 Open access peer-reviewed chapter
Open access peer-reviewed chapter
Abstract
The unusual role of the gallbladder in storing bile, which is crucial for digestive processes and the health of the gastrointestinal tract, sets it apart from other hollow organs. Under the influence of various factors in the gallbladder, where the processes of condensation and reconstitution of bile fluid take place, problems may arise in the cycle and pathologies may appear. Understanding the anatomy of the gallbladder, extrahepatic biliary tract, and surrounding organs is crucial for the diagnosis and treatment of various clinical conditions. The typical and variant anatomy of the gallbladder and the structures surrounding it will be covered in this section.
Keywords
- gallbladder
- extrahepatic biliary tract
- embryological development
- anatomy
- variation
1. Introduction
Bile is a secretion of water, bile salts, bilirubin, cholesterol, and several electrolytes secreted from the liver and stored in the gallbladder, which plays an important role in the digestion and absorption of fat in the small intestine. Bile is continuously produced in the liver and transported through the bile ducts. It is concentrated while stored in the gallbladder and excreted into the digestive tract with food intake. During these processes, pathological conditions (gallstones, etc.) can occur due to metabolic and other factors (genetic, infection, etc.). Although the ultimate solution is cholecystectomy, removal of the gallbladder, the localization and anatomical variations of the gallbladder, and related formations may cause iatrogenic injuries. This chapter discusses the anatomy and variations of the gallbladder and bile ducts.
2. Development of gallbladder
In humans, the extrahepatic bile ducts and liver develop from the hepatic diverticulum or liver bud, an endodermal outgrowth of the foregut, around the eighteenth day after fertilization (toward the beginning of the fourth week). The gallbladder also develops from the caudal part (pars cystica) of the hepatic foregut diverticulum. The gallbladder becomes recognizable on the twenty-ninth day after fertilization and the cystic duct around the thirty-fourth day [1]. The gallbladder has a tubular shape until the eleventh week of pregnancy, after which it expands and becomes saccular. The fetal gallbladder is intrahepatic, embedded in the liver fossa [2] until the seventeenth gestational week. It then protrudes under the inferior surface of the liver [3].
The extrahepatic bile ducts develop between the third and eighth embryonic weeks with the extension of the caudal part of the hepatic diverticulum. The extrahepatic parts of the hepatic duct and the right and left hepatic ducts develop from the cranial part of the hepatic diverticulum (pars hepatica). The proximal parts of the hilar ducts originate from the intrahepatic ductal plates. At the beginning of the fifth gestational week, the hepatobiliary anatomical structures (gallbladder, cystic duct, hepatic ducts, common bile duct, and ventral pancreas) are in the ventral mesentery of the duodenum. At the end of the fifth week, with the rotation of the duodenum to the right side, the developing common bile duct is displaced to its new position in the dorsal part of the duodenum. The lower part of the common bile duct and the ventral pancreatic primordium enter the dorsal mesentery and join the dorsal pancreatic primordium. They become secondary retroperitoneal, located anterior to the retroperitoneal organs. The fusion fascia surrounding these structures contributes to the formation of the anterior layer of Gerota’s fascia.
In the sixth gestational week, the developing extrahepatic biliary tract is organized. By the seventh week, the lumen reaches the cystic duct, but the gallbladder is still a cluster of cells (until the twelfth week). Abnormalities during the reorganization of the extrahepatic biliary tract can affect the development of the bile ducts and gallbladder, resulting in various types of atresia. In addition, two or more lumens may be present in the duct, and duplications may occur due to their inability to merge. In the ninth week, the muscular part of the gallbladder develops from the mesenchymal cells surrounding the epithelial primordium.
An outward growth from the common bile duct forms the ventral pancreas. The connection of the common bile duct with the anterior intestine occurs at the major duodenal papilla in the second part of the duodenum. Here, the terminal part of the common bile duct and the terminal part of the pancreatic duct come together to form a short duct.
Other associated anomalies include annular pancreas, malrotation, duodenal atresia, imperforate anus, portal and inferior vena cava abnormalities, polysplenia, congenital heart disease, and urinary tract anomalies. It has been reported that reovirus type-3 infections may lead to possible biliary atresia.
