 Open access peer-reviewed chapter
Open access peer-reviewed chapter
Abstract
This chapter provides an in-depth exploration of cartilage, a pivotal component crucial for joint health, particularly within the context of osteoarthritis (OA). It delves deeply into the intricate structure and dynamic functions of articular cartilage, elucidating its essential roles in load-bearing, shock absorption, and maintaining joint stability. Emphasizing the delicate balance of cellular components, such as chondrocytes, and extracellular matrix constituents like proteoglycans and collagens, which collectively ensure the mechanical and biological integrity of cartilage, the discussion places significant attention on factors influencing cartilage homeostasis and contributing to its eventual degradation, analyzing age-related changes, mechanical stress, and genetic predispositions, alongside the impact of inflammatory processes and cytokine imbalances. By highlighting the multifaceted interplay among these factors, a clear narrative emerges, elucidating the initiation of OA. Furthermore, the chapter investigates into the cascade of events that define OA pathogenesis, dissecting the underlying mechanisms responsible for cartilage damage and matrix degradation, tracing their combined contribution toward the development of OA. In its focus on OA’s etiology, the chapter underscores importance of comprehending cartilage alterations as a critical starting point for designing therapeutic interventions aimed at effectively managing OA.
Keywords
- cartilage structure
- cartilage function
- cartilage degradation
- cartilage repair
- osteoarthritis pathogenesis
1. Introduction
Cartilage, a specialized type of connective tissue, plays a fundamental role in providing structural support and maintaining the integrity of various body structures. It exists in several forms, with each type adapted to specific functions and anatomical locations. The three main types of cartilage include hyaline cartilage, elastic cartilage, and fibrocartilage. Hyaline cartilage, recognized by its smooth and glassy appearance, occupies areas like the articular surfaces of joints. It functions as a protective cushion between bones, facilitating frictionless movements. Fibrocartilage, in contrast, boasts resilience and durability due to its high collagen fiber density. This type is prevalent in structures like intervertebral discs, contributing to shock absorption and stability. Elastic cartilage, containing both elastic fibers and collagen, is situated in regions requiring a blend of flexibility and support. Examples include the external ear and the epiglottis [1].
Articular cartilage, a specialized form of connective tissue, envelops the articulating surfaces of bones within synovial joints. It holds a pivotal role in enabling fluid and frictionless motion, guaranteeing joint stability, and effectively distributing mechanical loads across the joint surfaces. On one side, the articular cartilage interfaces with the joint cavity, providing the essential low-friction surface required for seamless joint movement. On the opposing side, it connects to the underlying subchondral bone plate
Referred to as hyaline cartilage due to its glassy and translucent appearance under microscopic observation, this specialized tissue boasts a distinctive and organized structure, which, when combined with its highly specialized composition, endows it with remarkable resilience against high compressive forces. These biophysical properties play a critical role in upholding the mechanical strength and durability of joints, particularly during weight-bearing activities. The amorphous nature of the articular cartilage, coupled with its lubricated surface and capacity to withstand substantial compressive forces, grants it the ability to withstand the repetitive movements and mechanical stresses inherent in joint motion. The absence of this smooth, wear-resistant cartilage surface would jeopardize joint functioning, leading to heightened friction and wear and the potential onset of painful joint conditions [3, 4].
Understanding articular cartilage is of paramount importance for unveiling the mechanisms that underlie joint diseases, notably osteoarthritis (OA), characterized by the gradual deterioration of cartilage. This condition impacts millions worldwide, serving as a major source of pain, disability, and compromised quality of life. Through the exploration of cellular and molecular processes governing cartilage health and degeneration, researchers can gain insights into the pathophysiology of OA, potentially paving the way for innovative therapeutic strategies. Moreover, advancements in regenerative medicine and tissue engineering hinge on a profound comprehension of articular cartilage. Crafting effective treatments for cartilage injuries and ailments demands a grasp of cartilage biology, biomechanics, and the intricate interplay between cells and the extracellular matrix components. Against the backdrop of mounting demand for joint-preserving interventions, the study of articular cartilage assumes pivotal significance, guiding the creation of interventions aimed at restoring its structure and function, thus mitigating the necessity for invasive joint replacement surgeries. Furthermore, as the global population ages and musculoskeletal disorders become more prevalent, a growing necessity emerges for early detection and intervention to prevent or delay cartilage degeneration. Research endeavors into noninvasive imaging techniques, biomarkers, and risk factors associated with cartilage deterioration hold the potential to identify individuals at risk of joint diseases, enabling timely interventions and personalized treatment strategies.
In conclusion, the study of articular cartilage transcends its structural and functional implications. It serves as the gateway to deciphering joint diseases, advancing regenerative therapies, and elevating the well-being of individuals dealing with joint-related conditions. By illuminating the intricate biology of this pivotal tissue, researchers and healthcare practitioners lay the groundwork for more efficacious treatments, early interventions, and improved joint health on a global scale.
2. Structure
The articular cartilage consists of chondrocytes, which are its resident cells, along with an extracellular matrix primarily comprised of collagen fibers, proteoglycans, and water. This combination, along with the pericellular matrix of chondrocytes, is collectively termed as the chondron [3]. Refer to Figure 1 for an illustration of the structure of articular/hyaline cartilage.
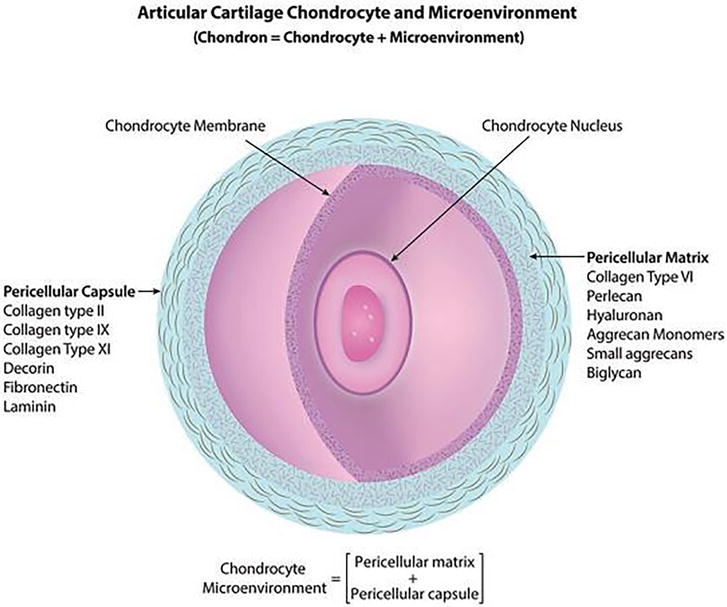
Figure 1.
A chondrocyte along with its surrounding microenvironment has been depicted in this picture. The membrane of the chondrocyte is encompassed by a delicate pericellular matrix consisting of type VI collagen, along with various minor glycoproteins and proteoglycans. This pericellular matrix is enveloped by a fibrous pericellular capsule composed of collagens and non-collagen proteins [
2.1 Extracellular matrix (ECM)
Water dominates the extracellular matrix (ECM) of articular cartilage, constituting approximately 65–80% of its wet weight. As the cartilage traverses various zones, the water content decreases from roughly 80% in the superficial zone to around 65% in the deep zone [1, 2]. Water’s pivotal role in upholding cartilage’s structure and function cannot be overstated. A core function of water is hydrating the proteoglycans within the ECM. These proteoglycans, in partnership with water molecules, facilitate the expansion of the collagen network, endowing the cartilage with resilience and flexibility. Moreover, water functions as a lubricant within the joint, promoting smooth movement, while also aiding in the transportation of vital nutrients to cartilage cells [3]. The presence of water in the ECM is meticulously regulated through interactions with proteoglycans and collagens. Electrolytes, including sodium, potassium, chloride, and calcium, are integral components of this aqueous medium, further contributing to the maintenance of cartilage’s biochemical equilibrium [1]. Over a person’s lifespan, the water content in articular cartilage tends to diminish. However, individuals grappling with osteoarthritis (OA) may witness an increase in water content to approximately 90%. This surge in water content is linked to alterations in the mechanical properties of cartilage, resulting in reduced strength and heightened permeability (as depicted in Figure 2) [3, 4].
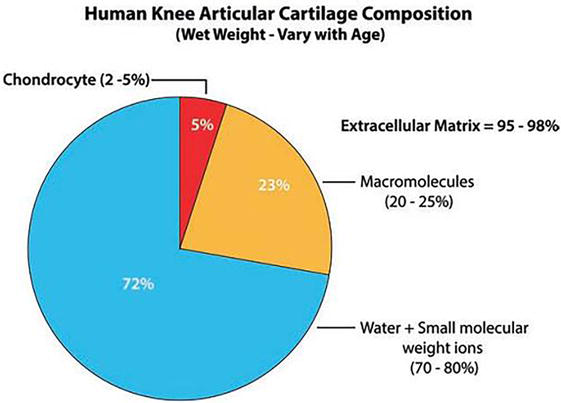
Figure 2.
The composition of wet weight in the knee joint cartilage of the human adult reveals that chondrocytes constitute a mere 2–5% of the total weight, while the bulk of 95–98% is composed of the extracellular matrix. This matrix is largely comprised of tissue fluid and low molecular weight ions. It is worth noting that the wet weight of the macromolecules in knee articular cartilage differs based on both age and the specific anatomical location [
The second most abundant component of the articular cartilage’s extracellular matrix is collagen. Chondrocytes, the specialized cells within the cartilage, secrete collagen in the form of procollagen molecules. These procollagen molecules undergo enzymatic cleavage of their C- and N-propeptides within the extracellular matrix (ECM). This processing step is essential for the normal growth of collagen fibrils. Intriguingly, even N-procollagen that has undergone partial processing can still come together to form slender collagen fibrils. Upon entering the extracellular matrix (ECM), these collagen molecules engage with one another and collaboratively polymerize to establish a fibrillar structure. The enduring structural integrity of these collagen fibrils is subsequently reinforced through the formation of covalent cross-links. These cross-links happen between adjoining collagen chains (referred to as intramolecular cross-links) and between neighboring collagen molecules (known as intermolecular cross-links). These cross-links provide a robust and resilient structure, crucial for maintaining the integrity and mechanical properties of the articular cartilage [3]. In human articular cartilage, collagen type II is the primary structural protein, making up approximately 90–95% of the total collagen content. The remaining 5–10% of collagen is composed of other cartilage-specific and nonspecific collagens, accounting for about 1% of the cartilage’s dry weight (Figure 3) [5].
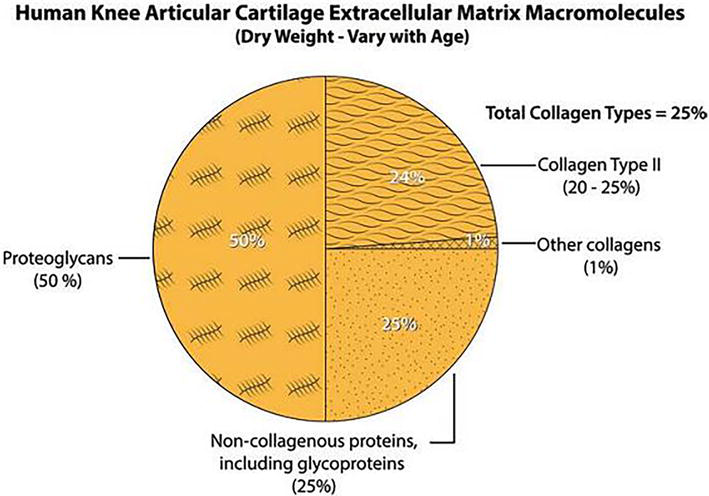
Figure 3.
