direct agglutination test in Northwestern Iran. Iranian Journal of Parasitology. 2018;13(2):172-179
78.Hasker E et al. A new format of the CATT test for the detection of human African trypanosomiasis, designed for use in peripheral health facilities. Tropical Medicine & International Health. 2010;15(2):263-267. DOI: 10.1111/j.1365-3156.2009.02446.x
79.Lumbala C et al. Prospective evaluation of a rapid diagnostic test for Trypanosoma brucei gambiense infection developed using recombinant antigens. PLoS Neglected Tropical Diseases. 2018;12(3):e0006386. DOI: 10.1371/journal.pntd.0006386
80.Schallig HD, Canto-Cavalheiro M, da Silva ES. Evaluation of the direct agglutination test and the rK39 dipstick test for the sero-diagnosis of visceral leishmaniasis. Memórias do Instituto Oswaldo Cruz. 2002;97(7):1015-1018. DOI: 10.1590/s0074-02762002000700015
81.Abbott. Bioline™ CHAGAS Ab ANTIBODY TEST FOR TRYPANOSOMA CRUZI (CHAGAS) [Internet]. 2022. Available from: https://chembio.com/products/chagas-stat-pak-assay-europe/ [Accessed: December 23, 2022]
82.InBios-International. Chagas Detect™ Plus Rapid Test: FDA Cleared for In Vitro Diagnostic Use in the United States [Internet]. 2022. Available from: https://inbios.com/chagas-detecttm-plus-rapid-test-intl-fda-cleared/ [Accessed: December 03, 2022]
83.InBios-International. Trypanosoma Detect™ Rapid Test [Internet]. 2022. Available from: https://inbios.com/trypanosoma-detecttm-rapid-test-intl/ [Accessed: December 23, 2022]
84.Diagnostics, F. Chagas Antibody Test [Internet]. 2022. Available from: https://www.fortressdiagnostics.com/products/rapid-diagnostic-tests/chagas-antibody-test [Accessed: December 30, 2022]
85.CHEMBIO. Chagas STAT PAK® Assay: Rapidly Detect Chagas Infection [Internet]. 2022. Available from: https://chembio.com/products/chagas-stat-pak-assay-europe/ [Accessed: December 20, 2022]
86.Abbott. Bioline™ ONCHO/IF IGG4 Biplex: New Tools to Support Disease Elimination for Both River Blindness and Elephantiasis [Internet]. 2022. Available from: https://www.globalpointofcare.abbott/en/product-details/bioline-onchocerciasis-LF-igg4-rapid-test.html [Accessed: December 03, 2022]
87.Fotress-Diagnostics. Chlamydia Test [Internet]. 2022. Available from: https://www.fortressdiagnostics.com/products/rapid-diagnostic-tests/chlamydia-test [Accessed: December 08, 2022]
88.Cypress-Diagnostics. Chlamydia Ag. [Internet]. 2022. Available from: https://diagnostics.be/fr/product/322 [Accessed: December 03, 2022]
89.Diagnostics, F. Dengue Fever [Internet]. 2022. Available from: https://www.fortressdiagnostics.com/products/rapid-diagnostic-tests/dengue-fever [Accessed: December 09, 2022]
90.Cypress-Diagnostics. Dengue NS1 Rapid Antigen Test for Dengue Fever [Internet]. 2022. Available from: https://fgmdiagnostici.it/files/78.pdf [Accessed: December 05, 2022]
91.CTK-Biotech. Chikungunya IgM Combo Rapid Test CE [Internet]. 2022. Available from: https://ctkbiotech.com/product/chikungunya-igm-combo-rapid-test-ce/ [Accessed: December 15, 2022]
92.Abbott. SD BIOLINE Chikungunya IgM: One Step IgM antibodies to Chikungunya virus Test [Internet]. 2022. Available from: https://maxanim.com/content/abbott/sd-bioline/sd-bioline-chikungunya-igm.pdf [Accessed: December 15, 2022]
