Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
This is a retrospective study that has had the objective to establish if there are any risk factors for developing Hashimoto thyroiditis (HT) in a type 2 diabetes (T2DM) population and also to determine if the prevalence of HT is higher in the population of T2DM, comparing with the European population. In the beginning, 5064 patients were evaluated and after that three groups were analysed, one of patients having only type 2 diabetes, one having only Hashimoto thyroiditis and one in which the patients had both of this diseases; each group had 50 patients in it. All patients were analysed using the same clinical and biological parameters. Results showed an increased prevalence of Hashimoto thyroiditis among the type 2 diabetes population, three times higher than in the European population (789.89/105 per year versus 259.12/105 per year). The second part of the study established that female gender, insulin resistance, overweight, high value of glycaemia, hepatic steatosis, cardiac ischemic disease, hypothyroidism, smoking and alcohol intake are risk factors for the onset of HT in T2DM population.
National Institute of Pneumoftiziology “Marius Nasta” Bucharest, Romania
Octavian Alexe
“Dunarea de Jos” University Galati, Romania
Corina Risca (Popazu)
“Dunarea de Jos” University Galati, Romania
Dan Mircea Cheta
“Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania
Cristiana Voineag
Emergency County Clinical Hospital Braila, Romania
*Address all correspondence to: oana_andreea@yahoo.com
1. Introduction
Our goal with this research was to demonstrate if the association between type 2 diabetes mellitus (T2DM) and Hashimoto’s autoimmune thyroiditis (HT) is a real or just it was just a random coincidence. In our practice, we noticed an increased prevalence of chronic lymphocytic thyroiditis in patients with T2DM. After searching the literature, we noticed that this association had not been studied and only type 1 diabetes mellitus (T1DM) and HT were known to associate, both of which are autoimmune diseases and the association between them was logical.
We designed an observational, retrospective study on patients from “Sanamed Hospital” clinic in Bucharest; this clinic mainly treats diabetes patients, both type 1 and type 2 diabetes.
Using the data from the patient database, we analysed firstly the incidence of the association of the two diseases, comparing it with the European dates, and we proved that our incidences were significantly and statistically higher, showing that our initial hypothesis was right, and there is an association between T2DM and HT.
The second phase of our research was focused on clinical and paraclinical elements that can explain the abovementioned association, risk factors involved and finding the population at risk for developing both this diseases.
We used the data collected from the database of the clinic “Sanamed Hospital” based in Bucharest during 01 January 2016–2031 December 2018 to identify the possible correlations in patients with T2DM and thyroid impairment.
First, we evaluated 5064 patients with T2DM that were examined during that period of time; this patients were used in an initial study that was called Study 1 Determining the incidence of chronic autoimmune lymphocytic thyroiditis in the population of patients diagnosed with T2DM.
Second, we designed another study—Study 2: Clinicometabolic and therapeutic features in patients with T2DM and HT, in which we evaluated 150 patients divided into three groups: 50 patients had only T2DM, 50 patients had only HT and 50 patients had both T2DM and HT (referred to as Lot 1, Lot 2 and Lot 3).
The database and processing of own data was performed in Microsoft Office Excel 2010 and SPSS.
2.1 Purpose of the research
2.1.1 Main objectives
to determine the incidence of HT in a population with T2DM,
to determine the existence of independent predictors of the association, if any, between the two pathologies.
As secondary objectives we proposed:
to determine if insulin resistance (IR) is in any way involved in this association by determining by surrogate indices of IR;
to determine if the presence or absence of obesity is correlated with the association of T2DM and HT;
to determine if the presence or absence of dyslipidaemia is correlated with the association of T2DM and HT;
to determine if the presence or absence of metabolic syndrome is correlated with the association of T2DM and HT;
to determine if the existence of clinicometabolic features of micro- and macrovascular complications of T2DM in patients are a risk factor for developing HT.
2.1.2 Criteria for inclusion in study 1
age over 16 years,
previous diagnosis of T2DM established according to the criteria listed below:
previous diagnosis of HT established according to the criteria listed below for patients in Group 2,
previous diagnosis of HT established during the follow-up period of the study established according to the criteria listed below for patients in Group 3,
patients who have agreed to the processing of their personal data by signing the informed consent form of the clinic in which they were investigated.
2.1.3 Exclusion criteria in study 1
diagnosis of T1DM,
presence of anti-GAD antibodies in patients’ serum.
