Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
To purchase hard copies of this book, please contact the representative in India:
CBS Publishers & Distributors Pvt. Ltd.
www.cbspd.com
|
customercare@cbspd.com
Malignant colorectal polyp refers to the polyp in which the neoplastic lesion invades into but not beyond the submucosa. The morphological features and surface patterns of the malignant polyps are examined by the white-light and image-enhanced endoscopy, which help to predict the depth of invasion of neoplastic lesions. The deep submucosal invasion is associated with a high risk of residual cancer and lymph node metastasis. The image-enhanced endoscopy is useful in identifying the malignant polyp amenable for endoscopic resection or require formal oncological surgery. After the endoscopic resection of the polyp, the thorough histopathological assessment is required to determine the possibility of residual tumor, recurrence, and lymph node involvement. The presence of high-risk features (deep submucosal invasion, poor differentiation, lymphovascular invasion, <1 mm resection margin, piecemeal resection, and tumor budding) indicates a need for surgical resection with lymph node clearance. In low-risk cases, the endoscopic resection is considered adequate and further surveillance is advised. The final decision about the endoscopic resection versus surgical resection of malignant polyp needs to be individualized and should be based not only on polyp related characteristics but also on comorbidities, local resources, expertise availability, and patient’s preference.
Department of Gastroenterology, Nepal Mediciti Hospital, Bhaisepati, Lalitpur, Nepal
*Address all correspondence to: umidshrestha@gmail.com
1. Introduction
Malignant colorectal polyp (MP) refers to the polyp in which the cancer cells invade into but not beyond the submucosa, regardless of lymph node involvement [1]. Colorectal cancer (CRC) is defined as the invasion of cancer cells beyond the muscularis mucosa. Since the colonic mucosa is devoid of lymphatics, the cancer cells confined to the muscularis mucosa have a negligible risk for lymph node metastasis (LNM) and hence are defined as benign (non-malignant) polyps [2]. According to the American Joint Committee on Cancer tumor-node metastasis classification system, an MP represents early CRC and is categorized as pT1 [3]. Different studies have shown that at least 0.2–8.3% of colorectal polyps are MPs [4, 5, 6, 7]. The CRC has become the third most commonly diagnosed form of cancer, and its incidence reaches approximately 1.9 million cancer cases each year (10% of all new cancer cases globally) [8]. Traditionally, the incidence of CRC increases strongly with age and is highest in Western, affluent countries, but the change in the lifestyle has made its incidence increasing in many less developed countries and in younger generations in both developed and developing countries [8].
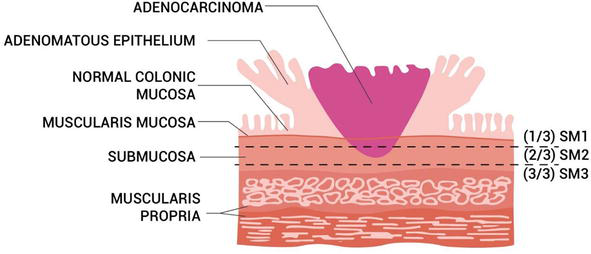
The CRC arises from the progressive accumulation of genetic and epigenetic alterations. The adenoma-to-carcinoma sequence in development of CRC is shown in the Figure 1. The sequence involves the transformation of normal colorectal epithelium to adenoma and ultimately to invasive and metastatic tumor. Such malignant transformation requires up to 15 years, depending on the characteristics of the lesion and on other independent risk factors, such as gender, body weight, body mass index, physical inactivity [9]. The chromosomal instability (CIN), microsatellite instability (MSI), and CpG island methylator phenotype (CIMP) pathways are responsible for genetic and epigenetic instability in CRC [10, 11]. The CIN pathway consists of activation of proto-oncogene Kirsten-ras (K-ras) located on chromosome 12p and inactivation of at least three tumor suppression genes, namely, loss of APC (Adenomatous Polyposis Coli gene) located on chromosome 5q, DCC (Deleted on Colorectal Cancer gene) located within the region of loss of heterozygosity (LOH) of long arm of chromosome 18q, and p53 located on chromosome 17p [10, 11].
Figure 1.
Adenoma-to-carcinoma sequence in development of colorectal cancer.