The composition of macromolecules by dry weight in the extracellular matrix of hyaline cartilage within the human adult knee. It is important to observe that the dry weight of these molecules within the articular cartilage fluctuates based on both age and the specific anatomical location [
Interestingly, the turnover rate of collagen type II in normal adult cartilage is exceedingly slow, with a half-life of over 100 years. In contrast, proteoglycans (PGs) and aggrecans, which are essential components of the cartilage’s extracellular matrix (ECM), continue to be produced and secreted throughout life. The usual turnover rate for a large monomer of PG corresponds to a half-life of about 3.4 years [6]. This dynamic balance between collagen and proteoglycan turnover is crucial for maintaining cartilage structure and function. Besides collagen and proteoglycans, other non-collagenous proteins play a significant role in the ECM’s composition, constituting approximately 25% of the dry weight depending on age. These proteins include laminin, fibronectin, chondronectin, tenascin, cartilage matrix glycoprotein (CMGP), and cartilage oligomeric matrix protein (COMP). These glycoproteins contribute to the structural organization and integrity of the ECM, promoting cell–matrix interactions and tissue stability [1]. Collagen derives its impressive tensile strength from a unique triple-helix structure, where three polypeptide chains are intertwined through hydrogen bonds. Each polypeptide consists of an iterating sequence of amino acids: proline, glycine, and hydroxyproline, forming a left-handed helical structure through additional hydrogen bonds [7]. Although Type II collagen is the most studied collagen, yet other collagen types, such as Types IV, VI, IX, X, XI, XII, XIII, and XIV, also exist in articular cartilage. These less-studied collagen fibers might offer valuable insights into disease progression and potential biomarkers for improved treatment [3, 4, 5]. Collagen is distributed throughout the extracellular matrix, and its arrangement varies depending on the regional differences within the joint cartilage (different zones). Additionally, the density of collagen is higher at the apical surface of a chondron compared to at the basal side [5]. Collagen forms associations and cross-links with proteoglycans, creating the fundamental organizational unit of the extracellular matrix (Figure 4) [3].
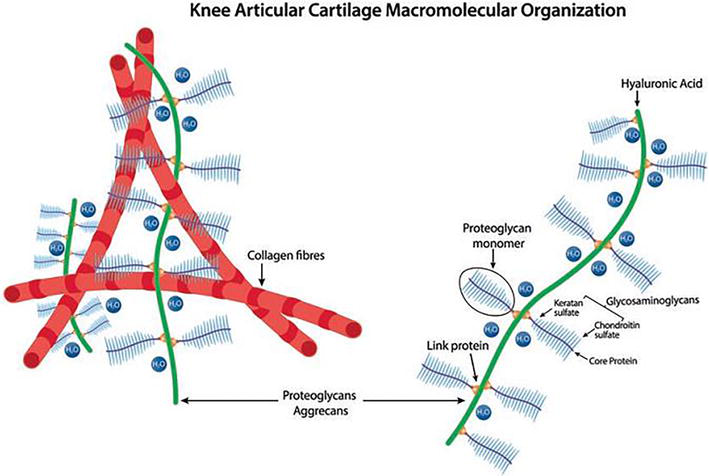
Figure 4.
The picture depicts interaction and arrangement of collagen and aggrecan within the articular cartilage. The basic structure of the proteoglycan monomer comprises a central protein core that is linked through covalent bonds to glycosaminoglycan side chains, specifically keratan sulfate and chondroitin sulfate. These monomers are connected to the hyaluronic acid back through a region that binds hyaluronic acid (referred to as the hyaluronic acid-binding region), which is additionally stabilized by the presence of the link protein [
Proteoglycans are another essential component of the extracellular matrix and are found throughout the connective tissues. They contribute to the strength of the matrix and are hydrophilic due to their negative charges. This hydrophilic property plays a crucial role in facilitating the lubrication of the joint’s bearing surfaces, ensuring smooth and frictionless movement during joint motion, minimizing wear and tear on the cartilage surface. Proteoglycans are proteins covalently linked to glycosaminoglycans (GAGs), which are repetitive dimers of a hexosamine and a uronic acid [3, 7]. In articular cartilage, proteoglycans exhibit significant variability in their size, glycosaminoglycan (GAG) content, and functional properties. The proteoglycans (PGs) can be classified into two major groups based on their properties and functions. The first group comprises large aggregating PGs, which include molecules like aggrecan and versican. These large aggregating PGs are responsible for forming complex structures that can trap and retain a significant amount of water, backing to the cartilage’s ability to endure compressive forces and maintain its elasticity. They make up a substantial portion of the total PGs, accounting for about 50–58%. The second group consists of non-aggregating PGs, making up approximately 40% of the total PGs [7, 8]. Unlike the large aggregating PGs, non-aggregating PGs do not form extensive complexes with water. Instead, they serve other crucial functions within the cartilage matrix. These non-aggregating PGs play roles in cell signaling, tissue organization, and interacting with other components of the extracellular matrix. The balance between these two types of PGs is essential for maintaining the overall structure and function of articular cartilage [3, 4, 8]. In the case of aggrecan, the major GAGs attached are chondroitin sulfate and keratin sulfate. Hyaluronic acid (HA) is another crucial GAG for the function and structure of articular cartilage. Although it does not form covalent bonds to proteins like other proteoglycans, yet hyaluronic acid plays a significant role by making non-covalent complexes with proteoglycans, particularly aggrecan, through proteoglycan link proteins. Collectively, hyaluronic acid and proteoglycans form extensive proteoglycan-hyaluronic acid aggregates that fix to the surface of collagen II fibers by their side chains, creating strong connections among all ECM constituents and forming the resilient backbone of hyaline cartilage [8].
2.2 Chondrocytes
Chondrocytes represent the vital cellular component of cartilage that is housed within small spaces called lacunae. Despite their significance, chondrocytes account for only about 5% of the total volume of articular cartilage [9]. These chondrocytes exhibit diverse morphologies, transitioning from flat, discoid-shaped cells at the surface of the cartilage to round or polygonal shapes as we move deeper into the cartilage tissue. These spheroidal cells are not uniformly distributed but rather form clusters known as isogenous groups, and their metabolic activity plays a vital role in sustaining the integrity of the extracellular matrix surrounding them [9]. One of the unique aspects of chondrocytes’ environment is its hypoxic nature, meaning it has a low oxygen concentration. As a result, a considerable portion of the chondrocytes’ metabolic processes is anaerobic, not reliant on oxygen [3, 4]. These anaerobic pathways are adapted to the specific conditions of the cartilage, allowing chondrocytes to thrive in this oxygen-deprived environment [3]. Chondrocytes originate from mesenchymal stem cells, which differentiate into specialized cells called chondroblasts. The chondroblasts then play a critical role in the formation and secretion of the essential components of the ECM, such as collagens and proteoglycans [10]. These ECM components provide the cartilage with its structural framework and mechanical properties. As chondroblasts continue to synthesize the ECM, they eventually become surrounded and completely embedded by the matrix they produce. At this point, they are referred to as chondrocytes [8, 10]. Once chondrocytes are fully enclosed within their lacunae, they remain metabolically active and continue to maintain the cartilage’s health and function. Overall, chondrocytes are vital cellular units within cartilage responsible for ECM maintenance and ensuring proper cartilage structure and function. Their ability to adapt to the unique hypoxic environment of cartilage and the ongoing metabolic processes is crucial for the long-term health and integrity of articular cartilage [3, 4]. Understanding the behavior of chondrocytes and their role in cartilage physiology is essential for developing effective therapies to address cartilage-related disorders and promote joint health.
2.3 Zones
Articular cartilage can be divided into distinct zones based on their unique structural and functional characteristics (Figure 5) [11].
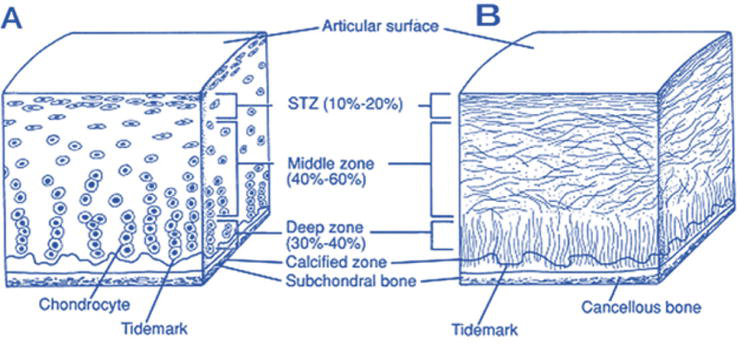
Figure 5.
A cross-sectional schematic diagram of intact articular cartilage is displayed, illustrating two main aspects: (A) the cellular arrangement across different zones within the articular cartilage structure and (B) the intricate architecture of collagen fibers [
To conclude, the zonal organization of articular cartilage enables it to withstand the various mechanical stresses imposed during joint movement. Each zone possesses distinct structural characteristics and functions, contributing to the overall mechanical properties and resilience of articular cartilage in maintaining smooth joint articulation and joint health [3, 13].
2.4 Regions
The extracellular matrix (ECM) of articular cartilage exhibits distinct regions based on their proximity to chondrocytes, composition, and organization of collagen fibrils. These regions can be categorized into pericellular, territorial, and interterritorial regions [3, 4].
The
The
The
In summary, the ECM of articular cartilage can be subdivided into pericellular, territorial, and interterritorial regions, each with unique compositions and functions. These distinct regions work in harmony to maintain the cartilage’s mechanical integrity, ensuring smooth joint movement and providing essential protection and support to chondrocytes in response to various mechanical stresses.
3. Functions of articular cartilage
Cartilage plays a paramount role in joint function and mobility; operating as a silent yet essential partner, it orchestrates an array of indispensable mechanisms that are pivotal for sustaining seamless and pain-free movement. It operates as a cushion, a shock absorber, a load distributor, and a friction-reducing agent, all of which contribute to the smooth functioning of joint.
3.1 Smooth articulation
One of the primary functions of articular cartilage is to facilitate smooth articulation between bones in the joints. By preventing bone-to-bone contact, cartilage ensures that the joint surfaces can move smoothly against each other. During joint movement, such as flexion and extension, the smooth articulation provided by cartilage reduces the impact and shear forces on the joint. This helps to prevent excessive wear and tear on the cartilage and underlying bones. Without the protective cushioning and smoothness of cartilage, joint surfaces would be subjected to direct contact, leading to damage, inflammation, and pain over time [14].