2.1.4 Inclusion criteria in study 2
age over 16 years,
previous diagnosis of T2DM established according to the criteria listed below,
previous diagnosis of HT established according to the criteria listed below for patients in Group 2,
diagnosis established during the follow-up period of the HT study established according to the criteria listed below for patients in Group 3,
patients who agreed to the processing of their personal data by signing the informed consent form of the clinic where they were investigated.
presence of anti-TPO antibodies in the serum of patients in Group 1,
pregnant or breastfeeding patients,
patients with severe psychiatric pathologies that prevent from discerning,
patients with physical disabilities or severe cognitive impairment that may affect their mobility and therefore their ability to move for further investigations necessary to complete the database in this study,
patients who have refused to sign the clinic’s informed consent to the processing of personal data,
patients who refused to continue further investigations necessary to collect data for this study.
Patients included in the study were additionally analysed for the following clinical and paraclinical parameters: total cholesterol, triglycerides, serum creatinine, estimated glomerular filtration rate (eGFR), uric acid, oxalacetic transaminase (TGO), pyruvic transaminase (TGP), height, weight, abdominal circumference, body mass index (BMI) and blood pressure. These parameters were used to identify possible correlations and possible risk factors.
Patients were also clinically assessed; the presence or absence of the following conditions was sought: obesity, dyslipidaemia, atrial hypertension, chronic micro- and/or macrovascular complications of DM, ischemic heart disease, congestive heart failure, metabolic syndrome, hepatic steatosis, hyperuricemia/gout, cataracts, glaucoma, depression and pre-existing thyroid pathology, each was defined according to international diagnostic criteria.
We calculated surrogate markers for the determination of IR. We used the value of Triglycerides and Glucose Index (TyG Index), Visceral Adiposity Index (VAI), Lipid Accumulation Product (LAP) and Triglycerides Ratio on HDL Cholesterol (TG/HDL). We also calculated variants of TyG, more exactly TyG in relation to BMI (TyG-BMI) and in relation to abdominal circumference (TyG-WC) [1, 2].
2.1.6 Research hypotheses
In this regard, we formulated the following hypotheses:
Patients diagnosed with T2DM have a higher risk of developing HT compared to the general population;
Patients with a certain degree of high risk for T2DM and HT will have a high degree of association with medical laboratory values in relation to the associated thyroid disfunction and metabolic syndrome.
2.2 Study 1: determination of the incidence of chronic autoimmune lymphocytic thyroiditis in a population of patients diagnosed with type 2 diabetes mellitus
2.2.1 Introduction
Based on a finding from our daily practice with patients, we aimed to assess the incidence of HT in patients with T2DM. Among patients diagnosed with T2DM, we observed a large number of new cases of HT. Previously in the literature, only the association between T1DM and HT was described in terms of the underlying autoimmune pathophysiological mechanism of the two pathologies; thus, our findings were either mere coincidences or there is a link between T2DM and HT.
2.2.2 Objectives of study 1
In the first phase of our research, we aimed to assess the incidence of HT in patients with T2DM, to determine what we had previously found, namely an increased proportion of thyroiditis in patients with T2DM, was confirmed or was just a chance finding without clinical significance.
2.2.3 Purpose
The main purpose of this first study was to determine the incidence of HT in the population with T2DM from “Sanamed Hospital” clinic in Bucharest, through a retrospective observational study for over 3 years, between 1 January 2016 and 31 December 2018.
2.2.4 Materials and methods
A total number of 5064 patients with T2DM were evaluated using patient details from “Sanamed Hospital” clinic, which were collected over 3 years, between 1 January 2016 and 31 December 2018. Subsequently, the incidence per 100,000 inhabitants was calculated and the data were compared with those found in the European population; at the national level such data are not available, so the comparison with the Romanian population was not possible.
2.2.5 Results of study 1
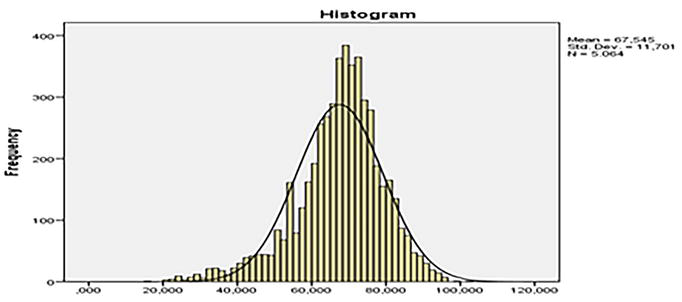
Of the 5064 subjects analysed in the initial phase of our study, 2383 were men, representing 47.05%, and 2681 (52.94%) were female. We can say that the initial sample was divided into almost two equal parts which did not create a research bias (Figure 1).
Figure 1.
Average age in the initial lot.
Regarding the mean age in the initial group, we had 67.545 ± 11.701 years, with an older age for the patients evaluated in the Diabetes Mellitus section (68.508 ± 10.653 years) compared to those evaluated in the Endocrinology ward (57.058 ± 16.432 years). This was natural, given that the average age at the onset of patients with T2DM is older.