With the increasing CRC screening programs, the detection of early CRC has become possible, leading to an increase in the number of people identified as having MP [12, 13, 14]. There is often a dilemma regarding the management of MP: the first dilemma is at the time of colonoscopy, when the endoscopist must decide whether a suspicious polyp can be safely endoscopically resected; the second dilemma is after pathologic examination of a polypectomy specimen, when a decision must be made about attempted endoscopic re-excision, surgical resection, or surveillance. The management decision requires an assessment of the endoscopic and pathological features, risk of adverse outcome after endoscopic polypectomy, risk of surgery, and the available surgical options. There are additional considerations in high-risk patients, for instance, those with a family history suggesting hereditary nonpolyposis colorectal cancer (HNPCC), long-standing inflammatory bowel disease, and familial polyposis. This chapter deals primarily with the average-risk patient with an aim to review the endoscopic and pathological features of MP and to discuss about the management strategies of MP.
During colonoscopy, all colorectal lesions should be examined by white-light and image-enhanced techniques to differentiate between adenomas and CRC and to predict the depth of invasion [13, 15]. The deep submucosal invasion (SMI) is associated with a high risk of residual cancer and LNM [13, 16]. Gross morphological features and polyp surface patterns are carefully examined during endoscopic evaluation of polyp.
2.1 Gross morphological features
The endoscopic gross features of malignancy include an irregular surface contour, ulceration, firm (or hard) consistency, and broadening of the stalk [17, 18, 19, 20, 21, 22, 23]. Although polyps with these features are not invariably malignant, any lesion with malignant characteristics should be carefully evaluated in order to identify the resectable adenoma.
The Paris classification should be used as following for the endoscopic classification of superficial colorectal lesions: polypoid (pedunculated 0-Ip and sessile 0-Is), non-polypoid (elevated 0-IIa, flat 0-IIb, depressed 0-IIc), and excavated or ulcerated lesions (0-III) [16]. The risk of MP (and CRC) seems to be directly proportional to polyp size and the presence of depression: with the risk being as high as 40% in smaller lesions (6–10 mm) to nearly all lesions measuring more than 20 mm [24, 25, 26]. The Paris Classification does not address the lateral spreading tumor (LST), which is defined as the superficial non-polypoid colorectal lesion measuring more than 10 mm in diameter, with flat (0-II) or sessile (0-Is) morphology, extending laterally rather than vertically along the colonic wall. On routine colonoscopy, the incidence of LST is approximately 9% [25]. The LST can be broadly subdivided into the granular (LST-G) or non-granular (LST-NG) type [27].
The risk of SMI is as high as 30% in LST-G of more than 30 mm size with mixed-size nodules, whereas LST-G with a homogenous nodular pattern has a low risk of invasion (<2%) [28]. LST-NG is characterized by a smooth surface and can be either flat or pseudo-depressed. The LST-NG with pseudo-depression carries the highest risk of SMI among LSTs (31.6%; 95%CI: 19.8–43.4%) [29].
The location is another important risk factor for SMI. The LST-G mixed type or LST-NG lesion in the rectosigmoid colon carries the highest risk for malignancy [30]. Within the serrated pathway, most carcinomas arise in the cecum or ascending colon, and approximately one-third arise in the rectum [31].
Other gross morphological features that correlate with SMI have also been studied. In one prospective multicenter study including more than 2000 lesions >10 mm, it was found that non-lifting, chicken-skin sign (pale yellow-speckled mucosa), edge retraction, depressed areas, fold convergence, induration, ulceration, and polyp over polyp were all significantly associated with deep SMI [32]. However, the sensitivity of these features for diagnosing deep SMI seems to be low, ranging from 0.18 to 0.68, with specificity varying from 0.8 to 0.98 [33].
2.2 Polyp surface pattern
Besides gross morphology, the risk of SMI can also be assessed by the surface vascular and pit pattern of polyp, which helps in reaching the management decisions. The polyp surface is characterized by image-enhanced endoscopy (IEE), which can be performed by conventional chromoendoscopy and electronic or virtual chromoendoscopy. The conventional chromoendoscopy is dye-based (contrast: indigo carmine; absorptive: crystal violet) and assesses the pit pattern, whereas the electronic or virtual chromoendoscopy is equipment-based (Olympus: NBI; Pentax: I-scan; Fujifilm: BLI, LCI) and assesses the capillary pattern. The polyp surface characterization has been classified by different methods, including Narrow-Band Imaging International Colorectal Endoscopic (NICE) classification system, Japan NBI Expert Team (JNET) classification system, Kudo pit pattern nomenclature, and others.