93.Abbott. AlereTM Filariasis Test Strip [Internet]. 2022. Available from: https://www.cor-ntd.org/sites/default/files/content/document/FTS_v2_07JUL2016.pdf [Accessed: December 15, 2022]
94.Reszon-Diagnostics. LYMPHATIC FILARIASIS RAPID TEST KIT BRUGIA RAPID TEST [Internet]. 2022. Available from: https://reszonics.com/products/infectious-diseases-diagnosis/lateral-flow-rapid-test/brugia-rapid-test/ [Accessed: December 15, 2022]
95.Ease-Medtrend-Biotech. Leishmania IGG/IGM Test [Internet]. 2022. Available from: http://www.atlas-link.com/english/product_s33.html [Accessed: December 21, 2022]
96.Bio-Rad. IT LEISH Individual Rapid Test [Internet]. 2022. Available from: https://www.bio-rad.com/sites/default/files/webroot/web/pdf/cdg/literature/16490_B-IT_LEISH-EN.pdf [Accessed: December 15, 2022]
97.Pattabhi S et al. Design, development and evaluation of rK28-based point-of-care tests for improving rapid diagnosis of visceral leishmaniasis. PLoS Neglected Tropical Diseases. 2010;4(9):e0000822. DOI: 10.1371/journal.pntd.0000822
98.Hagos DG et al. Performance of rapid rk39 tests for the diagnosis of visceral leishmaniasis in Ethiopia: A systematic review and meta-analysis. BMC Infectious Diseases. 2021;21(1):1166. DOI: 10.1186/s12879-021-06826-w
99.InBios-International. Kalazar Detect™ Rapid Test for Visceral Leishmaniasis [Internet]. 2022. Available from: https://inbios.com/kalazar-detecttm-rapid-test-for-visceral-leishmaniasis-intl/ [Accessed: December 21, 2022]
100.InBios-International. CL Detect™ Rapid Test for Cutaneous Leishmaniasis [Internet]. 2022. Available from: https://inbios.com/cl-detecttm-rapid-test-for-cutaneous-leishmaniasis-intl/ [Accessed: December 26, 2022]
101.CTK-Biotech. OnSite Leishmania Ab Rapid Test—Strip (Serum/Plasma) [Internet]. 2022. Available from: https://athenesedx.com/insert/R0122S.pdf [Accessed: December 19, 2022]
102.CTK-Biotech. Leishmania Ab Rapid Test CE [Internet]. 2022. Available from: https://ctkbiotech.com/product/leishmania-ab-rapid-test-ce/ [Accessed: December 21, 2022]
103.Tamarozzi F et al. Comparison of the diagnostic accuracy of three rapid tests for the serodiagnosis of hepatic cystic echinococcosis in humans. PLoS Neglected Tropical Diseases. 2016;10(2):e0004444. DOI: 10.1371/journal.pntd.0004444
104.Vircell-S.L. VIRAPID® HYDATIDOSIS [Internet]. 2022. Available from: https://www.vircell.com/producto/virapid-hydatidosis/ [Accessed: December 10, 2022]
105.ICST. ADAMU-CE [Internet]. 2022. Available from: https://icst.jp/english/products/pdf/adamu_ce_en.pdf [Accessed: December 26, 2022]
106.Creative-Diagnostics. Hydatidosis Rapid Test. 2022. Available from: https://www.creative-diagnostics.com/Hydatidosis-Test-132038-453.htm
107.Meridian-Healthcare. Echinococcus (Echi) IgG Rapid Test [Internet]. 2022. Available from: https://www.meridianhealthcare.it/echinococco-echi-igg-rapid-test/?lang=en [Accessed: December 15, 2022]
108.Eggerbauer E et al. Evaluation of six commercially available rapid immunochromatographic tests for the diagnosis of rabies in brain material. PLoS Neglected Tropical Diseases. 2016;10(6):e0004776. DOI: 10.1371/journal.pntd.0004776
109.Lechenne M et al. Validation of a rapid rabies diagnostic tool for field surveillance in developing countries. PLoS Neglected Tropical Diseases. 2016;10(10):e0005010. DOI: 10.1371/journal.pntd.0005010