During the three-year period of the study, the incidence of HT in the group of 5064 patients diagnosed with T2DM was 789.89/105 per year, with an incidence of 230.80/105 per year among diabetic men and an incidence of 1286.83/105 per year among women. Comparing European wide reports of HT incidence in the general European population [3] (259.12/105 per year, 85.36/105 per year in men and 419.72/105 per year in women), there is a highly significant difference between the incidence in the general population and the incidence among patients diagnosed with T2DM (Table 1). This confirms the original hypothesis of the study. Remarkably, a patient with T2DM has a threefold higher risk of developing chronic lymphocytic thyroiditis (HT), and also, female patients with T2DM have an almost sixfold higher prevalence of Hashimoto’s thyroiditis than men diagnosed with T2DM.
Total subjects (n = 5064)
Men (n = 2383)
Women (n = 2681)
Total incidence per year 105
Incidence in men per year 105
Incidence in women per year 105
With HT acquired after the diagnosis of T2DM in the present study
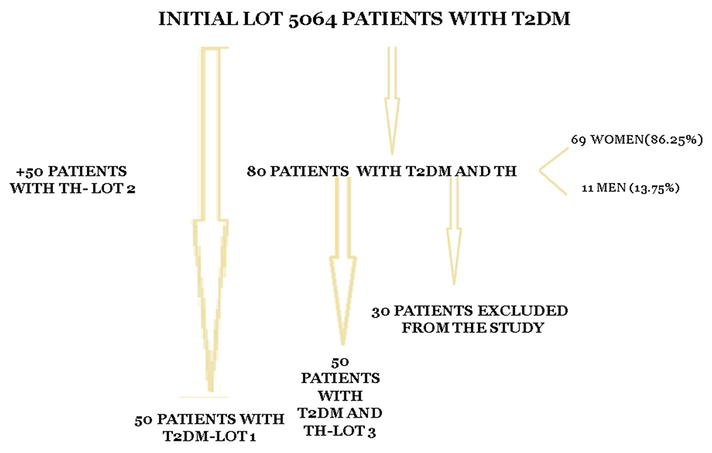
80
11
69
789.89
230.80
1286.83
Incidence of HT in the general population of Europe*
259.12
85.36
419.72
Table 1.
Incidence of patients diagnosed with HT after acquisition of T2DM in the study group and incidence at European level [3].
2.2.6 Analytical discussions: Study 1
Comparing our incidence studies of HT in a population with T2DM with incidence studies of HT in the general population published in the literature, we found similarities. A study conducted by Wiersinga et al. showed a prevalence of HT of 10–12% in the general population, making it the most common autoimmune disease encountered. The higher prevalence was observed in women, increasing with age and being higher in the white versus black population worldwide [4].
In terms of incidence worldwide, this study showed an incidence of 350 per 105 per year in women and 60 per 105 per year in men in non-iodine-deficient areas and 44 per 105 per year in women and 12 per 105 per year in men in iodine-deficient areas. [4] In our study, the incidence was 789.89 per 105, which allows us to conclude that T2DM may be a risk factor involved in the occurrence of HT, since the incidence in the population with T2DM is much higher than the incidence in the general population. Also in our study, the incidence was higher in women than in men, which is in agreement with the results of the study previously mentioned. The population in our study, the initial sample of 5064 patients, were mainly patients from Bucharest and from vicinity of the country’s capital, so from areas without iodine deficiency, also the patients were white (Caucasian). Comparing with the results of the aforesaid study, in which the highest incidence was in white patients from areas without iodine deficiency, we can say that the results of our study are in agreement with those described in the study by Wiersinga et al. In our study, the highest incidence was in females, almost six times higher than in males; in females, it was 1286.83 per 105 per year, while in males, it was 230.80 per 105 per year, and these data agree with the previously mentioned results, where a higher incidence was shown in females versus males.
Another study led by Lee et al. showed an HT incidence in the US population of 350 per 105 per year in women and 80 per 105 per year in men, with an incidence of nearly 600 per 105 from the Appalachian Mountain region. In this study, a global incidence of HT was estimated at 30–150 per 105, 10–15 times higher in women than in men, occurring most frequently in the 30–50 age group in women, with a peak incidence in men 10–15 years later [5]. The results of our study agree with those of this study, with a higher incidence among women than men of six times higher. The age group in which occurred most frequently in our study HT in the population with T2DM studied was in women between 60 and 70 years, and for men it was the same age category. These results are not in agreement with those of the study conducted by Lee et al., with the peak incidence in that study being at age of 30–50 years for women and 45–60 years for men. We can say that our population being composed of patients with T2DM had an older age than the general population studied in that study of HT incidence; thus, these results are in agreement with the average age of the people studied by us. We notice, however, that the proportion in relation to the predominant gender, female, is preserved.