3.2 Load distribution
Articular cartilage serves as a load-bearing surface within the joints, by distributing the mechanical forces and loads that occur during movement. This function is essential for preventing excessive stress on specific areas of the joint and ensuring uniform force distribution across the entire joint surface. During weight-bearing activities like walking, running, or lifting, the joints experience substantial compressive forces. These forces can be quite significant, especially in weight-bearing joints like the knees and hips. Without the load distribution function of articular cartilage, the joint surfaces would be subject to concentrated pressure, which could lead to local damage, wear, and ultimately joint degeneration. The collagen fiber network within the cartilage provides structural support and enhances its load distribution capacity. Collagen fibers are arranged in a specific pattern, enabling the cartilage to resist tensile and shear forces effectively. These fibers work in conjunction with the proteoglycans to disperse loads evenly across the joint surface [7, 14].
3.3 Low-friction surface
The unique composition of cartilage, particularly the presence of proteoglycans and synovial fluid, creates a low-friction surface within the joint. Cartilage is characterized by a very low coefficient of friction, both static (0.01–0.02) and dynamic (0.003). This minimizes the resistance during joint movement, allowing for smooth and effortless motion. As a result, cartilage enables a wide range of movements, including flexion, extension, rotation, and gliding, which are essential for activities of daily living and physical performance. This lubrication minimizes wear and tear on the joint surfaces, promoting longevity and preserving joint function [14].
3.4 Shock absorption
Cartilage’s ability to absorb shock is vital for protecting the joints and preventing injury during weight-bearing activities and impact-related movements. Articular cartilage may be collapsed by up to 40% of its resting height when subjected to physiological stresses [4]. This is secondary to its high elasticity and compressibility in turn provided by the collagen fiber network as well as proteoglycans owing to their capacity to bind water molecules and cations, allowing them to maintain high osmotic pressure within the cartilage [3, 4]. When pressure is applied to the joint during activities such as jumping or lifting heavy objects, the water within the cartilage matrix is forced out. This redistribution of fluid helps counteract the compressive forces and maintain joint stability. As the pressure is released, the water is reabsorbed, allowing the cartilage to return to its original shape and ensuring proper joint function. By absorbing and dissipating forces, cartilage reduces the risk of damage to both the joint surfaces and the surrounding structures. This shock-absorbing property is especially important in high-impact activities, such as running or jumping, where joints are subjected to increased stress [7, 14, 15].
3.5 Joint stability
Healthy cartilage plays a vital role in maintaining joint stability and overall joint health. Acting as a natural cushion between bones, cartilage prevents direct contact between joint surfaces during movement. This cushioning effect is crucial for reducing friction and wear on the bones, safeguarding them from damage and ensuring their longevity. Moreover, the smooth surface of cartilage allows bones to articulate seamlessly, further enhancing joint stability and preventing dislocations or subluxations [14].
In summary, cartilage is an indispensable tissue in joint function and mobility. Its ability to facilitate smooth articulation, distribute loads, provide a low-friction surface, absorb shock, and maintain joint stability is crucial for overall musculoskeletal health. Proper care and preservation of cartilage are essential to sustain joint function and prevent the onset of joint disorders, such as osteoarthritis, which can significantly impact an individual’s quality of life.
4. Factors influencing cartilage repair and regeneration
Cartilage has limited regenerative capacity due to its avascular nature and low cellular density. Nevertheless, cartilage repair and regeneration can occur to some extent under specific conditions. Several intrinsic and extrinsic factors influence the repair and regeneration processes. Understanding these factors is essential for developing strategies to enhance cartilage healing and to potentially address cartilage-related disorders such as osteoarthritis.
4.1 Age
Cartilage is known for its limited ability to self-repair, and this regenerative capacity diminishes with advancing age. Younger individuals generally exhibit better cartilage-healing capabilities compared to older individuals. Several factors contribute to this age-related decline in cartilage repair. One of the main reasons for reduced cartilage repair in older individuals is the decline in the metabolic activity of chondrocytes, the specialized cells responsible for maintaining cartilage. Chondrocytes play a vital role in synthesizing and maintaining the extracellular matrix (ECM) of cartilage, which includes collagen fibers and proteoglycans. As age progresses, the chondrocytes become less active and have a slower rate of ECM synthesis, thereby impairing their ability to repair damaged cartilage. Clinical evidence supports the notion that cartilage-healing capabilities decline with age. For example, studies have shown that cartilage injuries in young adults tend to heal more efficiently and produce better-quality repair tissue than in older adults [16]. A study published in the American Journal of Sports Medicine assessed cartilage repair outcomes in patients undergoing autologous chondrocyte implantation (ACI) for knee cartilage defects. The researchers found that younger patients (under 40 years old) achieved better outcomes in terms of cartilage repair and clinical improvement compared to older patients (over 40 years old) [17]. As a result of the reduced regenerative capacity, cartilage injuries in older individuals are less likely to heal completely. Instead, the body may initiate a repair response that leads to the formation of fibrocartilage, which is a structurally inferior tissue compared to native hyaline cartilage [16]. Fibrocartilage lacks the organization and mechanical properties of hyaline cartilage, making it less effective in withstanding mechanical stresses and maintaining joint function [18]. The age-related decline in cartilage repair and regeneration has significant implications for joint health. As age-related factors contribute to reduced cartilage repair and regeneration, older individuals may be at a higher risk of developing osteoarthritis or experiencing more severe joint degeneration [19].
4.2 Severity of injury
The ability of cartilage to repair itself is limited due to its avascular nature [3, 4, 20]. The extent and severity of cartilage injury indeed play a crucial role in the repair process. Minor injuries, such as small defects or superficial lesions, generally have a better chance of healing compared to more extensive injuries. For instance, a study published in the Journal of Orthopaedic Research examined the repair of small, full-thickness cartilage defects in the knee joint in rabbits. The researchers found that these small defects exhibited better healing outcomes compared to larger defects, with evidence of new cartilage formation and tissue integration [21]. In contrast, larger and deep cartilage injuries pose greater challenges to the repair process. Injuries that extend into the deeper layers of cartilage may involve damage to the underlying subchondral bone or even reach the bone itself. The lack of direct blood supply to cartilage and the limited ability of cartilage cells (chondrocytes) to proliferate and migrate to the injury site hinder the repair process. Consequently, large and deep injuries are less likely to heal spontaneously and may result in incomplete or inadequate cartilage repair. The presence of a stable and intact subchondral bone is also crucial for cartilage repair as it provides a scaffold for cell migration and tissue repair. It serves as a source of growth factors and other signaling molecules that can stimulate cartilage repair processes [20]. Clinical studies have emphasized the importance of the subchondral bone in cartilage repair. The researchers have found that when subchondral bone integrity was compromised, cartilage repair was less successful, and fibrocartilage was formed instead of hyaline cartilage [22].
4.3 Blood supply
Cartilage’s avascular nature poses a significant challenge to its healing process. Unlike well-vascularized tissues, cartilage relies on alternative mechanisms for repair, limiting its regenerative capacity. Without blood vessels, essential nutrients, oxygen, and immune cells cannot efficiently reach the injured site, hampering chondrocytes’ access to resources needed for effective healing [3, 4]. The lack of immune cells at the injury site also reduces the body’s ability to initiate the inflammatory and reparative responses necessary for tissue healing [5]. However, there are certain scenarios in which cartilage injuries may extend into the subchondral bone. The subchondral bone is well-vascularized, containing numerous blood vessels that supply nutrients and oxygen to the underlying bone and surrounding tissues. In some cases, when an injury extends into the subchondral bone, blood vessels from the bone may penetrate the injured cartilage, potentially improving the healing response [21, 22]. Clinical studies have shown that cartilage injuries that extend into the subchondral bone may exhibit improved healing potential compared to injuries limited to the cartilage layer alone [22].
4.4 Mechanical stimulation
Mechanical loading plays a crucial role in the repair and regeneration of cartilage. Cartilage is a dynamic tissue that responds to mechanical forces by adapting its structure and function. Proper mechanical stimulation through controlled joint movement and physical activity is essential for cartilage health and maintenance. Controlled and appropriate joint movement helps distribute nutrients and fluid within the cartilage, providing essential nourishment to the chondrocytes and maintaining the extracellular matrix (ECM) integrity. This mild mechanical loading stimulates chondrocyte activity and ECM turnover, promoting tissue repair and remodeling [23, 24]. In a study published in the American Journal of Sports Medicine, researchers investigated the impact of controlled dynamic compression on cartilage repair. They found that mild mechanical loading led to increased chondrocyte proliferation and synthesis of ECM components, suggesting a potential role in cartilage repair and regeneration [25]. On the other hand, excessive or abnormal mechanical loading can be detrimental to cartilage health. Overloading the joint with excessive forces can lead to cartilage degeneration and damage. High-impact activities or repetitive loading beyond the physiological capacity of the joint can cause wear and tear on the cartilage, leading to the breakdown of ECM components, thereby compromising cartilage integrity [26].
4.5 Inflammation
Inflammatory processes indeed play a critical role in cartilage repair and regeneration. Inflammation is a natural and necessary response of the body to tissue injury, including cartilage damage. It is an essential early stage in the healing process, as it helps to initiate tissue repair and recruit immune cells and growth factors to the injured site [15]. When cartilage is damaged, due to either trauma, wear and tear, or degenerative conditions, the body’s immune system responds by triggering an acute inflammatory response. This acute inflammation helps remove damaged tissue and debris, promotes the release of growth factors and cytokines, and attracts immune cells, such as macrophages and neutrophils, to the injury site [15]. Clinical evidence supports the role of acute inflammation in cartilage repair [27]. While acute inflammation is a beneficial and necessary step in cartilage repair, chronic inflammation can have detrimental effects on the healing process and cartilage health. In chronic inflammatory conditions, such as rheumatoid arthritis, release of destructive enzymes that break down the ECM components of cartilage disrupts the delicate balance between tissue breakdown and tissue repair [28] and contributes to progressive cartilage loss and joint destruction [29].
4.6 Growth factors and cytokines
Cartilage repair and regeneration are highly influenced by various growth factors and cytokines that regulate the behavior of chondrocytes. These signaling molecules play a critical role in orchestrating the complex processes involved in cartilage healing and tissue remodeling [15]. Transforming growth factor-beta (TGF-β) and insulin-like growth factor-1 (IGF-1) are two essential growth factors that stimulate chondrocyte activity and contribute to cartilage repair and regeneration. TGF-β is known for its potent effects on chondrocyte proliferation and differentiation. It promotes the synthesis of extracellular matrix (ECM) components, including collagen and proteoglycans, which are essential for cartilage structure and function. TGF-β also helps to regulate the balance between cartilage breakdown and synthesis, favoring the repair and rebuilding of damaged cartilage [30]. Insulin-like growth factor-1 (IGF-1) is another growth factor that plays a significant role in cartilage repair. It acts as a potent mitogen, stimulating chondrocyte proliferation and promoting the synthesis of ECM proteins. IGF-1 also enhances the anabolic activity of chondrocytes, leading to increased production of cartilage-specific molecules that are crucial for cartilage repair and regeneration [31]. In contrast to growth factors that promote cartilage repair, certain cytokines can have detrimental effects on cartilage health. Pro-inflammatory cytokines, such as interleukin-1 (IL-1), are key mediators of the inflammatory response and are often elevated in conditions like osteoarthritis and rheumatoid arthritis. IL-1 can promote cartilage degradation by stimulating the production of matrix-degrading enzymes, such as matrix metalloproteinases (MMPs) and aggrecanases. These enzymes can break down the ECM components of cartilage, leading to cartilage degradation and tissue damage. Additionally, IL-1 can inhibit the synthesis of ECM proteins, further compromising cartilage repair [32]. Clinical evidence has confirmed the impact of these growth factors in cartilage repair and degeneration [33].