110.Abbexa-Ltd. Rabies Virus Antigen Rapid Test Kit [Internet]. 2022. Available from: https://www.abbexa.com/rabies-virus-antigen-rapid-test-kit-colloidal-gold [Accessed: December 10, 2022]
111.Ict-diagnostics, Schisto POC-CCA®: Rapid test for qualitative detection of: Bilharzia (Schistosomiasis) [Internet]. 2022. Available from: http://www.ictdiagnostics.co.za/schistosomanew.html [Accessed: December 19, 2022]
112.Feng X et al. Dot immunogold filtration assay (DIGFA) with multiple native antigens for rapid serodiagnosis of human cystic and alveolar echinococcosis. Acta Tropica. 2010;113(2):114-120. DOI: 10.1016/j.actatropica.2009.10.003
113.Njiru ZK et al. African trypanosomiasis: Sensitive and rapid detection of the sub-genus Trypanozoon by loop-mediated isothermal amplification (LAMP) of parasite DNA. International Journal for Parasitology. 2008;38(5):589-599. DOI: 10.1016/j.ijpara.2007.09.006
114.Hossain F et al. Evaluation of Loopamp leishmania detection kit and leishmania antigen ELISA for post-elimination detection and Management of Visceral Leishmaniasis in Bangladesh. Frontiers in Cellular and Infection Microbiology. 2021;11:670759. DOI: 10.3389/fcimb.2021.670759
115.Gillet P et al. Assessment of the prozone effect in malaria rapid diagnostic tests. Malaria Journal. 2009;8:271. DOI: 10.1186/1475-2875-8-271
116.Alvarez-Rodriguez A et al. Recent progress in diagnosis and treatment of human African trypanosomiasis has made the elimination of this disease a realistic target by 2030. Frontiers in Medicine. 2022;9:1037094. DOI: 10.3389/fmed.2022.1037094
117.Land KJ et al. REASSURED diagnostics to inform disease control strategies, strengthen health systems and improve patient outcomes. Nature Microbiology. 2019;4(1):46-54. DOI: 10.1038/s41564-018-0295-3
118.Koczula KM, Gallotta A. Lateral flow assays. Essays in Biochemistry. 2016;60(1):111-120. DOI: 10.1042/EBC20150012
119.Desquesnes M et al. The analysis of the cross-reactions occurring in antibody-ELISA for the detection of trypanosomes can improve identification of the parasite species involved. Annals of Tropical Medicine and Parasitology. 2001;95(2):141-155. DOI: 10.1080/00034980120050251
120.Lejon V et al. Performance of enzyme-linked immunosorbent assays for detection of antibodies against T. congolense and T. vivax in goats. Veterinary Parasitology. 2003;116(2):87-95. DOI: 10.1016/s0304-4017(03)00257-7
121.Kennedy PGE. Update on human African trypanosomiasis (sleeping sickness). Journal of Neurology. 2019;266(9):2334-2337. DOI: 10.1007/s00415-019-09425-7
122.Büscher P. Diagnosis of human and animal African trypanosomiasis. In: Black SJ, Seed JR, editors. The African Trypanosomes. New York: Kluwer Academic Publishers; 2002. pp. 51-63. DOI: 10.1007/0-306-46894-8_5
123.Ross GMS et al. Unraveling the hook effect: A comprehensive study of high antigen concentration effects in Sandwich lateral flow immunoassays. Analytical Chemistry. 2020;92(23):15587-15595. DOI: 10.1021/acs.analchem.0c03740
124.Niemz A, Ferguson TM, Boyle DS. Point-of-care nucleic acid testing for infectious diseases. Trends in Biotechnology. 2011;29(5):240-250. DOI: 10.1016/j.tibtech.2011.01.007