Agenesis of the gallbladder is extremely rare. It may be associated with normal or atresia biliary tract. One in six patients with extrahepatic biliary atresia has gallbladder agenesis. The rapid growth of the liver in the second gestational month is important to understand anomalies related to the localization of the gallbladder. Positional anomalies of the gallbladder are intrahepatic, retrohepatic, left-sided, and ptotic (hanging).
The retrohepatic gallbladder is thought to be associated with the abnormal migration of the gallbladder-cystic duct bud posteriorly.
Left-sided gallbladder occurs rarely and can be found on the undersurface of the left lobe of the liver or to the left of the falciform ligament. It may have a cystic duct with a normal position, or it may angulate sharply to the left.
In the twelfth week, the gallbladder becomes hollow by vacuolization. Errors in vacuolization can lead to septation within the gallbladder. The presence of a complete septation is referred to as gallbladder duplication. Duplication can occur at various levels. When the fundus and corpus are involved starting from the neck, it is called external duplication. In a mild type, a duplication may occur that is not visible externally but is completely separated internally by a longitudinal septum. Partial duplications can also occur due to gallbladder-cystic duct bifurcation. In this case, duplications of the cystic duct or gallbladder (as two separate sacs) may occur.
Embryologic changes in the terminal part of the gallbladder-cystic duct bud can cause deformities such as Phrygian cap, hourglass gallbladder, Hartmann’s pouch, and diverticula. Some of these may be acquired rather than congenital (e.g., Hartmann’s pouch may occur as a result of dilatation of the infundibulum due to chronic obstruction).
The gallbladder, because of its solid structure, is not sonographically distinguishable until the second trimester of pregnancy. Around the twentieth gestational week, it can be identified in 65% of fetuses [4].
3. Anatomy of gallbladder
The gallbladder is a flask- or pear-shaped diverticulum connected to the extrahepatic bile duct by a duct called the ductus cysticus. It has three parts: fundus, corpus, and neck (Figure 1). It is involved in the storage, concentration, and rehydration of bile from hepatocytes and its ejection into the digestive tract. This function is regulated by the parasympathetic nervous system and hormones, especially cholecystokinin.

Figure 1.
Anatomy and location of the gallbladder [
In the living organism, it is gray-blue in color and is located in a depression (fossa vesicae biliaris) on the visceral surface of the right lobe of the liver (segments IV and V) and is fixed to it by the visceral peritoneum. This fossa is located at the caudal border of the interlobar fissure, an embryologic structure separating the right and left hepatic lobes. Within this fissure (fissure of Gans, Rouviere’s sulcus, or incisura hepatis dextra) is the middle hepatic vein. It is a useful anatomic landmark in hepatic resection and laparoscopic cholecystectomy (the cystic duct and artery are located anterosuperior to the sulcus, whereas the common bile duct is posteroinferior) [5]. In the posterosuperior part of the fossa is the porta hepatis through which the hepatic artery, portal vein, and common bile duct pass. The peritoneum surrounds these structures and is called the hepatoduodenal ligament (free edge of the lesser omentum, Figure 2). A fold extending from the hepatoduodenal ligament around the gallbladder is called the cholecystoduodenal ligament.

Figure 2.
The hepatoduodenal ligament and its contents [
In an adult, the gallbladder is 7 to 10 cm long and has a volume of 25 (resting/empty) to 50 ml [7]. The relationship of the gallbladder to the liver varies and has been classified into seven groups by [8]. Outside of these groups, the gallbladder may very rarely be surrounded by the parenchyma of the liver (intrahepatic gallbladder) [9]. In cases that allow the gallbladder to move away from the liver, more caution should be exercised as there is a risk of gallbladder torsion [10, 11].
In most of the population (approximately 75% according to Tihan [8]), the gallbladder has a fundus that contacts the anterior abdominal wall in the transpyloric plane, a corpus located in the fossa, and a neck located most medially. The junction of the fundus and corpus is the widest part of the gallbladder and narrows toward the neck. The most rapidly narrowing part is called the infundibulum. The collum vesicae biliaris is close to the porta hepatis and is attached to the liver by a short and thin peritoneal attachment (mesentery). This peritoneal attachment usually contains the cystic artery. The mesenteric attachment shortens as it moves from the neck to the body and covers the gallbladder fossa. The mucosa on the inner wall of the neck contains oblique folds, which are continuous with the spiral mucosal folds in the cystic duct [12]. The neck of the gallbladder expands laterally to form the body. The expansion site is associated with gallstone disease and is called “Hartmann’s pouch.” The neck of the gallbladder is located in front of the descending part, the second part of the duodenum.