In another study conducted by Dong et al. in the US army, on 20.270688 soldiers, predominantly male 85.8%, an incidence of HT of 758 cases in females and 548 cases in males was described. This study showed that the highest incidence was in the white Caucasian population, and the lowest incidence was in black females (IRR, 0.33; 95% Cl, 0.21–0.51) and black males (IRR, 0.22; 95% Cl, 0.11–0.47), in Asian Pacific Islander females (IRR, 0.31; 95% Cl, 0.17–0.56) and in Asian Pacific Islander males (IRR, 0.23; 95% Cl, 0.07–0.72) [6]. The results of this study are mainly determined by the preponderantly male gender of the study participants (85.8% were male), but even so we can observe that the number of HT cases in females is higher, 758, than in males, 548. Considering that the female population of the study was 14.2%, we can say that the incidence in the female population is much higher than in the male population. These results were also obtained by us in our study, a much higher incidence in women. Our study evaluated only white, Caucasian population, which, by comparison to the increased incidence in the study conducted by Dong et al. in the white population, could explain a high incidence rate in our study population as well.
2.2.7 Conclusions of study 1
As a conclusion of Study 1 “Determining the incidence of chronic autoimmune lymphocytic thyroiditis in a population of patients diagnosed with Type 2 Diabetes Mellitus,” we can state that we have demonstrated our main objective: we have shown that T2DM is a risk factor for the development of autoimmune thyroiditis through a higher incidence of HT among patients with T2DM versus the general European population (789.89/105 per year, with an incidence of 230.80/105 per year among diabetic men respectively an incidence of 1286.83/105 per year among women versus 259.12/105 per year, 85.36/105 per year among men and 419.72/105 per year among women in the general European population).
2.3 Study 2: clinicometabolic and therapeutic features in patients with type 2 diabetes mellitus and Hashimoto’s autoimmune thyroiditis
2.3.1 Introduction
After demonstrating the main objective of this research thesis, proving the statistically significant association between T2DM and HT, by means of Study 1, through determining the incidence of chronic autoimmune lymphocytic thyroiditis in a population of patients diagnosed with type 2 diabetes mellitus, we set out to evaluate the possible causes for this association: we aimed to detect the clinicometabolic and therapeutic features in patients with type 2 diabetes mellitus and Hashimoto’s autoimmune thyroiditis.
2.3.2 Objectives of study 2
The objectives of Study 2 are as follows:
to determine the weights of associated pathologies impacting the two studied pathologies in the three groups,
to determine the implications of IR assessed by surrogate indices of IR, that is, whether it correlates with the presence or absence of the studied association,
to determine the correlation of obesity with the presence or absence of HT in the group of patients with T2DM,
to determine the correlation of dyslipidaemia with the presence or absence of HT in the T2DM group of patients,
to determine whether metabolic syndrome correlates with the presence of absence of HT in the T2DM group of patients,
to determine the existence of clinicometabolic features of micro- and macrovascular complications of T2DM in patients with HT.
2.3.3 Purpose
We aimed to:
evaluate the relationship between the clinicometabolic factors in the groups of patients with T2DM, HT, T2DM and HT,
determine independent predictors of the association of the two pathologies studied,
evaluate the risk factors or the protection factors involved in the occurrence of HT in patients with T2DM.
After evaluating the 5064 patients diagnosed with T2DM and determining the incidence of HT in the study population, we developed a new study, Study 2—Clinicometabolic and therapeutic features in patients with type 2 diabetes mellitus and Hashimoto’s autoimmune thyroiditis study, to try to better understand the association between the two pathologies. We selected from the group of patients with T2DM and HT a number of 50 patients who were eligible to participate in our study. Of the initial 80 patients diagnosed with HT, 11 also suffered from other autoimmune diseases (Graves Basedow disease—5, rheumatoid polyarthritis—4, vitiligo—1 and ankylosing spondylitis—1), 7 had advanced chronic diseases or physical disabilities that prevented them from continuing the investigations needed to complete the study database, 3 had severe mental illnesses that prevented them from making judgements and 9 refused to continue the investigations needed to complete the study database. Thus, out of the total of 80 patients diagnosed with HT, only 50 were eligible after applying the exclusion criteria for the study, thus forming Group 3. Group 1 was made up of patients with only T2DM, also from the initial group followed in Study 1, out of 5064 patients with T2DM of the clinic, this being the control group. Group 2 included 50 patients with HT from the Endocrinology department’s records, also a control group. The selection of patients was consecutive; initially, patients were selected from Group 3, subsequently, from the same time period; consecutively, as they presented to the clinic, patients were selected for groups 1 and 2.