125.Matthew MA, Christie J, Yang N, Yao C. A loop-mediated isothermal amplification (LAMP) assay specific to trichomonas tenax is suitable for use at point-of-care. Microorganisms. Microorganisms. 2022;10:594. DOI: 10.3390/microorganisms10030594
126.Zou Y, Mason MG, Botella JR. Evaluation and improvement of isothermal amplification methods for point-of-need plant disease diagnostics. PLoS One. 2020;15(6):e0235216. DOI: 10.1371/journal.pone.0235216
127.Buscher P, Deborggraeve S. How can molecular diagnostics contribute to the elimination of human African trypanosomiasis? Expert Review of Molecular Diagnostics. 2015;15(5):607-615. DOI: 10.1586/14737159.2015.1027195
128.Wastling SL et al. LAMP for human African trypanosomiasis: A comparative study of detection formats. PLoS Neglected Tropical Diseases. 2010;4(11):e865. DOI: 10.1371/journal.pntd.0000865
129.Njiru ZK. Rapid and sensitive detection of human African trypanosomiasis by loop-mediated isothermal amplification combined with a lateral-flow dipstick. Diagnostic Microbiology and Infectious Disease. 2011;69(2):205-209. DOI: 10.1016/j.diagmicrobio.2010.08.026
130.Tanner NA, Zhang Y, Evans TC Jr. Visual detection of isothermal nucleic acid amplification using pH-sensitive dyes. BioTechniques. 2015;58(2):59-68. DOI: 10.2144/000114253
131.Pinto J et al. Structural basis for the high specificity of a Trypanosoma congolense immunoassay targeting glycosomal aldolase. PLoS Neglected Tropical Diseases. 2017;11(9):e0005932. DOI: 10.1371/journal.pntd.0005932
132.Pardon E et al. A general protocol for the generation of nanobodies for structural biology. Nature Protocols. 2014;9(3):674-693. DOI: 10.1038/nprot.2014.039
133.Luka G et al. Microfluidics integrated biosensors: A leading technology towards lab-on-a-Chip and Sensing applications. Sensors (Basel). 2015;15(12):30011-30031. DOI: 10.3390/s151229783
134.Hagihara Y, Saerens D. Engineering disulfide bonds within an antibody. Biochimica et Biophysica Acta. 2014;1844(11):2016-2023. DOI: 10.1016/j.bbapap.2014.07.005
135.Muyldermans S. Nanobodies: Natural single-domain antibodies. Annual Review of Biochemistry. 2013;82:775-797. DOI: 10.1146/annurev-biochem-063011-092449
136.Polonelli L et al. Antibody complementarity-determining regions (CDRs) can display differential antimicrobial, antiviral and antitumor activities. PLoS One. 2008;3(6):e2371. DOI: 10.1371/journal.pone.0002371
137.Charles A, Janeway J, Travers P, Walport M, Shlomchik MJ. The structure of a typical antibody molecule, in Immunobiology: The Immune System in Health and Disease. New York: Garland Science; 2001
138.Kubala MH et al. Structural and thermodynamic analysis of the GFP:GFP-nanobody complex. Protein Science. 2010;19(12):2389-2401. DOI: 10.1002/pro.519
139.Pagneux Q et al. SARS-CoV-2 detection using a nanobody-functionalized voltammetric device. Communications Medicine. 2022;2:56. DOI: 10.1038/s43856-022-00113-8
140.Heukers R, De Groof TWM, Smit MJ. Nanobodies detecting and modulating GPCRs outside in and inside out. Current Opinion in Cell Biology. 2019;57:115-122. DOI: 10.1016/j.ceb.2019.01.003
141.Jovcevska I, Muyldermans S. The therapeutic potential of nanobodies. BioDrugs. 2020;34(1):11-26. DOI: 10.1007/s40259-019-00392-z
142.Sohier JS et al. Allosteric inhibition of VIM metallo-beta-lactamases by a camelid nanobody. The Biochemical Journal. 2013;450(3):477-486. DOI: 10.1042/BJ20121305