4.7 Treatment interventions
The choice of treatment interventions can significantly impact cartilage repair and regeneration. Surgical techniques, such as microfracture, autologous chondrocyte implantation (ACI), or matrix-assisted autologous chondrocyte transplantation (MACT), aim to promote cartilage healing by stimulating the formation of fibrocartilage or transplanting healthy chondrocytes into the injured site [34]. Moreover, it is noteworthy that several treatments intended to enhance the quality of life for patients with mild to moderate arthritis might inadvertently contribute to cartilage damage. Notably, interventions such as intra-articular steroid and lignocaine injection, commonly administered to alleviate pain in individuals with arthritic knees, have been found to accelerate the deterioration of cartilage and the advancement of arthritis [35, 36]. Although these treatments may offer short-term pain relief and improved mobility, yet they also carry the risk of exacerbating cartilage breakdown over the long term, potentially impacting joint health and function.
4.8 Adjacent tissues and joint alignment
The health and stability of adjacent tissues, such as ligaments and menisci, play a crucial role in cartilage repair and overall joint health. These structures are intimately connected and work together to ensure proper joint function and stability. When adjacent tissues like ligaments and menisci are damaged or compromised, they can lead to altered joint biomechanics, causing abnormal loading and stress on the cartilage. This increased stress can contribute to cartilage degeneration and hinder the healing process of existing cartilage injuries. For example, a torn anterior cruciate ligament (ACL) in the knee can destabilize the joint, leading to abnormal movement and increased shear forces on the cartilage surfaces. This can result in cartilage damage and accelerate the progression of osteoarthritis. In contrast, a well-functioning ACL helps in maintaining joint stability and promotes more uniform distribution of forces, reducing the risk of cartilage injuries and degeneration [37, 38]. To support cartilage repair and regeneration, it is essential to address any concurrent injuries or instability in the joint. Restoring the health and stability of ligaments and menisci through appropriate rehabilitation or surgical intervention can optimize joint biomechanics and reduce excessive loading on specific areas of the cartilage. This, in turn, creates a more favorable environment for cartilage healing and helps to preserve joint function and longevity [39].
In conclusion, cartilage repair and regeneration are complex processes influenced by multiple factors. Age, severity of injury, blood supply, mechanical stimulation, inflammation, growth factors, treatment interventions, and joint alignment all play significant roles in determining the success of cartilage healing. Understanding and optimizing these factors is crucial for developing effective strategies to enhance cartilage repair, promote tissue regeneration, and potentially alleviate the impact of cartilage-related disorders.
5. Pathogenesis of osteoarthritis
Osteoarthritis (OA) is a complex and multifactorial degenerative joint disorder that affects millions of people worldwide. Articular cartilage is a crucial component of synovial joints, facilitating smooth and painless movement while providing load-bearing support. In osteoarthritis (OA), the progressive degeneration of articular cartilage is a central feature of the disease’s pathogenesis. The breakdown of this essential tissue leads to joint pain, stiffness, and functional impairment. This section explores the intricate processes involved in articular cartilage degeneration in OA, shedding light on the key factors contributing to its deterioration.
5.1 Role of mechanical stress
Mechanical stress stands as a pivotal driving force in the intricate interplay of factors contributing to articular cartilage degeneration, particularly in the context of osteoarthritis (OA). The complex nature of joint movement orchestrates a symphony of compressive and shear forces that cartilage experiences during daily activities and weight-bearing tasks. In a healthy joint, the remarkable resilience of cartilage enables it to adeptly manage and distribute these mechanical forces, maintaining the joint’s structural integrity and function [40]. However, in the complicated tapestry of osteoarthritis, this equilibrium is disrupted. The delicate balance between mechanical stress and the cartilage’s inherent capacity to regenerate and adapt becomes compromised. Excessive or aberrant mechanical loading, commonly observed in OA due to altered joint mechanics, musculoskeletal imbalances, or other contributing factors, manifests as a critical catalyst in cartilage degeneration [40, 41]. The persistent or abrupt mechanical stress leads to microdamage within the cartilage structure, creating fissures, cracks, and areas of localized stress concentration. This microdamage is a tipping point that prompts a complex series of biochemical responses within the cartilage tissue. In response to microdamage, chondrocytes initiate a complex web of signaling pathways. This includes the release of inflammatory mediators, matrix-degrading enzymes, and pro-inflammatory cytokines. The inflammatory milieu sets the stage for a heightened state of catabolism within the cartilage, promoting the degradation of matrix components like collagen and proteoglycans [41]. Over time, the sustained and cumulative impact of this cascade of events erodes the cartilage’s structural integrity. As the cartilage matrix loses its components and the chondrocytes’ regenerative capacity diminishes, the once-resilient tissue succumbs to progressive degradation and thinning. This, in turn, amplifies joint pain, restricts mobility, and exacerbates the degenerative process characteristic of osteoarthritis [42].
5.2 Proteoglycan loss
One of the early changes observed in OA is the loss of proteoglycans from the cartilage matrix. As discussed earlier, proteoglycans are essential for retaining water within the cartilage, which gives it its shock-absorbing properties. In the early stages of OA, the delicate equilibrium within the cartilage matrix becomes disrupted. The loss of proteoglycans is observed as a result of altered metabolism and biochemical changes in the cartilage tissue. This depletion of proteoglycans directly impacts the cartilage’s capacity to retain water, leading to a reduction in its shock-absorbing capabilities. As the disease progresses, the diminished water retention and subsequent loss of proteoglycans compromise the cartilage’s ability to withstand the mechanical stresses encountered during joint motion [19]. The consequence of this proteoglycan loss is twofold. First, the cartilage becomes less efficient at absorbing and distributing mechanical forces generated by activities such as walking, running, or weight-bearing. This diminished shock-absorbing capacity results in increased mechanical stress being transmitted directly to the underlying bone and joint tissues. Secondly, the altered biomechanical properties of the cartilage contribute to an environment conducive to further damage. The compromised cartilage becomes more susceptible to microdamage and fibrillation, which, in turn, accelerates the progression of OA [19, 43].
5.3 Collagen disorganization
Collagen fibers play a fundamental role in maintaining the robust structural integrity of articular cartilage. In healthy conditions, the ordered and aligned arrangement of collagen fibers within the cartilage matrix imparts resilience and durability, contributing significantly to the cartilage’s ability to function as a cushioning buffer within the joint. However, the intricate balance of collagen organization becomes disturbed in the context of osteoarthritis (OA). This degenerative joint disorder introduces a series of detrimental changes that compromise the architecture of collagen fibers. This process is referred to as collagen disorganization, and it manifests as alterations in the arrangement, alignment, and density of collagen fibers within the cartilage matrix. The consequences of collagen disorganization in OA are far-reaching [44]. As collagen fibers lose their well-ordered configuration, the tensile strength that they once provided diminishes. The once-efficient mechanical network that facilitated even distribution of forces across the cartilage surface becomes disrupted. This weakening effect leaves the cartilage more vulnerable to the mechanical stress generated during joint movement [44, 45].
Consequently, areas of increased stress concentration form on the cartilage surface, which can lead to localized microdamage and tissue degradation. Furthermore, the altered alignment of collagen fibers results in reduced ability to resist shear forces. Shear forces, which occur when opposing surfaces slide against each other, place additional stress on the cartilage. The diminished capacity of disorganized collagen to withstand these forces exacerbates the wear and tear experienced by the cartilage that hastens its deterioration. The interaction between collagen disorganization and cartilage breakdown is a vicious cycle. As the cartilage matrix loses its integrity due to collagen disorganization, chondrocytes respond with an elevated production of matrix-degrading enzymes and inflammatory mediators [45, 46]. These biochemical changes contribute to the degradation of collagen and other components within the cartilage, further accelerating tissue damage and exacerbating the OA process [15].
5.4 Chondrocyte dysfunction
Chondrocytes, assume a pivotal role in upholding the overall health and integrity of the cartilage matrix. However, in the context of osteoarthritis (OA), the functioning of chondrocytes undergoes significant alterations, which contribute to the degenerative processes associated with this condition. In OA, chondrocytes experience a shift in their synthetic activity, marked by a decline in their ability to produce essential extracellular matrix components. This diminished synthetic capacity impairs the cartilage’s ability to replenish its structural elements, thereby weakening its resilience and ability to withstand mechanical stresses. Moreover, in OA-affected joints, chondrocytes exhibit an augmented production of catabolic enzymes, particularly matrix metalloproteinases (MMPs) and aggrecanases. These enzymes act as molecular scissors, cleaving various components of the extracellular matrix, including collagen and proteoglycans. Such enzymatic breakdown of the matrix accelerates the degradation of cartilage tissue disrupting of the delicate balance between matrix synthesis and degradation within the cartilage. As the synthetic capacity wanes and catabolic enzyme activity increases, the extracellular matrix deteriorates, and the structural integrity of the cartilage progressively erodes. This compromised matrix not only reduces the cartilage’s ability to support joint movement but also diminishes its shock-absorbing properties, contributing to the overall pathology of OA [15].
5.5 Inflammatory processes
In addition to mechanical stress and structural changes, inflammation emerges as a crucial driver of articular cartilage degeneration in the context of osteoarthritis (OA). The presence of pro-inflammatory cytokines, such as interleukin-1 (IL-1) and tumor necrosis factor-alpha (TNF-α), serves as a key trigger for the initiation and propagation of inflammatory processes within the joint microenvironment. When pro-inflammatory cytokines are present, chondrocytes undergo a shift in their gene expression profiles, resulting in an elevated production of catabolic enzymes, particularly matrix metalloproteinases (MMPs) and aggrecanases. These enzymes wield the ability to cleave vital components of the extracellular matrix. The upregulation of catabolic enzymes contributes to the accelerated breakdown of matrix components, while the synthesis of matrix molecules, including collagen and proteoglycans, is compromised. This disequilibrium skews the cartilage microenvironment toward degradation, intensifying the degenerative processes at play in OA. Furthermore, the inflammatory milieu can trigger the release of pro-inflammatory mediators, amplifying the inflammatory cascade and leading to a self-perpetuating loop of cartilage breakdown [46].
5.6 Fibrillation and erosion
Notably, one of the hallmark changes observed in the course of OA is the progression of cartilage surface fibrillation [47, 48, 49, 50]. Fibrillation is characterized by the emergence of fissures and cracks on the cartilage surface, imparting a rough and irregular appearance [47]. This process of fibrillation initiates as a result of the cumulative wear and tear experienced by the cartilage during joint movement and loading [47, 51]. The constant exposure to mechanical stresses, particularly under the conditions of OA, gradually weakens the cartilage matrix and disrupts its integrity [51]. The weakened areas become prone to the formation of fissures, which gradually extend and deepen, ultimately resulting in more significant erosions [47, 51]. Over time, these erosions can progress through the layers of cartilage, eventually reaching the underlying subchondral bone [48, 52].