The bulbous fundus of the gallbladder is located at the lateral end of the corpus and usually crosses the inferior margin of the liver and contacts the parietal peritoneum on the abdominal wall behind the ninth costal cartilage, at the lateral edge of the right rectus abdominis. This area is examined in the clinical examination of gallbladder enlargement. The gallbladder is posteroinferiorly adjacent to the duodenum as well as the transverse colon and sometimes the inferior vena cava.
The gallbladder is usually supplied by the cystic artery branching from the right hepatic artery. Venous drainage occurs
The gallbladder is histologically composed of three layers. The outermost serous layer is formed by the peritoneum and is usually lost where the gallbladder contacts the liver and is replaced by a connective tissue. Microscopic bile ductules (radicles, ducts of Luschka) may extend from the intrahepatic bile ducts into this connective tissue. The innermost mucosal layer consists of columnar epithelium and has both absorption and mucus-secretory functions. The inner surface of the gallbladder is surrounded by thin folds that become prominent during contraction. The mucosa protrudes into the outer layers in sacs, forming the Rokitansky-Aschoff sinuses. These can be associated with disease and are found in most adults. The mucosa of the gallbladder is continuous with the mucosa of the cystic duct. The mucosa is lifted by spiral folds (Heister valves). The intervening muscular layer comprises circular, longitudinal, and obliquely oriented muscle fibers and surrounding connective tissue. The muscular layer also continues in the wall of the cystic duct but not in the wall of the bile ducts.
The size and shape of the gallbladder is variable. The fundus may be elongated and highly mobile. Rarely, the fundus curves over the corpus and is called a Phrygian cap, which may be misinterpreted on ultrasonographic examination as the presence of a septum. Other variations of the gallbladder include agenesis, duplication, the presence of double cystic duct, internal septation, and ectopic localization [13]. Boyden [14] and Harlaftis et al. classified gallbladder variations as Type 1 and Type 2, which were further subdivided (Figure 3) [15, 16]

Figure 3.
Variations of the gallbladder.
Although variations of the gallbladder are rare, they are very important in patients requiring surgery for gallbladder diseases or gallstones [17, 18].
4. Intrahepatic biliary tract
The left half of the liver has segmental ducts with a relatively constant pattern, and one segmental duct can drain more than one segment. The left hepatic duct is formed by the fusion of segment II and segment III ducts and is located posterior or to the left of the umbilical portion of the left portal vein. Bile drainage of segment IV varies but is accomplished by a single duct that opens into the left hepatic duct. The right hepatic duct is formed by the union of the right anterior (medial) and posterior (lateral) sectoral ducts. The right anterior (medial) sectoral duct drains segments V and VIII, and the right posterior (lateral) sectoral duct drains segments VI and VII. The right posterior sectoral duct usually bends on the posterior aspect of the right anterior duct and converges medially. This is called Hjortsö’s crook and is an important condition to be considered during liver resection.
The right hepatic duct and its branches show more variations than the left ductal system [19]. They are divided into six main groups. Left intrahepatic ductal variations are mostly related to the drainage pattern of segment IV. This segmental duct usually drains into the left hepatic duct but can sometimes open into the segment II or even III duct, the right anterior sectoral duct, or even the common hepatic duct [20].
A bile duct from segment V of the liver, described by Luschka, may pass through the fossa of the gallbladder and open into the right hepatic duct or its anterior sectoral branch, the common hepatic duct, or, rarely, the cystic duct. These ducts, classified as Luschka’s ducts, occur in 30% of the population in various sizes, whereas ducts 1 to 2 mm in diameter have a prevalence of only 5% [21]. Damage to these variational ducts during cholecystectomy can cause postoperative complications such as bile leakage.
5. Extrahepatic biliary tract
After leaving the liver, the right and left hepatic ducts merge at the right edge of the porta hepatis to form the common hepatic duct (Figure 4). The extrahepatic right duct is short (0.5 to 2.0 cm in adults) and vertically oriented. The extrahepatic left duct is longer (1.5 to 3.5 cm) and more horizontal, lying on the inferior margin of segment IV. Access to the extrahepatic segment of the left hepatic duct is important during surgical biliary bypass for benign hilar bile duct strictures.