2.2.1 NICE classification system
Narrow-band imaging (NBI) is a form of electronic or virtual chromoendoscopy initially developed by Sano et al. in 1999 [34, 35]. The NBI enables detailed assessment of the capillary mucosal pattern of polyps by filtering white light into specific wavelengths to enhance the superficial microvascular structures [34, 35]. The NBI has been used for the optical diagnosis of colorectal tumors in NICE classification system, which is based on the color, vessels, and surface pattern on endoscopy [36, 37]. In this classification scheme, polyps can be divided into three categories (type 1, 2 or 3) based on their appearance (Table 1). NICE type 1 and 2 polyps are benign and can be resected endoscopically. Type 3 polyps are characterized by disrupted/missing vessel pattern and amorphous or absent surface pattern on NBI and are highly suggestive of deep SMI, requiring surgical resection.
Type 1
Type 2
Type 3
Color
Same or lighter than background
Browner relative to background
Brown to dark brown relative to background
Vessels
None or lacy vessels
Brown vessels
Disrupted or missing vessels
Surface pattern
Dark or white spots of uniform size
Oval, tubular, or branched white structures
Amorphous or absent surface pattern
Most likely pathology
Hyperplastic and sessile serrated polyp
Adenoma
Deep submucosal invasive cancer
Table 1.
NBI International Colorectal Endoscopic (NICE) classification system.
2.2.2 JNET classification system
The JNET introduced an NBI-magnifying endoscopic classification system for colorectal polyps in 2014 [36, 38]. The JNET system classifies colorectal polyps into four types (Types 1, 2A, 2B, and 3) (Table 2). Type 3 polyps are characterized by irregular or amorphous vessel and surface patterns under magnified endoscopy with NBI; these type 3 polyps are highly suggestive of deep SMI and require surgical resection.
Type 1
Type 2A
Type 2B
Type 3
Vessel pattern
Invisible
Regular caliber and distribution (meshed/spiral)
Variable caliber, irregular distribution
Loose vessel areas, interruption of thick vessels
Surface pattern
Regular dark or white spots similar to surrounding mucosa
Regular (tubular/branched/papillary)
Irregular or obscure
Amorphous areas
Most likely pathology
Hyperplastic or sessile serrated polyps
Low-grade dysplasia
High grade dysplasia/shallow submucosal invasive cancer
Deep submucosal invasive cancer
Table 2.
Japan Narrow-band imaging Expert Team (JNET) classification system.
2.2.3 Kudo’s pit pattern
Kudo and colleagues classified colorectal polyps according to their appearance, structure, and staining patterns by using magnifying endoscopy [39, 40]. Type I pits appear as roundish pits; type II pits appear as stellar or papillary pits; type III-s pits are small roundish, tubular pits (smaller than type I), and type III-L are roundish and tubular pits (larger than type I); type IV pits appear as branch-like or gyrus-like pits, and type V pits appear as amorphous, nonstructured pits [39, 40].
Most colorectal polyps (Kudo pit pattern types I through IV) are benign polyps and are amenable to endoscopic resection, whereas those with Kudo pit pattern V are suggestive of deep SMI and require surgical resection [26, 41].
Artificial intelligence (AI) has emerged as an exciting tool in identifying the endoscopic resectability in colorectal polyps by differentiating noninvasive and superficially submucosal invasive neoplasms and deeply invasive cancer. The AI white light systems have shown high accuracy, sensitivity, and specificity in predicting the feasibility of curative endoscopic resection of large colonic lesions [42, 43]. In a study done by Kudo et al., the AI model was validated to identify T1 colorectal tumors at risk for metastasis to the lymph nodes [44]. At this point of time, incorporating AI into clinical practice in the management algorithm of MP may be challenging, but the results of the AI study provide valuable insights into the future trends and potential of AI in the management of MP.