The consequences of cartilage fibrillation are multifaceted and impactful. The erosion of the once-smooth cartilage surface disturbs the normal mechanics of joint movement [52]. The smooth articulation between bones is compromised, leading to increased friction, uneven loading, and altered joint biomechanics [50]. This disruption in joint mechanics not only triggers pain but also exacerbates inflammation within the joint [52]. The exposed subchondral bone, lacking the protective cushioning of cartilage, becomes vulnerable to microtrauma and contributes to the inflammatory response [47, 52].
Moreover, the loss of the smooth cartilage surface compounds the mechanical stress placed on the remaining healthy cartilage [53]. The altered joint mechanics and the absence of the protective cartilage buffer force the remaining cartilage to bear an increased load, further accelerating its degeneration [47, 53]. As a result, a detrimental feedback loop ensues, where cartilage fibrillation and degradation drive joint pain, inflammation, and greater mechanical stress on the already compromised joint structures [47, 54].
5.7 Impact on synovium and joint capsule
In osteoarthritis (OA), the impact extends beyond articular cartilage degeneration to involve other joint structures, including the synovium—the lining of the joint capsule [46, 48]. The synovium plays a crucial role in joint lubrication, nutrient supply, and the regulation of inflammatory processes [46]. However, in OA, the synovium undergoes pathological changes that contribute to the disease progression [48]. One significant alteration observed in OA is synovial inflammation and thickening [55]. This inflammatory response in the synovium results in the release of pro-inflammatory cytokines, such as interleukin-1 (IL-1) and tumor necrosis factor-alpha (TNF-α), as well as various matrix-degrading enzymes. These cytokines and enzymes have detrimental effects on the joint environment fueling overall joint inflammation. The increased levels of inflammatory cytokines amplify the activity of chondrocytes that produce matrix-degrading enzymes, such as matrix metalloproteinases (MMPs), which contribute to cartilage degradation [46, 55, 56].
The interaction between synovial inflammation and articular cartilage degeneration emphasizes the systemic nature of OA and highlights the importance of considering the entire joint environment in disease management [55, 57]. Strategies aimed at mitigating OA progression need to address not only cartilage health but also the underlying inflammatory processes occurring within the synovium [46, 48, 55, 57]. By targeting synovial inflammation and its associated cytokines and enzymes, it may be possible to modulate the degenerative cascade and alleviate the overall burden of OA on joint health.
In conclusion, articular cartilage degeneration is a central feature of osteoarthritis. The complex interplay of mechanical stress, proteoglycan loss, collagen disorganization, chondrocyte dysfunction, and inflammatory processes contributes to the progressive breakdown of cartilage. Understanding these complex mechanisms is essential for developing targeted interventions to slow or halt the degenerative process and improve joint health in individuals affected by OA.
6. Subchondral bone changes and osteophyte formation
Subchondral bone plays a crucial role in supporting the articular cartilage and maintaining joint integrity. In osteoarthritis (OA), subchondral bone undergoes significant changes that contribute to the disease’s progression and symptoms. This section explores the alterations in subchondral bone and the formation of osteophytes—bone spurs—associated with OA.
6.1 Subchondral bone changes in OA
In the context of osteoarthritis (OA), subchondral bone undergoes a series of complex structural and metabolic changes that significantly impact joint health and function. These changes are intimately linked to the altered mechanical environment resulting from the degeneration of articular cartilage, and they play a crucial role in the progression of the disease. These subchondral bone changes are not only a consequence of OA but also contribute to the overall pathophysiology of the condition. Some key subchondral bone changes include:
Collectively, these subchondral bone changes in OA not only reflect the adaptation of the bone to the altered joint mechanics but also play a significant role in driving the progression of the disease. The interconnected relationship between subchondral bone and articular cartilage highlights the complexity of OA’s pathogenesis and underscores the importance of considering both tissue types when developing interventions to address this debilitating condition. The structural and metabolic changes within the subchondral bone add to the intricate web of factors that contribute to the overall deterioration of the joint in OA.
6.2 Osteophyte formation
Osteophytes, commonly referred to as bone spurs, represent a significant phenomenon within the context of osteoarthritis (OA), contributing to the complex interplay between joint degeneration and adaptive responses. These bony outgrowths develop at the margins of the affected joint and serve as a unique response of the body to the underlying pathological changes. Osteophytes play a dual role, attempting to stabilize the compromised joint while also potentially exacerbating joint symptoms and limitations [60, 61].
In summary, osteophytes are a remarkable manifestation of the body’s response to the challenges posed by OA. While they serve as an adaptive mechanism to stabilize the joint, their presence can also give rise to additional symptoms and functional limitations. The formation of osteophytes underlines the intricate relationship between joint degeneration and the body’s attempts at compensation, further emphasizing the complexity of OA’s pathophysiology.
6.3 Relationship with articular cartilage degeneration
Subchondral bone changes and osteophyte formation are closely linked with the degeneration of articular cartilage [58, 59]. The loss of cartilage results in increased mechanical stress on the subchondral bone, leading to sclerosis and cyst formation [59]. Osteophytes develop as a compensatory mechanism to stabilize the joint and redistribute forces [60, 61].
6.4 Clinical implications
The clinical implications of the interrelationship between subchondral bone changes, osteophyte formation, and articular cartilage degeneration are profound in the management of osteoarthritis (OA). These interconnected processes hold diagnostic and monitoring value, aiding healthcare professionals in accurately assessing disease progression through imaging techniques. Subchondral bone alterations and osteophyte presence can serve as indicators of disease severity, guiding treatment decisions and enabling predictions about the trajectory of OA. Treatment strategies can be refined to address both cartilage degeneration and subchondral bone abnormalities, leading to more effective interventions.
7. Emerging therapies and regenerative medicine for cartilage repair
Cartilage repair remains a significant challenge in the management of osteoarthritis (OA) and other cartilage-related conditions. Traditional treatments focus on symptom management and delaying disease progression, but they often fall short in promoting true cartilage regeneration. However, advancements in regenerative medicine offer promising approaches to stimulate cartilage repair and restoration. This section explores some of the emerging therapies and regenerative medicine techniques for cartilage repair.
7.1 Cell-based therapies
In recent years, cell-based therapies have gained prominence as potential solutions for cartilage repair. Progress in cell sourcing, scaffold design, and clinical implementation highlights the dynamic nature of this field. Despite challenges, including long-term efficacy and standardization, cell-based therapies remain at the forefront of cartilage repair strategies. Their transformative potential might hold the key to redefining the treatment landscape for cartilage-related conditions [62].
Autologous chondrocyte implantation (ACI ): ACI involves the harvest and culture of a patient’s own healthy chondrocytes. These cultured chondrocytes are then implanted into the damaged area of the cartilage, promoting tissue repair. ACI is suitable for larger cartilage defects and has shown encouraging outcomes in clinical trials [62, 63].Matrix-induced autologous chondrocyte implantation (MACI ): MACI is a variation of ACI that involves the use of a biodegradable scaffold to support the implanted chondrocytes. The scaffold enhances cell adhesion and proliferation, aiding in cartilage repair [64].Mesenchymal stem cell (MSC) therapy: MSCs are multipotent cells with the potential to differentiate into various cell types, including chondrocytes [65]. MSC therapy involves the injection of MSCs into the damaged cartilage, promoting its regeneration and repair. MSCs can be derived from various sources, such as bone marrow, adipose tissue, and umbilical cord tissue [65, 66].
7.2 Tissue engineering
Tissue engineering, a multidisciplinary field at the intersection of biology, engineering, and medicine, has emerged as a groundbreaking approach to address the limitations of conventional medical treatments and organ transplantation. In orthopedics, it is revolutionizing joint and bone repair; in cardiology, it is advancing heart tissue regeneration. Skin substitutes aid wound healing, while engineered organs strive to overcome the organ shortage crisis. Tissue engineering has emerged as a transformative solution for cartilage repair, aiming to overcome the challenges posed by the limited self-renewal capacity of articular cartilage [67].
3D bioprinting : 3D bioprinting allows the creation of custom-designed scaffolds that mimic the complex architecture of native cartilage. Chondrocytes or MSCs are seeded onto these scaffolds, which are then implanted into the defect site to promote cartilage regeneration [68, 69].Decellularized matrix-based approaches : Decellularized cartilage matrix provides an excellent biological scaffold for cartilage repair. The decellularized matrix retains the natural tissue architecture and biochemical cues necessary for cartilage regeneration. Cells, such as chondrocytes or MSCs, are then seeded onto the scaffold for implantation [69, 70].
7.3 Growth factor and cytokine therapy
Growth factors and cytokines play pivotal roles in orchestrating cellular responses, driving tissue repair, and modulating inflammatory processes. In the realm of cartilage repair, harnessing the potential of these signaling molecules has emerged as a promising strategy. Growth factors such as transforming growth factor-beta (TGF-β), fibroblast growth factors (FGFs), and insulin-like growth factors (IGFs) exert profound effects on chondrocytes and stem cells, regulating proliferation, differentiation, and extracellular matrix synthesis [71]. Direct delivery of growth factors or cytokines to the injury site aims to enhance the local environment for endogenous repair [71, 72]. Despite the promise, growth factor and cytokine therapies face challenges. Achieving optimal dosing, ensuring sustained release, and avoiding unwanted effects are hurdles. Precise spatial and temporal control of signaling activation is necessary to avoid undesirable outcomes, such as hypertrophy or fibrosis [71, 73].
Platelet-rich plasma (PRP ): PRP is extracted from the patient’s own blood and contains a high concentration of growth factors. When injected into the damaged cartilage, PRP can stimulate chondrocyte proliferation and ECM synthesis, promoting cartilage repair. Scientific studies have shown that PRP’s application can lead to improvements in cartilage repair and pain reduction. While its efficacy can vary based on factors such as the severity of the cartilage damage and the patient’s overall health, PRP offers a minimally invasive approach to stimulate the body’s natural healing mechanisms and support the restoration of cartilage tissue [74, 75, 76].Cytokine therapy: Specific cytokines, such as transforming growth factor-beta (TGF-β) and insulin-like growth factor (IGF), have shown potential in promoting chondrogenesis and cartilage regeneration. They can be delivered directly to the damaged cartilage to enhance repair processes [33].
7.4 Gene therapy
Gene therapy, a revolutionary approach to manipulate genetic information, has appeared as a promising frontier in the realm of cartilage repair [77]. Gene therapy encompasses the delivery of therapeutic genes to target cells, either by viral vectors or by nonviral methods [78]. The introduced genes can encode growth factors, cytokines, or molecular regulators that modulate cellular responses, foster chondrogenesis, and promote tissue regeneration. In osteoarthritis, genes encoding anti-inflammatory factors can mitigate inflammation-driven cartilage degradation [77, 78]. Gene therapy faces challenges, including the achievement of sustainable and localized gene expression. Off-target effects and immune responses are critical safety concerns. Balancing therapeutic efficacy with safety necessitates meticulous design and testing [79]. As research advances, gene therapy’s potential to revolutionize cartilage repair is increasingly evident, paving the way for a new era of targeted, genetically tailored regenerative treatments.