Figure 4.
Porta hepatis and its content [
After leaving the liver, the right and left hepatic ducts merge 2.5 to 25 mm from the liver parenchyma to form the common hepatic duct. The left hepatic duct has a longer extrahepatic course than the right hepatic duct (17 and 9 mm, respectively). In some cases, the junction may remain within the liver parenchyma as the liver enlarges. The length of the common hepatic duct can vary considerably (15 to 35 mm). Sometimes, the cystic duct may open at the junction of the right and left hepatic ducts to form the common bile duct (Figure 5B). Three types of cystohepatic junction have been classified as angular, parallel, and spiral.

Figure 5.
Formation of the common hepatic duct. A: normal case; B: cystohepatic junction with aberrant common hepatic duct formation.
In adults, the common hepatic duct is 3 cm long and is obliquely joined to the cystic duct on the right side and is called the common bile duct. The common hepatic duct is located to the right of the hepatic artery and anterior to the portal vein within the hepatoduodenal ligament. In adults, the normal common hepatic duct lumen diameter is less than 5 mm in ultrasound measurements.
The cystic duct drains the gallbladder into the common bile duct (Figure 6). It has a length of 2 to 4 cm and a lumen diameter of 2 to 3 mm in adults [12]. With its tortuous structure, it passes through the posterior and medial part of the neck of the gallbladder, merges with the common hepatic duct, and forms the common bile duct. The junction of the cystic duct with the common hepatic duct varies. In most people, it opens into the middle third of the total length of the common hepatic and common bile ducts, but it may open more distally or more proximally (into the common hepatic duct or the right hepatic duct). It usually opens to the medial surface of the common hepatic duct but may also join medially, anteriorly, or posteriorly.

Figure 6.
Extrahepatic biliary tract anatomy [
The cystic duct usually forms an oblique angle at its junction with the common hepatic duct, but sometimes it may make a spiral turn around it, or it may descend parallel to it for a while and merge within the hepatoduodenal ligament.
The cystic duct may rarely be double or absent or may take an abnormal hepatic duct from segment V of the liver. These variations are very important for surgical interventions such as cholecystectomy, and in cases where the anatomy is not clear enough, it is important to detect them with a cholangiogram before the operation. The cystic duct should be occluded away from the common bile duct during cholecystectomy without damaging the common bile duct.
The triangular area formed by the cystic duct, the common hepatic duct, and the lower surface of the liver is called the hepatobiliary triangle (Figure 7, blue triangle). This triangle is often confused with Calot’s triangle (Figure 7, green triangle), an isosceles triangle with the common hepatic duct forming the base and the cystic artery and cystic duct forming the sides [24]. The hepatobiliary triangle is bridged by a two-layered peritoneum that forms the short and diverse mesentery of the cystic duct. Between the two sheets of the peritoneum are various amounts of adipose tissue, lymph vessels, cystic lymph node, autonomic nerves, and the cystic artery, which usually extends from the right hepatic artery to the gallbladder. Sometimes, an accessory bile duct can also be seen here. A good understanding of the anatomy of the biliary or arterial structures involved in the structure of the triangle is crucial to preventing damage to the common hepatic duct, common bile duct, or right hepatic artery during cholecystectomy [25, 26].
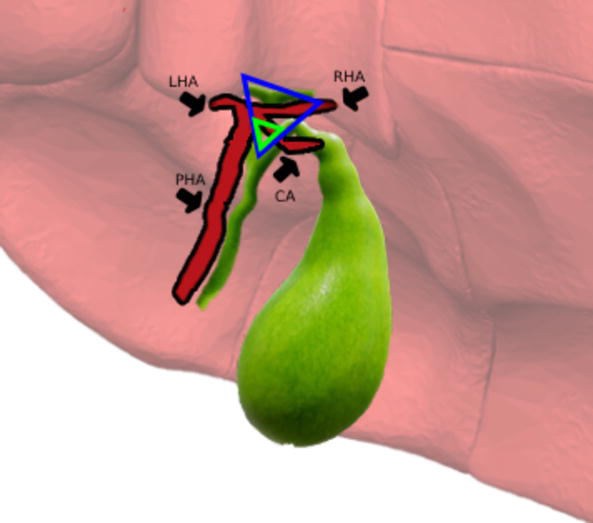
Figure 7.