Accurate histopathological assessment is critical in determining adequacy of endoscopic resection of MP, and hence, every effort must be made to retrieve the entire specimen. This is easier for pedunculated polyps than for large sessile polyps that are removed in piecemeal fashion. Saline injection to provide a cushion of normal mucosa under a sessile polyp can greatly aid in the completeness of removal.
4.1 Depth of submucosal invasion (SMI)
The level of SMI is important in predicting the outcome of MP in both pedunculated and sessile polyps. Studies have shown that deeper depth of invasion is related to increased LNM and a poorer outcome [45, 46, 47].
The Haggitt classification is used to describe the level of invasion (0—neoplastic cells confined to the mucosa, 1—head, 2—neck, 3—stalk, 4—submucosa of underlying colonic wall) in pedunculated polyps (Figure 2) [45]. The study done by Haggitt et al. showed that a depth of invasion to Haggitt level 4 was a significant adverse prognostic factor for pedunculated MP. Another study done by Nivatvongs et al. showed that there was no incidence of lymph node metastasis for pedunculated Haggitt level 1 to 3, but the risk of lymph node metastasis was as high as 27% for level 4 lesions [48]. For sessile polyps, the Kikuchi classification is used, in which three levels are present based on the degree of SMI: Sm1–invasion into the upper third of the submucosa; Sm2–invasion into the middle third; and Sm3–invasion into the lower third (Figure 3) [46]. The study done by Kikuchi et al. showed that the risk of metastasis was 0% in Sm1 lesions but increased to as high as 14.4% in Sm3 lesions [46]. Another study done by Kitajima et al. showed that for sessile MP, the risk of LNM was 0% if the depth of SMI was less than 1000 μm but increased to more than 11.5% when the depth of invasion exceeded 1000 μm [47]. In a meta-analysis by Beaton et al., it was shown that that the risk of LNM was significantly higher when the depth of SMI was more than 1000 μm [49].
Figure 2.
Haggitt classification system of pedunculated polyp (adapted from Haggitt et al [45]).
Figure 3.
Kikuchi classification system of sessile polyp (adapted from Kikkuchi et al [46]).
As such, the surgical resection is advised for pedunculated MP with Haggitt level 4 and for sessile MP with Sm3 lesion and SMI of more than 1000 μm.
The study done by Toh et al. showed that a width of invasion more than 11.5 mm and an area of SMI more than 35 mm2 were significant predictors for LNM [50]; however, this study was limited by its small sample size and retrospective nature.
4.2 Margin of resection
The positive margin of resection has been defined differently in various literature as tumor <1 mm or < 2 mm or within the cautery of the resection margin [2, 14, 51]. The study has shown that there is increased adverse oncological outcomes if tumor cell is at or near the resection margin [52, 53, 54, 55]. In a study done by Hassan et al., it was shown that the patient with positive resection margin had a higher residual and recurrent disease rate and higher rate of hematogenous metastasis and cancer-related mortality [52]. The another study done by Cooper et al. showed that there was an increased rate of recurrence of up to 33% when the resection margin was ≤1 mm [54]. Based on the recent scientific evidence, we suggest that 1 mm cutoff margin be a suitable positive margin.
4.3 Tumor differentiation
The tumor differentiation has been categorized into three grades based on the degree of glandular differentiation: grade 1 (well-differentiated), grade 2 (moderately differentiated), and grade 3 (poorly differentiated). The neoplastic lesions with poor differentiation have been shown to be associated with a significantly higher incidence of lymphatic spread and cancer-related mortality [56].
4.4 Lymphovascular invasion
Lymphovascular invasion (LVI) is another important poor prognostic indicator and predictor of patient outcome. The presence of LVI in MP has been associated with an increased risk of regional LNM [56].
4.5 Tumor budding
A single or cluster of up to 5 tumor cells at the advancing front of the tumor has been defined as tumor budding [51, 57]. This has been regarded as a significant risk factor for LNM [56].
4.6 Histological tumor type
A higher risk of LNM has also been found in the MP with cribriform or micropapillary variants [58, 59]. Moreover, the neoplastic lesions with mucinous or signet ring cells are also associated with a poor prognosis, requiring the surgical resection [60, 61].