7.5 Nanotechnology
Nanotechnology has revolutionized biomaterial design. Nanostructured scaffolds, inspired by cartilage’s extracellular matrix, offer precise control over mechanical properties and cell-material interactions. These scaffolds mimic native tissue architecture, enhancing cellular adhesion, proliferation, and chondrogenic differentiation [80]. Nanoparticles serve as carriers for precise and targeted delivery of growth factors and therapeutic agents. By encapsulating these molecules, nanotechnology enables sustained release, thus enhancing their bioavailability and therapeutic efficacy. This approach minimizes off-target effects and optimizes tissue healing. Nanotechnology extends beyond repair to diagnostics and monitoring. Nanosensors and imaging agents offer real-time insights into tissue health, enabling personalized treatment strategies and timely interventions [80, 81]. Nanotechnology’s immense potential is accompanied with challenges. Ensuring biocompatibility, long-term safety, and scalable manufacturing is a critical concern. Additionally, ethical and regulatory considerations arise as nanotechnology bridges the divide between medicine and material science [81].
7.6 Exosome therapy
Exosomes are carriers of bioactive molecules, including proteins, nucleic acids, and lipids, functioning as messengers between cells. Their unique ability to modulate recipient cell behavior makes them intriguing candidates for therapeutic interventions [82]. In cartilage repair, exosomes play roles in anti-inflammatory responses, extracellular matrix remodeling, and promotion of chondrogenic differentiation. Exosome therapy involves isolating and purifying exosomes from various sources, including mesenchymal stem cells (MSCs) and chondrocytes. Techniques like ultracentrifugation and precipitation are commonly employed, ensuring the enrichment of exosomal cargo. Direct exosome administration promotes chondroprotection, reducing inflammation and inhibiting cartilage degradation [83]. Encapsulation of exosomes in biomaterial scaffolds augments their release profile, enhancing their therapeutic effects [82, 83]. Exosome therapy circumvents challenges associated with cell-based therapies, such as immune responses and potential tumorigenicity. However, standardized isolation methods, cargo loading, and dosage optimization pose challenges [82].
While these emerging therapies show great promise for cartilage repair, further research is needed to optimize their effectiveness and safety. Additionally, research trials are being conducted to evaluate the long-term outcomes and potential side effects of these novel approaches. As research continues, regenerative medicine holds incredible potential in revolutionizing the treatment landscape for cartilage repair and improving the quality of life for persons with cartilage-related conditions.
8. Challenges and potential solutions in developing cartilage-targeted treatments
Developing effective and targeted treatments for cartilage-related conditions, such as osteoarthritis (OA), presents various challenges due to the intricate nature of cartilage tissue and its unique features. Overcoming these challenges is crucial to improving patient outcomes and achieving successful cartilage repair and regeneration. Here are various fundamental challenges and potential solutions in formulating cartilage-targeted treatments:
8.1 Limited blood supply and innervation
Challenge : Cartilage is avascular and lacks nerve fibers, making it difficult to deliver drugs and therapeutic agents directly to the affected area.Solution : Developing targeted drug delivery systems, such as nanoparticles or hydrogels, can help deliver medications precisely to the cartilage site. Intra-articular injections and tissue engineering approaches can also be used for localized delivery [84, 85, 86].
8.2 Low cellular activity
Challenge : Chondrocytes, the cells within cartilage, have low metabolic activity, limiting their capacity of self-repair and regeneration.Solution : Stimulating chondrocyte activity through growth factors, gene therapy, or cell-based therapies can enhance cartilage repair and regeneration [85].
8.3 Complex cartilage structure
Challenge : Cartilage has a unique extracellular matrix (ECM) composition, making it challenging to replicatein vitro for tissue engineering approaches.Solution : Decellularized matrix-based approaches that retain the natural ECM structure, combined with cell-based therapies, can enhance cartilage repair [85].
8.4 Inflammatory microenvironment
8.5 Disease heterogeneity
Challenge: OA is a heterogeneous condition with varying degrees of cartilage damage and different underlying mechanisms.Solution: Personalized medicine approaches, such as identifying specific biomarkers and disease phenotypes, can help tailor treatments to individual patients [87].
8.6 Integration with native cartilage
Challenge: Ensuring that the repaired or regenerated cartilage integrates seamlessly with the native cartilage is crucial for long-term success.Solution: Optimization of tissue engineering approaches, such as scaffold design and cell source selection, can enhance integration and biomechanical properties of the repaired tissue [88].
8.7 Long-term efficacy and safety
Challenge: Ensuring that cartilage-targeted treatments have durable efficacy and safety profiles is critical for their clinical use.Solution: Conducting robust preclinical and clinical research trials to estimate the long-term outcomes and safety of these treatments is essential [89].
8.8 High costs and accessibility
Challenge: Some advanced cartilage-targeted treatments may be costly and not readily accessible to all patients.Solution: Continued research and development may lead to more cost-effective and scalable treatments, making them more widely available [90].
In conclusion, developing effective cartilage-targeted treatments requires addressing the unique challenges presented by cartilage tissue. By leveraging advancements in drug delivery, tissue engineering, regenerative medicine, and personalized medicine, potential solutions can be found to improve cartilage repair, regeneration, and overall patient outcomes in cartilage-related conditions like osteoarthritis.
9. Call for continued research and collaboration in the field of cartilage and osteoarthritis
The study of cartilage and its related conditions, particularly osteoarthritis (OA), is of utmost importance in the field of orthopedics and musculoskeletal research. As we strive to improve patient outcomes and find effective treatments for cartilage-related disorders, a call for continued research and collaboration becomes imperative. By fostering a collaborative and multidisciplinary approach, we can unlock new insights, address current challenges, and develop innovative therapies for cartilage repair, regeneration, and osteoarthritis management.
Advancing basic science knowledge : A deeper understanding of cartilage biology, molecular signaling pathways, and the intricate interactions between inflammatory mediators and cartilage cells is essential. Basic science research will pave the way for the advancement of targeted therapies and interventions.Exploring regenerative medicine : Regenerative medicine offers great promise in the realm of cartilage repair and regeneration. Continued research in stem cell biology, tissue engineering, and gene therapy will enable us to harness the regenerative potential of the body for cartilage healing.Investigating biomarkers and disease phenotypes: Identifying reliable biomarkers for cartilage degeneration and osteoarthritis progression can aid in early diagnosis, prognostication, and monitoring treatment response. Additionally, studying disease phenotypes will help tailor personalized medicine approaches for improved patient care.
Enhancing drug delivery systems: Developing effective drug delivery systems for targeted cartilage treatment remains a challenge. Collaborative efforts between pharmacologists, engineers, and clinicians can lead to innovative solutions that deliver therapeutic agents precisely to the affected cartilage site.Conducting longitudinal studies: Longitudinal studies tracking patients over extended periods are crucial to understanding the natural progression of osteoarthritis and evaluating the long-term efficacy and safety of different treatments.
10. Conclusion
The journey through the intricate web of osteoarthritis (OA) pathogenesis has illuminated the multifaceted interplay of cellular, molecular, and biomechanical factors that orchestrate the degeneration of articular cartilage. OA, once considered a wear-and-tear phenomenon, has revealed itself as a dynamic disease driven by a plethora of intricate mechanisms.
The avascular and aneural nature of cartilage poses a challenge in delivering targeted therapies directly to the affected area. However, as highlighted in this chapter, innovative solutions are emerging. Nanoparticles, hydrogels, and tissue engineering approaches offer avenues for precise drug delivery, offering hope for localized treatment strategies that could potentially alter the trajectory of OA progression. Moreover, insights into the inflammatory microenvironment and cellular signaling have paved the way for novel interventions that target inflammation, reshaping the local milieu to support repair rather than degradation.
As our understanding of OA deepens, the significance of individualized approaches becomes paramount. Disease heterogeneity stresses the need for personalized medicine, harnessing the power of biomarkers and phenotypic characterizations to tailor treatments to patients’ specific needs. Furthermore, the imperative to seamlessly integrate repaired or regenerated cartilage with native tissue highlights the importance of scaffold design and cell selection in tissue engineering strategies, ensuring long-term success.
Yet challenges remain from ensuring long-term efficacy and safety to addressing the accessibility of advanced treatments. With each challenge, however, comes opportunity. Continued research and clinical trials hold the promise of refining and validating interventions, making them more accessible, affordable, and effective for a broader spectrum of patients.
In the grand narrative of cartilage degeneration and osteoarthritis pathogenesis, this chapter is but a stepping stone. As the field continues to evolve, forging connections between cellular mechanisms, biomaterials, and clinical practice, the journey to mitigate the impact of osteoarthritis takes on new dimensions. By understanding the intricate web of factors that contribute to OA, we will be empowered to envision a future where its progression is not inevitable, but rather a challenge that can be met with innovation, compassion, and scientific rigor.
Acknowledgments
I would like to express my deepest gratitude to my beloved wife “Samia Khurshid,” whose unwavering support, encouragement, and understanding have been the cornerstone of my journey in bringing this chapter to fruition. Her patience and constant belief in my abilities have been a wellspring of inspiration. Her presence has provided the calm amidst the storms of research and writing, and her love has been the guiding light that illuminated my path. This work would not have been possible without her love, sacrifices, and unwavering belief in my aspirations.
Dr. Saif ur Rehman
Conflict of interest
The authors declare no conflict of interest.
References
- 1.
Pirozzi KM. Histophysiology of fibrocartilage. Clinics in Podiatric Medicine and Surgery. 2022; 39 (3):363-370. DOI: 10.1016/j.cpm.2022.02.002 - 2.
Gahunia HK, Pritzker KPH. Structure and function of articular cartilage. In: Gahunia HK, Gross AE, Pritzker KPH, Babyn PS, Murnaghan L, editors. Articular Cartilage of the Knee Health, Disease and Therapy. Springer Nature; 2020. pp. 36-104 - 3.
Sophia Fox AJ, Bedi A, Rodeo SA. The basic science of articular cartilage: Structure, composition, and function. Sports Health. 2009; 1 (6):461-468. DOI: 10.1177/1941738109350438 - 4.
Żylińska B, Sobczyńska-Rak A, Lisiecka U, Stodolak-Zych E, Jarosz Ł, Szponder T. Structure and pathologies of articular cartilage. In Vivo. 2021; 35 (3):1355-1363. DOI: 10.21873/invivo.12388 - 5.
Vincent TL, McClurg O, Troeberg L. The extracellular matrix of articular cartilage controls the bioavailability of pericellular matrix-bound growth factors to drive tissue homeostasis and repair. International Journal of Molecular Sciences. 2022; 23 (11):6003. DOI: 10.3390/ijms23116003 - 6.
Verzijl N, DeGroot J, Thorpe SR, Bank RA, Shaw JN, Lyons TJ, et al. Effect of collagen turnover on the accumulation of advanced glycation end products. The Journal of Biological Chemistry. 2000; 275 :39027-39031 - 7.
Mostakhdemin M, Nand A, Ramezani M. Articular and artificial cartilage, characteristics, properties and testing approaches—A review. Polymers (Basel). 2021; 13 (12):2000. DOI: 10.3390/polym13122000 - 8.
Iozzo RV, Schaefer L. Proteoglycan form and function: A comprehensive nomenclature of proteoglycans. Matrix Biology. 2015; 42 :11-55. DOI: 10.1016/j.matbio.2015.02.003 - 9.
Bhosale AM, Richardson JB. Articular cartilage: Structure, injuries and review of management. British Medical Bulletin. 2008; 87 :77-95. DOI: 10.1093/bmb/ldn025 - 10.