Hepatobiliary (blue) and Calot’s (green) triangles. LHA, left hepatic artery; RHA, right hepatic artery; PHA, proper hepatic artery; CA, cystic artery.
The common bile duct is formed close to the porta hepatis by the union of the cystic duct and the common hepatic duct. In adults, the duct is usually 6 to 8 cm in length, with a luminal diameter of less than 7 mm measured by ultrasound [27]. The diameter changes with age (3.6 mm under 60 years, 4 mm over 80 years). The common bile duct can be divided into three segments: supraduodenal, retroduodenal, and pancreatic segments. The supraduodenal segment descends posteriorly and slightly to the left, anterior to the epiploic foramen and inferior vena cava, to the right of the hepatic artery on the free right margin of the lesser omentum, and to the right-anterior to the portal vein. This segment is the most surgically accessible part of the common bile duct. The retroduodenal segment is located behind the first part of the duodenum to the right of the gastroduodenal artery. The pancreatic segment lies in a groove behind the head of the pancreas. Here, it is embedded in the gland to varying degrees. It runs in front of the right renal vein 2 cm from the second part of the duodenum. The posterior superior pancreaticoduodenal branch of the gastroduodenal artery descends anterior to the retroduodenal portion of the common bile duct. When it crosses the upper edge of the pancreas, the artery winds around the common bile duct.
The common bile duct runs down and medially behind the head of the pancreas, approaching the medial end of the main pancreatic duct. Together, the two ducts enter the wall of the second part of the duodenum and form a short duct, 2 to 10 mm long. This duct opens into the medial wall of the second part of the duodenum through the major duodenal papilla after an expansion called the hepatopancreatic ampulla (of Vater). Clinically, this region is called the pancreaticobiliary junction. Sometimes, the two ducts may merge before entering the duodenum to form a long common duct, but sometimes, they resist the duodenum separated from each other by a septum (Figure 8).

Figure 8.
Common bile duct and duodenum [
In the terminal 5 to 10 mm of the common bile duct and main pancreatic duct, the mucosa has plicae with a complex circular organization. Their distribution and orientation are known to prevent the reflux of duodenal contents into the ducts and cause difficulty in the cannulation of the major duodenal papilla during endoscopic retrograde cholangiopancreatography (ERCP).
The common bile duct (bile duct sphincter), the main pancreatic duct (pancreatic duct sphincter), and the hepatopancreatic ampulla (sphincter of Oddi) are surrounded by complexly organized circular smooth muscle fibers. This sphincter muscle complex is 15 to 20 mm in length and is located within the duodenal wall but is anatomically and developmentally separate from the surrounding duodenal muscle fibers. The sphincter complex regulates the passage of pancreatic secretions and bile into the duodenum and prevents the reflux of duodenal contents into the ductal system. Cholecystokinin (CKK) inhibits the sphincter and causes contraction of the gallbladder. During ERCP, it may be necessary to divide the upper part of the sphincter of Oddi (sphincterotomy) to access the common bile duct. The pancreaticobiliary connection can be affected by various congenital and acquired diseases. An abnormal junction of the bile and pancreatic ducts can lead to congenital bile duct dilatation, recurrent pancreatitis, and/or gallbladder cancers. Gallstone obstructions and peri-ampullary tumors are pathologies that can occur later.
The innervation of the gallbladder and extrahepatic biliary tract is mediated by branches from the hepatic plexus. Parasympathetic fibers from the vagus nerve as well as CKK cause contractions of the gallbladder. Postganglionic sympathetic fibers from the coeliac and superior mesenteric ganglia cause inhibition of the smooth muscles of the gallbladder. On the other hand, these sympathetic fibers receive the pain sensation of the gallbladder and carry it to the seventh and ninth (T7–T9) spinal cord segments
Lymphatic drainage of the gallbladder and cystic duct occurs first to the cystic node above the cystic duct in the hepatobiliary triangle, then to the lymph nodes at the free edge of the lesser omentum, and then to the coeliac lymph nodes along the common hepatic artery. Some lymph also drains around the common bile duct to the superior pancreaticoduodenal node, which is connected to the para-aortic nodes, and to the superior mesenteric lymph nodes. Lymph from the part of the gallbladder adjacent to the liver passes into the intrahepatic lymph vessels [29].