The representative endoscopic pictures of the colorectal polyps with regard to the SMI are shown in the Figures 4–8.
Figure 4.
Large sessile adenomatous polyp; histopathology report showed no SMI.
Figure 5.
Pedunculated adenomatous polyp; histopathology report showed no SMI.
Figure 6.
Sessile polyp with borad base with lobular surface; histopathology report showed MP with superficial SMI.
Figure 7.
Laterally spread tumor—granular (LST-G); histopathology report showed MP with deep SMI.
Figure 8.
Laterally spread tumor—non-granular (LST-NG); histopathology report showed MP with deep SMI.
The management of patients with MP requires a multidisciplinary team approach with the involvement of endoscopists, surgeons, gastrointestinal pathologists, radiologists, and medical oncologists. The flowchart of the proposed algorithm of MP is shown in the Figure 9.
Figure 9.
Proposed algorithm for the management of MP.
Once a colonoscopy reveals a colorectal polyp suggestive of MP, the first critical decision would be to decide whether to resect the polyp completely endoscopically. Depending on the nature of the polyp and availability of expertise, the endoscopic removal of MP can be done by conventional snare polypectomy, endoscopic mucosal resection (EMR), endoscopic submucosal dissection (ESD), or other advanced polypectomy technique, such as endoscopic full-thickness resection [16].
The polyps thought to be benign on endoscopy during endoscopic resection have been found to be MP after histopathological evaluation in many instances, and the management of such MP detected after endoscopic resection is difficult because it involves the risk of residual or recurrent disease and of LNM and the patients’ surgical risk [12, 22, 62]. Depending upon the morphological, endoscopic, and histological prognostic features, MP is stratified into high- and low-risk polyps. The high-risk features of the MP include poor differentiation, presence of LVI, deep SMI, positive margin, piecemeal resection, or tumor budding. Such MPs with high-risk features should undergo surgical resection with lymph node clearance, if medically fit [12, 13, 22, 62]. In the case of the MPs with low-risk features, the endoscopic resection is considered curative and should undergo a surveillance program with regular colonoscopies to detect early recurrence and minimize the risk of metachronous disease. It has been suggested that the surveillance be performed 3–6 months after endoscopic removal of the MP, with the subsequent evaluations to be done based upon the risk and findings [13, 22, 62, 63].
The polyps with certain morphological features associated with a relative high risk of superficial SMI include the polyps with depressed morphology (Paris IIc), LST-NG with depression or bulky sessile appearance (Paris Is component), and LST-G with dominant nodules [26]. Moreover, the risk also increases with lesions ≥20 mm and LSTs located in the right colon, rectosigmoid, and rectum [13, 26].
En-bloc endoscopic resection is needed while removing the probable superficial SMI, because piecemeal resection results in fragmented tissue specimens that compromise the accurate histological assessment. For pedunculated MPs with features suggestive of superficial SMI (Haggitt level 1–3) [16, 60], conventional snare polypectomy is considered adequate for the en-bloc resection and is regarded as curative when the histopathology report and margins are favorable [60]. In the case of large polyp, the snare should be placed closer to the bowel wall than to the head of polyp, in order to obtain the cancer-free resection margin [64].
For the non-pedunculated polyp, the polyp size determines the type of the endoscopic method used for the en-bloc resection [13]. For the lesions ≤20 mm in size, EMR may achieve en-bloc resection, during which the additional margin of normal tissue is snared around the polyp. On the other hand, for the lesions >20 mm in size, ESD is required to achieve en-bloc resection. ESD is associated with a higher en-bloc and curative resection rate and lower risk of recurrence [65], whereas EMR is associated with a higher risk of potential complications and failure during the en-bloc resection of polyps >20 mm [66]. However, ESD is a technically more complex procedure and is associated with a steep learning curve with higher rate of serious adverse events [62, 67].