Marczyński W. Pathology of articular cartilage – Dynamics of changes, prevention. Wiadomości Lekarskie. 2007; 60 (1):53-59 - 11.
Youn I, Choi JB, Cao L, Setton LA, Guilak F. Zonal variations in the three-dimensional morphology of the chondron measured in situ using confocal microscopy. Osteoarthritis and Cartilage. 2006; 14 (9):889-897. DOI: 10.1016/j.joca.2006.02.017 - 12.
Pearle AD, Warren RF, Rodeo SA. Basic science of articular cartilage and osteoarthritis. Clinics in Sports Medicine. 2005; 24 (1):1-12. DOI: 10.1016/j.csm.2004.08.007 - 13.
Decker RS, Koyama E, Pacifici M. Articular cartilage: Structural and developmental intricacies and questions. Current Osteoporosis Reports. 2015; 13 (6):407-414. DOI: 10.1007/s11914-015-0290-z - 14.
Eschweiler J, Horn N, Rath B, Betsch M, Baroncini A, Tingart M, et al. The biomechanics of cartilage—An overview. Life (Basel). 2021; 11 (4):302. DOI: 10.3390/life11040302 - 15.
Goldring MB, Goldring SR. Articular cartilage and subchondral bone in the pathogenesis of osteoarthritis. Annals of the New York Academy of Sciences. 2010; 1192 :230-237. DOI: 10.1111/j.1749-6632.2009.05240.x - 16.
Lotz M, Loeser RF. Effects of aging on articular cartilage homeostasis. Bone. 2012; 51 (2):241-248. DOI: 10.1016/j.bone.2012.03.023 - 17.
Brittberg M, Peterson L, Sjögren-Jansson E, Tallheden T, Lindahl A. Articular cartilage engineering with autologous chondrocyte transplantation. A review of recent developments. The Journal of Bone and Joint Surgery. American Volume. 2003; 85-A (Suppl-3):109-115. DOI: 10.2106/00004623-200300003-00017 - 18.
Armiento AR, Alini M, Stoddart MJ. Articular fibrocartilage—Why does hyaline cartilage fail to repair? Advanced Drug Delivery Reviews. 2019; 146 :289-305. DOI: 10.1016/j.addr.2018.12.015 - 19.
Loeser RF, Goldring SR, Scanzello CR, Goldring MB. Osteoarthritis: A disease of the joint as an organ. Arthritis and Rheumatism. 2012; 64 (6):1697-1707. DOI: 10.1002/art.34453 - 20.
Masson AO, Krawetz RJ. Understanding cartilage protection in OA and injury: A spectrum of possibilities. BMC Musculoskeletal Disorders. 2020; 21 (1):432. DOI: 10.1186/s12891-020-03363-6 - 21.
Gross AE, Shasha N, Aubin P. Long-term followup of the use of fresh osteochondral allografts for posttraumatic knee defects. Clinical Orthopaedics and Related Research. 2005; 435 :79-87 - 22.
Madry H, Orth P, Cucchiarini M. Role of the subchondral bone in articular cartilage degeneration and repair. The Journal of the American Academy of Orthopaedic Surgeons. 2016; 24 (4):e45-e46. DOI: 10.5435/JAAOS-D-16-00096 - 23.
Salter RB, Simmonds DF, Malcolm BW, Rumble EJ, MacMichael D, Clements ND. The biological effect of continuous passive motion on the healing of full-thickness defects in articular cartilage. An experimental investigation in the rabbit. The Journal of Bone and Joint Surgery. American Volume. 1980; 62 (8):1232-1251 - 24.
Fahy N, Alini M, Stoddart MJ. Mechanical stimulation of mesenchymal stem cells: Implications for cartilage tissue engineering. Journal of Orthopaedic Research. 2018; 36 (1):52-63. DOI: 10.1002/jor.23670 - 25.
Iseki T, Rothrauff BB, Kihara S, Sasaki H, Yoshiya S, Fu FH, et al. Dynamic compressive loading improves cartilage repair in an in vitro model of microfracture: Comparison of 2 mechanical loading regimens on simulated microfracture based on fibrin gel scaffolds encapsulating connective tissue progenitor cells. The American Journal of Sports Medicine. 2019; 47 (9):2188-2199. DOI: 10.1177/0363546519855645 - 26.
Sanchez-Adams J, Leddy HA, McNulty AL, O’Conor CJ, Guilak F. The mechanobiology of articular cartilage: Bearing the burden of osteoarthritis. Current Rheumatology Reports. 2014; 16 (10):451. DOI: 10.1007/s11926-014-0451-6 - 27.
Lohmander LS, Englund PM, Dahl LL, Roos EM. The long-term consequence of anterior cruciate ligament and meniscus injuries: Osteoarthritis. The American Journal of Sports Medicine. 2007; 35 (10):1756-1769. DOI: 10.1177/0363546507307396 - 28.
Guo Q , Wang Y, Xu D, Nossent J, Pavlos NJ, Xu J. Rheumatoid arthritis: Pathological mechanisms and modern pharmacologic therapies. Bone Research. 2018; 6 :15. DOI: 10.1038/s41413-018-0016-9 - 29.
Coutant F, Miossec P. Evolving concepts of the pathogenesis of rheumatoid arthritis with focus on the early and late stages. Current Opinion in Rheumatology. 2020; 32 (1):57-63. DOI: 10.1097/BOR.0000000000000664 - 30.
Chawla S, Mainardi A, Majumder N, Dönges L, Kumar B, Occhetta P, et al. Chondrocyte hypertrophy in osteoarthritis: Mechanistic studies and models for the identification of new therapeutic strategies. Cell. 2022; 11 (24):4034. DOI: 10.3390/cells11244034 - 31.
Goldring MB. The role of the chondrocyte in osteoarthritis. Arthritis and Rheumatism. 2000; 43 (9):1916-1926. DOI: 10.1002/1529-0131(200009)43:9<1916::AID-ANR2>3.0.CO;2-I - 32.
Molnar V, Matišić V, Kodvanj I, Bjelica R, Jeleč Ž, Hudetz D, et al. Cytokines and chemokines involved in osteoarthritis pathogenesis. International Journal of Molecular Sciences. 2021; 22 (17):9208. DOI: 10.3390/ijms22179208 - 33.
Wen C, Xu L, Xu X, Wang D, Liang Y, Duan L. Insulin-like growth factor-1 in articular cartilage repair for osteoarthritis treatment. Arthritis Research & Therapy. 2021; 23 (1):277. DOI: 10.1186/s13075-021-02662-0 - 34.
Migliorini F, Eschweiler J, Schenker H, Baroncini A, Tingart M, Maffulli N. Surgical management of focal chondral defects of the knee: A Bayesian network meta-analysis. Journal of Orthopaedic Surgery and Research. 2021; 16 (1):543. DOI: 10.1186/s13018-021-02684-z - 35.
Rehman SU, Afzal T, Iqbal S, Zain-Ul-Abidin M, Aslam F. Comparison of disease progression in patients with osteoarthritis of knee treated with versus without intraarticular injection of corticosteroids. Pakistan Journal of Medical & Health Sciences. 2022; 16 (2):255-257. DOI: 10.53350/pjmhs22162255 - 36.
Zeng C, Lane NE, Hunter DJ, Wei J, Choi HK, McAlindon TE, et al. Intra-articular corticosteroids and the risk of knee osteoarthritis progression: Results from the osteoarthritis initiative. Osteoarthritis and Cartilage. 2019; 27 (6):855-862. DOI: 10.1016/j.joca.2019.01.007 - 37.
Arner JW, Irvine JN, Zheng L, Gale T, Thorhauer E, Hankins M, et al. The effects of anterior cruciate ligament deficiency on the meniscus and articular cartilage: A novel dynamic in vitro pilot study. Orthopaedic Journal of Sports Medicine. 2016; 4 (4):2325967116639895. DOI: 10.1177/2325967116639895 - 38.
Sutter EG, Liu B, Utturkar GM, Widmyer MR, Spritzer CE, Cutcliffe HC, et al. Effects of anterior cruciate ligament deficiency on tibiofemoral cartilage thickness and strains in response to hopping. The American Journal of Sports Medicine. 2019; 47 (1):96-103. DOI: 10.1177/0363546518802225 - 39.
Deckers C, Stephan P, Wever KE, Hooijmans CR, Hannink G. The protective effect of anterior cruciate ligament reconstruction on articular cartilage: A systematic review of animal studies. Osteoarthritis and Cartilage. 2019; 27 (2):219-229. DOI: 10.1016/j.joca.2018.10.001 - 40.
Anderson DD, Chubinskaya S, Guilak F, Martin JA, Oegema TR, Olson SA, et al. Post-traumatic osteoarthritis: Improved understanding and opportunities for early intervention. Journal of Orthopaedic Research. 2011; 29 (6):802-809. DOI: 10.1002/jor.21359 - 41.
Peffers M, Liu X, Clegg P. Transcriptomic signatures in cartilage ageing. Arthritis Research & Therapy. 2013; 15 (4):R98. DOI: 10.1186/ar4278 - 42.
Guilak F, Fermor B, Keefe FJ, Kraus VB, Olson SA, Pisetsky DS, et al. The role of biomechanics and inflammation in cartilage injury and repair. Clinical Orthopaedics and Related Research. 2004; 423 :17-26. DOI: 10.1097/01.blo.0000131233.83640.91 - 43.
Roughley PJ, Mort JS. The role of aggrecan in normal and osteoarthritic cartilage. Journal of Experimental Orthopaedics. 2014; 1 (1):8. DOI: 10.1186/s40634-014-0008-7 - 44.
Eyre D. Collagen of articular cartilage. Arthritis Research. 2002; 4 (1):30-35. DOI: 10.1186/ar380 - 45.
Chen H, Tan XN, Hu S, Liu RQ , Peng LH, Li YM, et al. Molecular mechanisms of chondrocyte proliferation and differentiation. Frontiers in Cell and Development Biology. 2021; 9 :664168. DOI: 10.3389/fcell.2021.664168 - 46.
Goldring MB, Otero M. Inflammation in osteoarthritis. Current Opinion in Rheumatology. 2011; 23 (5):471-478. DOI: 10.1097/BOR.0b013e328349c2b1 - 47.
Primorac D, Molnar V, Rod E, Jeleč Ž, Čukelj F, Matišić V, et al. Knee osteoarthritis: A review of pathogenesis and state-of-the-art non-operative therapeutic considerations. Genes (Basel). 2020; 11 (8):854. DOI: 10.3390/genes11080854 - 48.
Goldring MB, Goldring SR. Osteoarthritis. Journal of Cellular Physiology. 2007; 213 (3):626-634. DOI: 10.1002/jcp.21258 - 49.
Burr DB. Anatomy and physiology of the mineralized tissues: Role in the pathogenesis of osteoarthrosis. Osteoarthritis Cartilage. 2004; 12 (Suppl. A):S20-S30. DOI: 10.1016/j.joca.2003.09.016 - 50.
Buckwalter JA, Mankin HJ. Articular cartilage: Degeneration and osteoarthritis, repair, regeneration, and transplantation. Instructional Course Lectures. 1998; 47 :487-504 - 51.