The mean age of the patients in the three groups was 58.1 years.
The study sample consisted predominantly of 122 (81.3%) female and (18.7%) male patients [7].
We found statistically significant differences between groups 1 and 2 and between groups 2 and 3 for the parameters: abdominal circumference, weight, BMI, obesity, dyslipidaemia and SM; and between groups 1 and 3 for TAD, cholesterol, macro- and microvascular complications, depression, visceral adiposity index (VAI), trigliceride glucose index (TyG), trigliceride glucose-body mass index (TyGBMI), trigliceride glucose-waist circumference index (TyGWC) and lipid accumulation product (LAP).
Univariate analysis revealed the following risks factors for HT in patients with T2DM: weight over 83.5 kg, BMI over 29.6 kg/m2, HbA1c over 5.85%, blood glucose over 122 mg/dl, thyroid-stimulating hormone (TSH) over 1.1 pmol/L, TyG over 4.7, TyG BMI over 140.8, and TyGWC, female gender, alcohol consumption, smoking, BCI, hypothyroidism, goitre, microvascular complications of T2DM, depression and insulin treatment.
After multivariate analysis, it was found that the protective factor TAD was retained and BMI, blood glucose and surrogate index of insulin resistance TyG, female gender, alcohol, smoking, hepatic steatosis, BCI, hypothyroidism and insulin treatment remained as risk factors.
Table 2 Values obtained in all three groups for surrogate markers: Group 1, Group 2 and Group 3.
TyG
TyGBMI
TyGWC
LAP
VAI
TG/HDL
4.8886
149.6063
449.84
57.11
1.8315
3.0914
Table 2.
Results of surogate markers for insulin resistance.
Surrogate indices of IR for each group, group 1, group 2 and group 3.
In the three groups studied, a TyG value of more than 4.7 was observed, but the highest value was detected in the combined group 5.02 (standard deviation 0.32335).
2.3.6 Analytical discussions: Study 2
2.3.6.1 Insulin resistance in patients with Hashimoto’s thyroiditis and euthyroidism
The relationship between IR and clinical and subclinical hypothyroidism is well-documented. Hashimoto’s thyroiditis (HT) is the most common cause of hypothyroidism.
Hashimoto’s thyroiditis is a chronic autoimmune inflammatory disease and the most common cause of hypothyroidism in adults. It is characterised by histological infiltration of T- and B-cells in the thyroid gland. Autoimmune diseases detect the body’s own tissue as foreign and work to destroy it. Therefore, the immune system starts producing anti-thyroid antibodies (anti-TPO) and anti-thyroglobulin antibodies (anti-Tg) to destroy the thyroid gland. It is not known why the body starts behaving this way. Perioxidase thyroid antibodies are positive in 95% of Hashimoto’s thyroiditis and 85% of Graves’ disease [8].
2.3.6.2 Personal discussion
In order to try to demonstrate a definitive link between IR and the association of the two pathologies studied in the present study, we used surrogate indices of IR, indices that have demonstrated their accuracy and precision in establishing the presence of IR in many other studies [9, 10, 11, 12, 13].
According to the study by Kim et al., the surrogate IR marker TyG was a better predictor for T2DM than Homa-IR, and VAI and LAP also had prediction for T2DM, but a more modest one than TyG. The conclusion of this study was that this TyG marker may be a useful additional tool to determine which patients are at risk of IR and T2DM [1].
The results of this study for the surrogate markers were TyG 4.7 +/− 0.2, VAI 2.5 +/−1.9 and LAP 38.5 +/−31.9. In our study, we obtained similar values TyG 4.88, VAI 1.83 and LAP 57.11, values for the whole group of 150 patients cumulated from groups 1, 2 and 3.
The cut-off values from the study by Kim et al. were 4.69 for TyG, 2.54 for VAI and 36.6 for LAP. In our study, we obtained cut-off values of 4.7 for TyG, 1.4 for VAI and 27.19 for LAP.
In the study by Guerrero-Romano et al., a cut-off value for the IR determination of TyG of 4.68 was established [14]. Considering that the results of the two mentioned studies were similar to the results of our study, we can conclude that a TyG of 4.7, obtained by us, is diagnostic for IR.
Correlating the results obtained in the two studies conducted by Kimm et al. and Guerrero-Romano et al. with the results obtained in our study, we can state that the values obtained by us were diagnostic for IR.
In the study conducted by Kim et al., a strong relationship was established between the surrogate marker of IR, TyG and the occurrence of T2DM, which was found to be a better predictor of T2DM than HOMA-IR [1].