The polyps with NICE type 3, Kudo class V, surface ulceration without prior manipulation (i.e. biopsies or resection attempts), or stiffness of the lesion and colon wall are suggestive of deep SMI and are associated with LNM and need for surgery [68, 69]. For pedunculated MP, it was found that Haggitt level 4 invasion, LVI, muscularis mucosae type B (incompletely or completely disrupted), poorly differentiated clusters, and tumor budding were the high-risk histologic features, which need the surgery [70]. In another study, it was shown that even in high-risk MP, a high proportion of patients do not have evidence of residual disease in the bowel wall or in the draining lymph nodes [56]. It seems prudent to recommend surgical resection only if 2 or more high risk histological features are present (risk of nodal metastasis: 23.3%); in cases where only one risk feature is present, the estimated risk of nodal metastasis is 4.5% [71].
Certain polyps have indeterminate characteristics that include the following: lesions with endoscopic appearance suggestive of deep SMI yet negative for invasive cancer on biopsies [72, 73], lesions with equivocal endoscopic appearance for deep SMI, and lesions with equivocal biopsy results (i.e., histopathology showing “at least” high-grade dysplasia yet deeper invasion cannot be excluded based on the limited sample). These polyps need to be properly evaluated and managed in a high-volume center with expertise in both endoscopic imaging and resection of complex polyps.
There should be a proper colonoscopic surveillance strategy for MPs with both postsurgical resection as well as endoscopic resection [14]. The patients of MP with high-risk features but without the involvement of lymph node, who underwent the formal oncological resection of colon with lymph node clearance, are regarded as a T1 CRC, and surveillance with colonoscopy should be done at 1 year and repeated in 3 years and then every 5 years if there are no advanced adenomas [14]. If the colonoscopy done at 1 year reveals advanced adenoma, the colonoscopic surveillance should be repeated in 1 year. The cross-sectional imaging, endoscopic surveillance, and serial carcinoembryonic antigen testing should be done as per the National Clinical Practice Guidelines in Oncology, if there is a lymph nodal involvement [14]. For the patients of MP with low-risk features, who underwent the endoscopic resection, the surveillance colonoscopy should be done at 3 months, then at 1, 3, and 5 years, as recommended by the US Multi-Society Task Force on Colorectal Cancer and the American Cancer Society [74].
With the increasing use of colonoscopy, many patients having MPs are being diagnosed. The management of MP is challenging and begins with the accurate endoscopic assessment of the polyp. The IEE helps to differentiate the superficial and deep SMI of the neoplastic lesion and identify the MP amenable for endoscopic resection or require formal oncological surgery. The endoscopic resection techniques, such as conventional polypectomy, EMR, or ESD, best suited for each type of polyp, need to be determined. After the endoscopic resection of the polyp, the thorough assessment of histological features is important to determine the possibility of residual tumor, the risk of recurrence, and the risk of lymph node involvement. The presence of high risk features (deep SMI, poor differentiation, LVI, <1 mm resection margin, piecemeal resection, tumor budding) indicates a need for surgical resection with lymph node clearance (if medically fit) in the majority of cases. In case of the MPs with low-risk features, the endoscopic resection is considered adequate and further surveillance is advised; when compared to surgery, endoscopic resection is less costly and associated with improved clinical outcomes and patient satisfaction. Moreover, the final decision about the endoscopic resection versus surgical resection of MP needs to be individualized and should be based not only on polyp related characteristics but also on comorbidities, local resources, expertise availability, and patient’s preference. The management of patients with MP requires a multidisciplinary team approach with the involvement of referring physicians, endoscopists, surgeons, pathologists, radiologists, and medical oncologists.