6. Conclusion
Changing lifestyles and diets have led to an increase in clinical conditions related to the gallbladder and biliary tract. Since gallstone-related disorders affect the main pancreatic duct as well as the bile ducts, cholecystectomy gains importance as a permanent and effective solution. A good knowledge of the anatomy of the gallbladder and bile ducts is essential for a successful and uncomplicated surgery. In addition to basic knowledge of the anatomy of the biliary tract, intraoperative evaluation prevents possible injuries [30, 31]. The advantages of laparoscopic cholecystectomy such as minimal intervention and rapid recovery are limited by the complications that may be caused by anatomic variations. Therefore, both surgical intervention and the development of new treatment modalities can only be possible by transferring the current knowledge in the most accurate and broadest way.
References
- 1.
Roskams T, Desmet V. Embryology of extra- and intrahepatic bile ducts, the ductal plate. Anatomical Record (Hoboken, N.J.: 2007). 2008; 291 (6):628-635. DOI: 10.1002/ar.20710 - 2.
Wang BJ, Kim JH, Yu HC, Rodríguez-Vázquez JF, Murakami G, Cho BH. Fetal intrahepatic gallbladder and topographical anatomy of the liver hilar region and hepatocystic triangle. Clinical Anatomy (New York, NY). 2012; 25 (5):619-627. DOI: 10.1002/ca.21288 - 3.
Haffajee MR. The fetal gallbladder: morphology and morphometry by microdissection. Surgical and Radiologic Anatomy. 2000; 22 (5-6):261-270. DOI: 10.1007/s00276-000-0261-6 - 4.
Meilstrup JW. Imaging Atlas of the Normal Gallbladder and Its Variants. CRC Press; 2018 - 5.
Dahmane R, Morjane A, Starc A. Anatomy and surgical relevance of Rouviere’s sulcus. ScientificWorldJournal. 2013; 2013 :254287. DOI: 10.1155/2013/ 254287 - 6.
Remesz O. Hepatoduodenal ligament. [Online]. Accessed date: https://upload.wikimedia.org/wikipedia/commons/4/44/Hepatoduodenal_ligament_EN.svg - 7.
Di Ciaula A, Wang DQ-H, Portincasa P. Gallbladder and gastric motility in obese newborns, pre-adolescents and adults. Journal of Gastroenterology and Hepatology. 2012; 27 (8):1298-1305. DOI: 10.1111/j.1440-1746.2012.07149.x - 8.
Tihan D et al. The effect of morphometric and anatomic relationship of gallbladder to the liver on standard laparoscopic cholecystectomies and proposal of a new anatomical classification. European Review for Medical and Pharmacological Sciences. 2016; 20 (8):1458-1466 - 9.
Guiteau JJ, Fisher M, Cotton RT, Goss JA. Intrahepatic gallbladder. Journal of the American College of Surgeons. 2009; 209, 5 :s. 672. DOI: 10.1016/j.jamcollsurg.2009.03.027 - 10.
Ashaolu JO, Ukwenya VO, Adenowo TK. Cystoduodenal ligament as an abnormal fold and the accompanying anatomical and clinical implications. Surgical and Radiologic Anatomy. 2011; 33 (2):171-174. DOI: 10.1007/s00276-010-0736-z - 11.
Gupta V, Singh V, Sewkani A, Purohit D, Varshney R, Varshney S. Torsion of gall bladder, a rare entity: a case report and review article. Cases Journal. 2009; 2 :193. DOI: 10.1186/1757-1626-2-193 - 12.
Dasgupta D, Stringer MD. Cystic duct and Heister’s ‘valves’. Clinical Anatomy (New York, NY). 2005; 18 (2):81-87. DOI: 10.1002/ca.20118 - 13.
Faure JP, Doucet C, Scepi M, Rigoard P, Carretier M, Richer JP. Abnormalities of the gallbladder, clinical effects. Surgical and Radiologic Anatomy. 2008; 30 (4):285-290. DOI: 10.1007/s00276-008-0332-7 - 14.
Boyden EA. The accessory gallbladder an embryological and comparative study of aberrant biliary vesicles occurring in man and the domestic mammals. American Journal of Anatomy. 1926; 38 (2):177-231 - 15.
Harlaftis N, Gray SW, Skandalakis JE. Multiple gallbladders. Surgery, Gynecology & Obstetrics. 1977; 145 (6):928-934 - 16.