143.Staus DP et al. Regulation of beta2-adrenergic receptor function by conformationally selective single-domain intrabodies. Molecular Pharmacology. 2014;85(3):472-481. DOI: 10.1124/mol.113.089516
144.Vincke C, Muyldermans S. Introduction to heavy chain antibodies and derived nanobodies. Methods in Molecular Biology. 2012;911:15-26. DOI: 10.1007/978-1-61779-968-6_2
145.Kariuki CK, Magez S. Improving the yield of recalcitrant nanobodies(R) by simple modifications to the standard protocol. Protein Expression and Purification. 2021;185:105906. DOI: 10.1016/j.pep.2021.105906
146.Scully M et al. Caplacizumab treatment for acquired thrombotic thrombocytopenic purpura. The New England Journal of Medicine. 2019;380(4):335-346. DOI: 10.1056/NEJMoa1806311
147.Kratz F, Elsadek B. Clinical impact of serum proteins on drug delivery. Journal of Controlled Release. 2012;161(2):429-445. DOI: 10.1016/j.jconrel.2011.11.028
148.Wagner TR et al. NeutrobodyPlex-monitoring SARS-CoV-2 neutralizing immune responses using nanobodies. EMBO Reports. 2021;22(5):e52325. DOI: 10.15252/embr.202052325
149.Li Z et al. An unbiased immunization strategy results in the identification of enolase as a potential marker for nanobody-based detection of Trypanosoma evansi. Vaccines (Basel). 2020;8(3):415. DOI: 10.3390/vaccines8030415
150.Obishakin E et al. Generation of a nanobody targeting the paraflagellar rod protein of trypanosomes. PLoS One. 2014;9(12):e115893. DOI: 10.1371/journal.pone.0115893
151.Ditlev SB et al. Utilizing nanobody technology to target non-immunodominant domains of VAR2CSA. PLoS One. 2014;9(1):e84981. DOI: 10.1371/journal.pone.0084981
152.Deckers N et al. Nanobodies, a promising tool for species-specific diagnosis of taenia solium cysticercosis. International Journal for Parasitology. 2009;39(5):625-633. DOI: 10.1016/j.ijpara.2008.10.012
153.Liu Y et al. Ultrasensitive and highly specific lateral flow assays for point-of-care diagnosis. ACS Nano. 2021;15(3):3593-3611. DOI: 10.1021/acsnano.0c10035
154.Sena-Torralba A et al. Toward next generation lateral flow assays: Integration of nanomaterials. Chemical Reviews. 2022;122(18):14881-14910. DOI: 10.1021/acs.chemrev.1c01012
155.Sun W et al. A novel multi-walled carbon nanotube-based antibody conjugate for quantitative and semi-quantitative lateral flow assays. Bioscience, Biotechnology, and Biochemistry. 2017;81(10):1874-1882. DOI: 10.1080/09168451.2017.1365590
156.Porras JC et al. Comparative study of gold and carbon nanoparticles in nucleic acid lateral flow assay. Nanomaterials (Basel). 2021;11(3):741. DOI: 10.3390/nano11030741
157.Miller BS et al. Spin-enhanced nanodiamond biosensing for ultrasensitive diagnostics. Nature. 2020;587(7835):588-593. DOI: 10.1038/s41586-020-2917-1
158.Amadeo Sena-Torralba HT-M, Parolo C, Ranjbar S, Nejad MAF, Álvarez-Diduk R, Idili A, et al. A novel Ratiometric fluorescent approach for the modulation of the dynamic range of lateral flow immunoassays. Advanced Materials Technologies. 2022;7. DOI: 10.1002/admt.202101450
159.Shah KG, Yager P. Wavelengths and lifetimes of paper autofluorescence: A simple substrate screening process to enhance the sensitivity of fluorescence-based assays in paper. Analytical Chemistry. 2017;89(22):12023-12029. DOI: 10.1021/acs.analchem.7b02424