2.Mathews AA, Draganov PV, Yang D. Endoscopic management of colorectal polyps: From benign to malignant polyps.World Journal of Gastroenterology. 2021;13(9):356-370
3.Amin MB, Edge S, Greene F, Byrd DR, Brookland RK, Washington MK, et al. AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer; 2017. pp. 252-254
4.Hackelsberger A, Frühmorgen P, Weiler H, Heller T, Seeliger H, Junghanns K. Endoscopic polypectomy and management of colorectal adenomas with invasive carcinoma. Endoscopy. 1995;27:153-158
5.Netzer P, Forster C, Biral R, Ruchti C, Neuweiler J, Stauffer E, et al. Risk factor assessment of endoscopically removed malignant colorectal polyp. Gut. 1998;43:669-674
6.Coverlizza S, Risio M, Ferrari A, Fenoglio-Preiser CM, Rossini FP. Colorectal adenomas containing invasive carcinoma. Pathologic assessment of lymph node metastatic potential. Cancer. 1989;64:1937-1947
7.Tateishi Y, Nakanishi Y, Taniguchi H, Shimoda T, Umemura S. Pathological prognostic factors predicting lymph node metastasis in submucosal invasive (T1) colorectal carcinoma. Modern Pathology. 2010;23:1068-1072
8.Klimeck L, Heisser T, Hoffmeister M. Hermann Brenner colorectal cancer: A health and economic problem. Best Practice & Research Clinical Gastroenterology. 2023;2023:101839
9.Kuipers EJ, Rösch T, Bretthauer M. Colorectal cancer screening–optimizing current strategies and new directions. Nature Reviews. Clinical Oncology. 2013;10:130-142
10.Armaghany T, Wilson JD, Chu Q , Mills G. Genetic alterations in colorectal cancer. Gastrointestinal Cancer Research. 2012;5(1):19-27
11.Elisa De Palma FD, Pol J, Kroemer G, Maria Chiara Maiuri MC, Salvatore F. The molecular hallmarks of the serrated pathway in colorectal cancer. Cancer (Basel). 2019;11(7):1017
12.Labianca R, Nordlinger B, Beretta GD, Mosconi S, Mandalà M, Cervantes A, et al., editors. Early colon cancer:ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Annals of Oncology. 2013;24:vi64-vi72
13.Shaukat A, Kaltenbach T, Dominitz JA, Robertson DJ, Anderson JC, Cruise M, et al. Endoscopic recognition and management strategies for malignant colorectal polyps: Recommendations of the US multi-society task force on colorectal cancer. Gastroenterology. 2020;159:1916-1934
14.Teo NZ, Wijaya R, Ngu JC. Management of malignant colonic polyps. Journal of Gastrointestinal Oncology. 2020;11:469-474
15.Backes Y, Schwartz MP, Ter Borg F, Wolfhagen FHJ, Groen JN, et al. Multicentre prospective evaluation of real-time optical diagnosis of T1 colorectal cancer in large non-pedunculated colorectal polyps using narrow band imaging (the OPTICAL study). Gut. 2019;68:271-279
16.Rex DK, Shaukat A, Wallace MB. Optimal management of malignant polyps, from endoscopic assessment and resection to decisions about surgery. Clinical Gastroenterology and Hepatology. 2019;17:1428-1437
17.Waye JD, O’Brien MJ. Cancer in polyps. In: Cohen A, Winawer S, editors. Cancer of the Colon, Rectum and Anus. New York: McGraw-Hill; 1994. pp. 465-476
19.Cranley JP, Petras RE, Carey WD, et al. When is endoscopic polypectomy adequate therapy for colonic polyps containing invasive carcinoma? Gastroenterology. 1987;91:419-427
20.Rossini FP, Ferrari A, Coverlizza S, et al. Large bowel adenomas containing carcinoma: A diagnostic and therapeutic approach. International Journal of Colorectal Disease. 1988;3:47-52
21.Sugihara K, Muto T, Morioka Y. Management of patients with invasive carcinoma removed by colonoscopic polypectomy. Diseases of the Colon and Rectum. 1989;32:829-834
22.Williams CB, Whiteway JE, Jass JR. Practical aspects of endoscopic management of malignant polyps. Endoscopy. 1987;19:31-37
23.Christie JP. Polypectomy or colectomy? Management of 106 consecutively encountered colorectal polyps. The American Surgeon. 1988;54:93-99
24.Rembacken BJ, Fujii T, Cairns A, Dixon MF, Yoshida S, Chalmers DM, et al. Flat and depressed colonic neoplasms: A prospective study of 1000 colonoscopies in the UK. Lancet. 2000;355:1211-1214