Botsford A, McKay K, Hartery A, Hapgood C. MRCP imaging of duplicate gallbladder: A case report and review of the literature. Surgical and Radiologic Anatomy. 2015; 37 (5):425-429. DOI: 10.1007/s00276-015-1456-1 - 17.
Castorina S, Scilletta R, Domergue J. Gallbladder agenesis: Laparoscopic views of a significant diagnostic challenge. Surgical and Radiologic Anatomy. 2014; 36 (6):619-620. DOI: 10.1007/s00276-014-1263-0 - 18.
Singh B, Ramsaroop L, Allopi L, Moodley J, Satyapal KS. Duplicate gallbladder: An unusual case report. Surgical and Radiologic Anatomy. 2006; 28 (6):654-657. DOI: 10.1007/s00276-006-0139-3 - 19.
Cucchetti A et al. Anatomic variations of intrahepatic bile ducts in a European series and meta-analysis of the literature. Journal of Gastrointestinal Surgery. 2011; 15 (4):623-630. DOI: 10.1007/s11605-011-1447-4 - 20.
Chaib E, Kanas AF, Galvão FHF, D’Albuquerque LAC. Bile duct confluence: Anatomic variations and its classification. Surgical and Radiologic Anatomy. 2014; 36 (2):105-109. DOI: 10.1007/s00276-013-1157-6 - 21.
Ko K et al. A study of the subvesical bile duct (duct of Luschka) in resected liver specimens. World Journal of Surgery. 2006; 30 (7):1316-1320. DOI: 10.1007/s00268-005-0469-z - 22.
Sobotta J. An anatomical illustration from the 1906 edition of Sobotta’s Atlas and Text-book of Human Anatomy with English terminology - 23.
LukesAnatomy. Gross Gallbladder anatomy and local ducts. [Online]. Accessed date: https://upload.wikimedia.org/wikipedia/commons/6/61/GallbladderAnatomy.png - 24.
Stringer MD. Gallbladder and Extrahepatic Bile Ducts. In: Tubbs RS, Shoja MM, Loukas M, editors. Bergman’s Comprehensive Encyclopedia of Human Anatomic Variation. 2016. DOI: 10.1002/9781118430309.ch107 - 25.
Suzuki M, Akaishi S, Rikiyama T, Naitoh T, Rahman MM, Matsuno S. Laparoscopic cholecystectomy, Calot’s triangle, and variations in cystic arterial supply. Surgical Endoscopy. 2000; 14 (2):141-144. DOI: 10.1007/s004649900086 - 26.
Talpur KAH, Laghari AA, Yousfani SA, Malik AM, Memon AI, Khan SA. Anatomical variations and congenital anomalies of extra hepatic biliary system encountered during laparoscopic cholecystectomy. JPMA. Journal of the Pakistan Medical Association. 2010; 60 (2):89-93 - 27.
Perret RS, Sloop GD, Borne JA. Common bile duct measurements in an elderly population. Journal of Ultrasound in Medicine. 2000; 19 (11):727-730; quiz 731. DOI: 10.7863/jum.2000.19.11.727 - 28.
Cypressvine, PancreasColor.jpg. [Online]. Accessed date: https://commons.wikimedia.org/wiki/File:PancreasColor.jpg - 29.
Sato T, Ito M, Sakamoto H. Pictorial dissection review of the lymphatic pathways from the gallbladder to the abdominal para-aortic lymph nodes and their relationships to the surrounding structures. Surgical and Radiologic Anatomy. 2013; 35 (7):615-621. DOI: 10.1007/s00276-013-1088-2 - 30.
Buddingh KT, Nieuwenhuijs VB, van Buuren L, Hulscher JBF, de Jong JS, van Dam GM. Intraoperative assessment of biliary anatomy for prevention of bile duct injury: A review of current and future patient safety interventions. Surgical Endoscopy. 2011; 25 (8):2449-2461. DOI: 10.1007/s00464-011-1639-8 - 31.
Brunt LM et al. Safe Cholecystectomy Multi-society Practice Guideline and State of the Art Consensus Conference on Prevention of Bile Duct Injury During Cholecystectomy. Annals of Surgery. 2020; 272 (1):3-23. DOI: 10.1097/SLA.0000000000003791