Aigner T, Söder S, Gebhard PM, McAlinden A, Haag J. Mechanisms of disease: Role of chondrocytes in the pathogenesis of osteoarthritis--structure, chaos and senescence. Nature Clinical Practice. Rheumatology. 2007; 3 (7):391-399. DOI: 10.1038/ncprheum0534 - 52.
Lories RJ, Luyten FP. The bone-cartilage unit in osteoarthritis. Nature Reviews Rheumatology. 2011; 7 (1):43-49. DOI: 10.1038/nrrheum.2010.197 - 53.
Kuyinu EL, Narayanan G, Nair LS, Laurencin CT. Animal models of osteoarthritis: Classification, update, and measurement of outcomes. Journal of Orthopaedic Surgery and Research. 2016; 11 :19. DOI: 10.1186/s13018-016-0346-5 - 54.
Madry H, Luyten FP, Facchini A. Biological aspects of early osteoarthritis. Knee Surgery, Sports Traumatology, Arthroscopy. 2012; 20 (3):407-422. DOI: 10.1007/s00167-011-1705-8 - 55.
Scanzello CR, Goldring SR. The role of synovitis in osteoarthritis pathogenesis. Bone. 2012; 51 (2):249-257. DOI: 10.1016/j.bone.2012.02.012 - 56.
Pearle AD, Scanzello CR, George S, Mandl LA, DiCarlo EF, Peterson M, et al. Elevated high-sensitivity C-reactive protein levels are associated with local inflammatory findings in patients with osteoarthritis. Osteoarthritis and Cartilage. 2007; 15 (5):516-523. DOI: 10.1016/j.joca.2006.10.010 - 57.
Roach HI, Aigner T, Kouri JB. Chondroptosis: A variant of apoptotic cell death in chondrocytes? Apoptosis. 2004; 9 (3):265-277. DOI: 10.1023/b:appt.0000025803.17498.26 - 58.
Goldring SR, Goldring MB. Bone and cartilage in osteoarthritis: Is what’s best for one good or bad for the other? Arthritis Research & Therapy. 2010; 12 (5):143. DOI: 10.1186/ar3135 - 59.
Burr DB, Gallant MA. Bone remodelling in osteoarthritis. Nature Reviews Rheumatology. 2012; 8 (11):665-673. DOI: 10.1038/nrrheum.2012.130 - 60.
Martel-Pelletier J, Barr AJ, Cicuttini FM, Conaghan PG, Cooper C, Goldring MB, et al. Osteoarthritis. Nature Reviews. Disease Primers. 2016; 2 :16072. DOI: 10.1038/nrdp.2016.72 - 61.
Neogi T. The epidemiology and impact of pain in osteoarthritis. Osteoarthritis and Cartilage. 2013; 21 (9):1145-1153. DOI: 10.1016/j.joca.2013.03.018 - 62.
Jeuken RM, van Hugten PPW, Roth AK, Timur UT, Boymans TAEJ, van Rhijn LW, et al. A systematic review of focal cartilage defect treatments in middle-aged versus younger patients. Orthopaedic Journal of Sports Medicine. 2021; 9 (10):23259671211031244. DOI: 10.1177/23259671211031244 - 63.
Niemeyer P, Laute V, Zinser W, Becher C, Diehl P, Kolombe T, et al. Clinical outcome and success rates of ACI for cartilage defects of the patella: A subgroup analysis from a controlled randomized clinical phase II trial (CODIS study). Archives of Orthopaedic and Trauma Surgery. 2020; 140 (6):717-725. DOI: 10.1007/s00402-019-03264-x - 64.
Brittberg M, Recker D, Ilgenfritz J, Saris DBF, SUMMIT Extension Study Group. Matrix-applied characterized autologous cultured chondrocytes versus microfracture: Five-year follow-up of a prospective randomized trial. The American Journal of Sports Medicine. 2018; 46 (6):1343-1351. DOI: 10.1177/0363546518756976 - 65.
Le H, Xu W, Zhuang X, Chang F, Wang Y, Ding J. Mesenchymal stem cells for cartilage regeneration. Journal of Tissue Engineering. 2020; 11 :2041731420943839. DOI: 10.1177/2041731420943839 - 66.
Arshi A, Petrigliano FA, Williams RJ, Jones KJ. Stem cell treatment for knee articular cartilage defects and osteoarthritis. Current Reviews in Musculoskeletal Medicine. 2020; 13 (1):20-27. DOI: 10.1007/s12178-020-09598-z - 67.
Esdaille CJ, Washington KS, Laurencin CT. Regenerative engineering: A review of recent advances and future directions. Regenerative Medicine. 2021; 16 (5):495-512. DOI: 10.2217/rme-2021-0016 - 68.
Francis SL, Di Bella C, Wallace GG, Choong PFM. Cartilage tissue engineering using stem cells and bioprinting technology-barriers to clinical translation. Frontiers in Surgery. 2018; 5 :70. DOI: 10.3389/fsurg.2018.00070 - 69.
Sahranavard M, Sarkari S, Safavi S, Ghorbani F. Three-dimensional bio-printing of decellularized extracellular matrix-based bio-inks for cartilage regeneration: A systematic review. Biomaterials Translational. 2022; 3 (2):105-115. DOI: 10.12336/biomatertransl.2022.02.004 - 70.
Sun Y, Yan L, Chen S, Pei M. Functionality of decellularized matrix in cartilage regeneration: A comparison of tissue versus cell sources. Acta Biomaterialia. 2018; 74 :56-73. DOI: 10.1016/j.actbio.2018.04.048 - 71.
Goldring MB. Chondrogenesis, chondrocyte differentiation, and articular cartilage metabolism in health and osteoarthritis. Therapeutic Advances in Musculoskeletal Disease. 2012; 4 (4):269-285. DOI: 10.1177/1759720X12448454 - 72.
Kapoor M, Martel-Pelletier J, Lajeunesse D, Pelletier JP, Fahmi H. Role of proinflammatory cytokines in the pathophysiology of osteoarthritis. Nature Reviews Rheumatology. 2011; 7 (1):33-42. DOI: 10.1038/nrrheum.2010.196 - 73.
Bessa PC, Casal M, Reis RL. Bone morphogenetic proteins in tissue engineering: The road from laboratory to clinic, part II (BMP delivery). Journal of Tissue Engineering and Regenerative Medicine. 2008; 2 (2):81-96. DOI: 10.1002/term.74 - 74.
Filardo G, Previtali D, Napoli F, Candrian C, Zaffagnini S, Grassi A. PRP injections for the treatment of knee osteoarthritis: A meta-analysis of randomized controlled trials. Cartilage. 2021; 13 (Suppl. 1):364-375. DOI: 10.1177/1947603520931170 - 75.
Moretti L, Maccagnano G, Coviello M, Cassano GD, Franchini A, Laneve A, et al. Platelet rich plasma injections for knee osteoarthritis treatment: A prospective clinical study. Journal of Clinical Medicine. 2022; 11 (9):2640. DOI: 10.3390/jcm11092640 - 76.
Shahid A, Malik A, Bukhari A, Shaikh A, Rutherford J, Barkatali B. Do platelet-rich plasma injections for knee osteoarthritis work? Cureus. 2023; 15 (2):e34533. DOI: 10.7759/cureus.34533 - 77.
Li X, Shen L, Deng Z, Huang Z. New treatment for osteoarthritis: Gene therapy. Precision Clinical Medicine. 2023; 6 (2):pbad014. DOI: 10.1093/pcmedi/pbad014 - 78.
Uzieliene I, Kalvaityte U, Bernotiene E, Mobasheri A. Non-viral gene therapy for osteoarthritis. Frontiers in Bioengineering and Biotechnology. 2021; 8 :618399. DOI: 10.3389/fbioe.2020.618399 - 79.
Watson-Levings RS, Palmer GD, Levings PP, Dacanay EA, Evans CH, Ghivizzani SC. Gene therapy in orthopaedics: Progress and challenges in pre-clinical development and translation. Frontiers in Bioengineering and Biotechnology. 2022; 10 :901317. DOI: 10.3389/fbioe.2022.901317 - 80.
Qiao K, Xu L, Tang J, Wang Q , Lim KS, Hooper G, et al. The advances in nanomedicine for bone and cartilage repair. Journal of Nanobiotechnology. 2022; 20 (1):141. DOI: 10.1186/s12951-022-01342-8 - 81.
Eftekhari A, Maleki Dizaj S, Sharifi S, Salatin S, Rahbar Saadat Y, Zununi Vahed S, et al. The use of nanomaterials in tissue engineering for cartilage regeneration; current approaches and future perspectives. International Journal of Molecular Sciences. 2020; 21 (2):536. DOI: 10.3390/ijms21020536 - 82.
Shao J, Zaro J, Shen Y. Advances in exosome-based drug delivery and tumor targeting: From tissue distribution to intracellular fate. International Journal of Nanomedicine. 2020; 15 :9355-9371. DOI: 10.2147/IJN.S281890 - 83.
Chen LY, Kao TW, Chen CC, Niaz N, Lee HL, Chen YH, et al. Frontier review of the molecular mechanisms and current approaches of stem cell-derived exosomes. Cell. 2023; 12 (7):1018. DOI: 10.3390/cells12071018 - 84.
Nguyen LH, Annabi N, Nikkhah M, Bae H, Binan L, Park S, et al. Vascularized bone tissue engineering: Approaches for potential improvement. Tissue Engineering. Part B, Reviews. 2012; 18 (5):363-382. DOI: 10.1089/ten.TEB.2012.0012 - 85.
Pati F, Song TH, Rijal G, Jang J, Kim SW, Cho DW. Ornamenting 3D printed scaffolds with cell-laid extracellular matrix for bone tissue regeneration. Biomaterials. 2015; 37 :230-241. DOI: 10.1016/j.biomaterials.2014.10.012 - 86.
Spiller KL, Maher SA, Lowman AM. Hydrogels for the repair of articular cartilage defects. Tissue Engineering. Part B, Reviews. 2011; 17 (4):281-299. DOI: 10.1089/ten.TEB.2011.0077 - 87.
Kraus VB, Blanco FJ, Englund M, Henrotin Y, Lohmander LS, Losina E, et al. OARSI clinical trials recommendations: Soluble biomarker assessments in clinical trials in osteoarthritis. Osteoarthritis and Cartilage. 2015; 23 (5):686-697. DOI: 10.1016/j.joca.2015.03.002 - 88.
Benders KE, van Weeren PR, Badylak SF, Saris DB, Dhert WJ, Malda J. Extracellular matrix scaffolds for cartilage and bone regeneration. Trends in Biotechnology. 2013; 31 (3):169-176. DOI: 10.1016/j.tibtech.2012.12.004 - 89.
Butoescu N, Jordan O, Doelker E. Intra-articular drug delivery systems for the treatment of rheumatic diseases: A review of the factors influencing their performance. European Journal of Pharmaceutics and Biopharmaceutics. 2009; 73 (2):205-218. DOI: 10.1016/j.ejpb.2009.06.009 - 90.
Jiang N, Yang P, Liu S, Li H, Wu L, Shi X, et al. Satisfaction of patients and physicians with treatments for rheumatoid arthritis: A population-based survey in China. Patient Preference and Adherence. 2020; 14 :1037-1047. DOI: 10.2147/PPA.S232578