In a meta-analysis conducted by Song et al., obesity was shown to be a risk factor for HT occurrence, with odds ratio (OR) of 1.91 (Cl 95% 1.10–3.32) and p = 0.022 [15]. In our study, after risk analysis, obesity was not retained as a risk factor, but an increased BMI at the upper limit of overweight, 29.6 kg/m2, close to the limit of obesity, with p = 0.008 and an odds ratio of 1.230 (CL 95% 1.056–1.432), was found to be a risk factor in the occurrence of HT in patients with T2DM. Thus, our data are in agreement with those stated by Song et al.
We also found similar results to our study in the publication by Du et al., where it was shown that in diabetic patients, a high blood glucose was a risk factor involved in the occurrence of thyroid pathologies, with OR of 2.653 (Cl 95% 1.18–5.9) and p = 0.019 [16]. Our results were also in agreement with what Du et al. presented, and a blood glucose value over 122 mg/dL was also in our case an independent predictor of HT occurrence in diabetic patients, with OR of 1.023 (Cl 95% 1.007–1.040) and p = 0.004.
The study led by Choi et al. was the first to indicate TyG as a surrogate marker of IR in its evaluation in relation to thyroid dysfunction. It showed higher predictive values for the thyroid pathology including HOMA-IR, with OR of 1.81 and p = 0.031 [17]. Our study showed that at a TyG over 4.7, the risk of developing HT among patients with T2DM is 65-fold higher, with OR of 65.344 (Cl 5.067–842.607) and p = 0.001. We can state as a conclusion that our study is the second to demonstrate the predictive value of TyG for thyroid pathologies and the first that demostrates this in regards to Hashimoto`s autoimmune thyoriditis.
In the study led by Lee et al. [5], a 10–15-fold higher incidence of HT among females was shown, and similar results were also found in our study, which allows us to comment the result obtained that the female gender is at a risk factor of occurrence of HT in the patients with T2DM. For female gender, we obtained OR of 23.176 (Cl 4.530–118.572) and p = 0.0001 after multivariate analysis performed comparing the groups of patients with T2DM and with HT and T2DM. This result is not surprising in the context of the high incidence of HT among the female population.
Another risk factor for developing HT in patients with T2DM, comparing groups 1 and 3, is that our study found was alcohol consumption, with OR of 7.048 (Cl 95% 2.187–22.720) and p < 0.001. From our results, we can state that alcohol increases risk of developing HT, among the diabetic patients by 7 times, which is statistically significant. Comparing with the literature, we did not find another study attesting the risk; therefore, we can state that our study is the first to certify the causal relationship between the two. Moreover, a study conducted by Efferaimidis et al. showed that there is no association between alcohol consumption and de novo development of TPO antibodies. The results of this study are not in agreement with the results of our study [18].
Univariate analysis between groups 1 and 3 showed that BCI is also a risk factor for developing HT in patients with T2DM, with OR of 5.318 (Cl 95% 2.214–12.774) and p < 0.001. We found no other studies in the literature that addressed this relationship, but we did find one study that addressed the inverse relationship, and it described a twofold increased risk in HT patients to develop BCI, with OR of 2.06 (Cl 95% 1.46–2.92) [19]. Interpreting the results inversely, we can say that BCI may also be a risk factor involved in the development of HT, even with a higher prediction value, the risk being in this case five times higher in the population with T2DM. The higher result is somewhat normal, given that the population we studied was composed of diabetics, who have a higher proportion of associated BCI. Again our study is the first to demonstrate a positive independent predictor relationship for BCI in terms of the occurrence of HT in patients with T2DM.
The study conducted by Ogbonna et al. [20] showed a higher risk of patients with thyroid pathologies to develop diabetic nephropathy, with OR of 4.8 and p = 0.001. Considering diabetic nephropathy a part of microvascular complications of diabetes we can say that the results of our study are so similar to those of the above-mentioned study. In our case, after analysis of the comparison between groups 1 and 3, it was shown that there is a four times higher risk of developing HT among patients with microvascular complications among the population with T2DM; in other words, the presence of microvascular complications is a risk factor for the development of the association between the two pathologies, with OR of 4.571 (Cl 95% 1.963–10.646) and p < 0.001.
Another parameter that had statistical significance as a risk factor for the association between HT and T2DM was depression, this time in the comparison between the groups 2 and 3, with OR of 9.333 (Cl 1.121–77.204) and p < 0.001. In the study conducted by Bode et al., a positive predictive value for hypothyroidism was demonstrated for depression, with OR 1.30 (Cl 95% 1.08–1.57), while for autoimmune thyroid pathologies the results were inconclusive, with OR 1.24 (Cl 95% 0.89–1.74) [21]. Unfortunately, this situation is also confirmed by us, and the depression parameter maintains statistical significance for the other groups and not even after multivariate analysis of the data.