160.Dutta Chowdhury A et al. Femtomolar detection of dengue virus DNA with serotype identification ability. Analytical Chemistry. 2018;90(21):12464-12474. DOI: 10.1021/acs.analchem.8b01802
161.Hajian R et al. Detection of unamplified target genes via CRISPR-Cas9 immobilized on a graphene field-effect transistor. Nature Biomedical Engineering. 2019;3(6):427-437. DOI: 10.1038/s41551-019-0371-x
162.Guo K et al. Rapid single-molecule detection of COVID-19 and MERS antigens via nanobody-functionalized organic electrochemical transistors. Nature Biomedical Engineering. 2021;5(7):666-677. DOI: 10.1038/s41551-021-00734-9
163.Nuzaihan MNM et al. Electrical detection of dengue virus (DENV) DNA oligomer using silicon nanowire biosensor with novel molecular gate control. Biosensors & Bioelectronics. 2016;83:106-114. DOI: 10.1016/j.bios.2016.04.033
164.Dalila RN, Azman MF, Rajaahmoorthi M, Arshad MKM, Fathil MFM, Nuzaihan M, et al. Silicon-on-insulator FET biosensor for dengue DNA complementation. AIP Conference Proceedings. 2018;2045(1):020037-7. DOI: 10.1063/1.5080850
165.Rodriguez MO et al. Silver and gold enhancement methods for lateral flow immunoassays. Talanta. 2016;148:272-278. DOI: 10.1016/j.talanta.2015.10.068
166.Gao Z et al. Platinum-decorated gold nanoparticles with dual functionalities for ultrasensitive colorimetric in vitro diagnostics. Nano Letters. 2017;17(9):5572-5579. DOI: 10.1021/acs.nanolett.7b02385
167.Arshavsky-Graham S, Segal E. Lab-on-a-chip devices for point-of-care medical diagnostics. Advances in Biochemical Engineering/Biotechnology. 2022;179:247-265. DOI: 10.1007/10_2020_127
169.Byun J. Recent progress and opportunities for nucleic acid aptamers. Life (Basel). 2021;11(3):193. DOI: 10.3390/life11030193
170.Deroco PB, Kubota DWJLT. Recent advances in point-of-care biosensors for the diagnosis of neglected tropical diseases. Sensors and Actuators B: Chemical. 2021;349:130821. DOI: 10.1016/j.snb.2021.130821
171.Sereno D et al. Isothermal nucleic acid amplification to detect infection caused by parasites of the Trypanosomatidae family: A literature review and opinion on the laboratory to field applicability. International Journal of Molecular Sciences. 2022;23(14):7543. DOI: 10.3390/ijms23147543
173.Li L et al. HOLMESv2: A CRISPR-Cas12b-assisted platform for nucleic acid detection and DNA methylation quantitation. ACS Synthetic Biology. 2019;8(10):2228-2237. DOI: 10.1021/acssynbio.9b00209
174.Gootenberg JS et al. Multiplexed and portable nucleic acid detection platform with Cas13, Cas12a, and Csm6. Science. 2018;360(6387):439-444. DOI: 10.1126/science.aaq0179
175.Lee RA et al. Ultrasensitive CRISPR-based diagnostic for field-applicable detection of Plasmodium species in symptomatic and asymptomatic malaria. Proceedings of the National Academy of Sciences of the United States of America. 2020;117(41):25722-25731. DOI: 10.1073/pnas.2010196117
176.Portney LG, Watkins MP. Foundations of Clinical Research: Applications to Practice. 3rd ed. Philadelphia: F. A. Davis Company; 2015. p. 892. ISBN 10987654321
Written By
Andrés Álvarez-Rodríguez, Magdalena Radwanska, Stefan Magez and Steven Odongo
Submitted: 04 January 2023Reviewed: 06 January 2023Published: 08 February 2023
 Open access peer-reviewed chapter
Open access peer-reviewed chapter