2.3.7 Conclusions of study 2
The univariate analysis revealed the following risk factors for developing HT in patients with T2DM: weight over 83.5 kg, BMI over 29.6 kg/m2, HbA1c over 5.85%, blood glucose over 122 mg/dl, TSH over 1.1 pmol/L, TyG over 4.7, TyG BMI over 140.8, and TyGWC, female gender, alcohol consumption, smoking, BCI, hypothyroidism, Goitre, microvascular complications of T2DM, depression and insulin treatment.
After multivariate analysis, it was found that the protective factor TAD was retained and BMI, glycaemia and surrogate index of insulin resistance TyG, female gender, alcohol, smoking, hepatic steatosis, BCI, hypothyroidism and insulin treatment remained as risk factors.
T2DM is a risk factor for the development of autoimmune thyroiditis through a higher incidence of HT among patients with T2DM versus general European population.
Female gender was found to be a risk factor involved in the occurrence of HT in patients with T2DM, probably determined by the high incidence of thyroid pathology in female population.
Insulin resistance seems to be the vector linking HT and T2DM. A value of TyG, a calculated insulin resistance surrogate index, above 4.7 was found to be a risk factor involved in the occurrence of HT in patients with T2DM, and TyG increased the risk of occurrence of HT in the T2DM population by 65-fold.
Insulin resistance seems to be the vector linking HT and T2DM.
Overweight is a risk factor involved in the association of HT in patients with T2DM most likely through a week metabolic control, since it is known that overweight and obesity is a cause of glycaemic imbalance.
Abdominal obesity, above 88,5 cm, increases the risk of HT association with T2DM 6-fold, and this is caused also by a metabolic imbalance.
Blood glucose above 122 mg/dl was found to be an independent predictor of association of HT with T2DM, proving once more that a week metabolic control is the probable cause of the association between the two studied pathologies.
Insulin treatment increased the risk of developing HT in patients with T2DM over seven times, showing once again the involvement of the metabolic control in this association.
The correlation between elevated HbA1c, metabolic syndrome and elevated ATPO values was shown with increased statistical significance (p < .001) to be the pathophysiological link between T2DM and HT.
High systolic blood pressure increases the risk of HT in patients with T2DM almost threefold, and this is explained through the pathophysiological mechanism of cerebral insulin resistance involved in the pathology of arterial hypertension, mechanism which was proven by high values of insulin resistance markers; this allows us to conclude that insulin resistance is the real risk factor.
Diastolic blood pressure below 77.5 mmHg seems to have a protective effect on the occurrence of HT in patients with T2DM, because the normal or low values of diastolic blood pressure do not associate with insulin resistance, and this does not only elevate the risk, but gives a protective effect against the association of the two pathologies.
Hepatic steatosis is a risk factor for HT association in patients with T2DM, due to the high level of insulin resistance that low metabolic control patients have, as we have shown already.
The presence of ischemic heart disease increased the risk of HT association with T2DM twice, the pathophysiological mechanism to blame for this looks to be insulin resistance, especially the cardiac one, correlated with a low metabolic control.
Hypothyroidism was found to be risk factor for the association of HT with T2DM, and an association of high values of TSH in patients with type 2 diabetes can lead to a metabolic disorder, which seems to be the real risk factor for the association of Hashimoto thyroiditis with type 2 diabetes.
Smoking increased T2DM patient’s risk of developing HT sevenfold, it is known that smoking is a risk factor for autoimmune thyroid disorders, and in our study, it was also confirmed to be a risk factor for developing HT.
Alcohol consumption increased T2DM patient’s rick of developing HT by almost 3.5-fold; the probable cause is the destruction of the gland due to the increased toxicity associated with alcohol intake, this being probably followed by an autoimmune destruction.
This is the first study to demonstrate the predictive value of TyG for Hashimoto’s autoimmune thyroiditis.
Our study is the first to certify the causal relationship between alcohol consumption and the occurrence of HT in patients with T2DM.
Again our study is the first to demonstrate a positive independent predictive factor relationship for BCI with respect to the occurrence of HT in patients with T2DM.
The results of our study attest the need to introduce screening for the autoimmune thyroid pathologies among patients with T2DM.
References
1.Kim B, Choi HY, Kim W, Ahn C, Lee J, Kim JG, et al. The cut-off values of surrogate measures for insulin resistance in the Korean population according to the Korean genome and epidemiology study (KOGES). PLoS One. 2018;13(11):e0206994. DOI: 10.1371/journal.pone.0206994
2.Lim J, Kim J, Koo SH, Kwon GC. Comparison of triglyceride glucose index, and related parameters to predict insulin resistance in Korean adults: An analysis of the 2007-2010 Korean National Health and nutrition examination survey. PLoS One. 2019;14(3):e0212963
3.Madariaga AG, Palacios SS, Guillen-Grima F, Galofre JC. The incidence and prevalence of thyroid dysfunction in Europe: A meta-analysis. The Journal of Clinical Endocrinology and Metabolism. 2014;99(3):923-931
5.Lee SL, Griffing GT. What is the incidence of Hashimoto’s thyroiditis in the US?. 2020. Available from: https://www.medscape.com/answers/120937-122448/what-is-the-incidence-of-hashimoto-thyroiditis-in-the-us
6.McLeod DSA, Caturegli P, Cooper DS, Matos PG, Hutfless S. Variation in rates of autoimmune thyroid disease by race/ethnicity in US military personnel. Journal of the American Medical Association. 2014;311(15):1563-1565. DOI: 10.1001/jama.2013.285606
7.Parlițeanu O, Cheța D. Type 2 diabetes and Hashimoto’s thyroiditis-possible associations and clinical correlations - preliminary results. Romanian Journal of Diabetes Nutrition and Metabolic Diseases. 2018;25(3):297-301
8.Ozkardes A, Ozata M, Beyhan Z, Vural O, Yardim M, Gundogan MA. Acute hypothyroidism leads to reversible alterations in central nervous system as revealed by somatosensory evoked potentials. Electroencephalography and Clinical Neurophysiology. 1996;100(6):500-504
9.Ji B, Qu H, Wang H, Wei H, Deng H. Association between the visceral adiposity index and homeostatic model assessment of insulin resistance in participants with normal waist circumference. Angiology. 2017;68:716-721
10.Oh JY, Sung YA, Lee HJ. The visceral adiposity index as a predictor of insulin resistance in young women with polycystic ovary syndrome. Obesity (Silver Spring). 2013;21:1690-1694
11.Khan HS. The lipid accumulation product is better than BMI for identifying diabetes. Diabetes Care. 2006;29:151-153
12.Simental-Mendía LE, Rodríguez-Morán M, Guerrero-Romero F. The product of fasting glucose and triglycerides as surrogate for identifying insulin resistance in apparently healthy subjects. Metabolic Syndrome and Related Disorders. 2008;6:299-304
13.Vasques AC et al. TyG index performs better than HOMA in a Brazilian population: A hyperglycemic clamp validated study. Diabetes Research and Clinical Practice. 2011;93:e98-e100
14.Jali MV, Kambar S, Jali SM, Pawar N, Nalawade P. Prevalence of thyroid dysfunction among type 2 diabetes mellitus patients. Diabetes and Metabolic Syndrome. 2017;11(Suppl. 1):S105-S108
15.Song RH, Wang B, Yao QM, Li Q , Jia X, Zhang JA. The impact of obesity on thyroid autoimmunity and dysfunction: A systematic review and meta-analysis. Frontiers in Immunology. 2019;10:2349
16.Du Wenhua WF, Meng Z, Haiqing Z, Xu Z, Jia-Jun Z, Ling G. Prevalence of thyroid disorders and associated risk factors with various glycemic status in North China. Biotechnology & Biotechnological Equipment. 2019;33:1244-1250. DOI: 10.1080/13102818.2019.1656106
17.Choi W, Park JY, Hong AR, Yoon JH, Kim HK, Kang H-C. Association between triglyceride-glucose index and thyroid function in euthyroid adults: The Korea National Health and nutritional examination survey. PLoS One. 2021;16(7):e0254630
18.Effraimidis G, Tijssen JG, Wiersinga WM. Alcohol consumption as a risk factor for autoimmune thyroid disease: A prospective study. European Thyroid Journal. 2012;1(2):99-104
19.Chen W-H, Chen Y-K, Lin C-L, Yeh J-H, Kao C-H, Thyroiditis H's. Risk of coronary heart disease, and L-thyroxine treatment: A Nationwide cohort study. The Journal of Clinical Endocrinology & Metabolism. 2015;100(1):109-114
20.Ogbonna SU, Ezeani IU. Risk factors of thyroid dysfunction in patients with type 2 diabetes mellitus. Frontiers in Endocrinology (Lausanne). 2019;10:440
21.Bode H, Ivens B, Bschor T, Schwarzer G, Henssler J, Baethge C. Association of hypothyroidism and clinical depression: A systematic review and meta-analysis. JAMA Psychiatry. 2021;78(12):1375-1383
Written By
Oana-Andreea Parliteanu, Octavian Alexe, Corina Risca (Popazu), Dan Mircea Cheta and Cristiana Voineag
Submitted: 02 January 2024Reviewed: 23 February 2024Published: 26 April 2024