25.Soetikno RM, Kaltenbach T, Rouse RV, Park W, Maheshwari A, Sato T, et al. Prevalence of nonpolypoid (flat and depressed) colorectal neoplasms in asymptomatic and symptomatic adults. Journal of the American Medical Association. 2008;299:1027-1035
26.Moss A, Bourke MJ, Williams SJ, Hourigan LF, Brown G, Tam W, et al. Endoscopic mucosal resection outcomes and prediction of submucosal cancer from advanced colonic mucosal neoplasia. Gastroenterology. 2011;140:1909-1918
27.Conteduca V, Sansonno D, Russi S, Dammacco F. Precancerous colorectal lesions (Review). International Journal of Oncology. 2013;43:973-984
28.Lopez A, Bouvier AM, Jooste V, Cottet V, Romain G, Faivre J, et al. Outcomes following polypectomy for malignant colorectal polyps are similar to those following surgery in the general population. Gut. 2019;68:111-117
29.Bogie RMM, Veldman MHJ, Snijders LARS, Winkens B, Kaltenbach T, Masclee AAM, et al. Endoscopic subtypes of colorectal laterally spreading tumors (LSTs) and the risk of submucosal invasion: A meta-analysis. Endoscopy. 2018;50:263-282
30.Burgess NG, Hourigan LF, Zanati SA, Brown GJ, Singh R, Williams SJ, et al. Risk stratification for covert invasive cancer among patients referred for colonic endoscopic mucosal resection: A Large Multicenter Cohort. Gastroenterology. 2017;153:732-742
31.Bettington M, Walker N, Clouston A, Brown I, Leggett B, Whitehall V. The serrated pathway to colorectal carcinoma:Current concepts and challenges. Histopathology. 2013;62:367-386
32.Puig I, López-Cerón M, Arnau A, et al. Accuracy of the narrow-band imaging international colorectal endoscopic classification system in identification of deep invasion in colorectal polyps. Gastroenterology. 2019;156:75-87
33.Shahidi N, Vosko S, van Hattem WA, Sidhu M, Bourke MJ. Optical evaluation:The crux for effective management of colorectal neoplasia. Therapeutic Advances in Gastroenterology. 2020;13:1756
34.Sano Y, Kobayashi M, Kozu T, et al. Development and clinical application of a narrow band imaging (NBI) system with built-in narrow-band RGB filters. Stomach Intestine. 2001;36:1283-1287
35.Sano Y. NBI story. Early Colorectal Cancer. 2007;11:91-92
36.Yasushi Sano Y, Shinji Tanaka S, Shin-ei Kudo S, Shoichi Saito S, Takahisa Matsuda T, Yoshiki Wada Y, et al. Narrow-band imaging (NBI) magnifying endoscopic classification of colorectal tumors proposed by the Japan. NBI Expert Team. 2016;28(5):526-533
37.Hewett DG, Kaltenbach T, Sano Y, et al. Validation of a simple classification system for endoscopic diagnosis of small colorectal polyps using narrow-band imaging. Gastroenterology. 2012;143:599-607
38.Iwatate M, Sano Y, Tanaka S, Kudo SE, Saito S, Matsuda T, et al. Japan NBI expert team (JNET) validation study for development of the Japan NBI expert team classification of colorectal lesions. Digestive Endoscopy. 2018;30:642-651
39.Kudo S, Hirota S, Nakajima T, Hosobe S, Kusaka H, Kobayashi T, et al. Colorectal tumours and pit pattern. Journal of Clinical Pathology. 1994;47:880-885
40.Ali SM, Uma S, Liu J, Li YQ , Zuo XL. Kudo’s pit pattern classification for colorectal neoplasms: A meta-analysis. World Journal of Gastroenterology. 2014;20(35):12649-12656
41.Togashi K, Konishi F, Ishizuka T, Sato T, Senba S, Kanazawa K. Efficacy of magnifying endoscopy in the differential diagnosis of neoplastic and non-neoplastic polyps of the large bowel. Diseases of the Colon and Rectum. 1999;42:1602-1608
42.Lui TKL, Wong KKY, Mak LLY, Ko MKL, Tsao SKK, Leung WK. Endoscopic prediction of deeply submucosal invasive carcinoma with use of artificial intelligence. Endoscopic International Open. 2019;7:E514-E520
43.Luo X, Wang J, Han Z, et al. Artificial intelligence-enhanced white-light colonoscopy with attention guidance predicts colorectal cancer invasion depth. Gastrointestinal Endoscopy. 2021;94:627-638
44.Kudo SE, Ichimasa K, Villard B, et al. Artificial intelligence system to determine risk of T1 colorectal cancer metastasis to lymph node. Gastroenterology. 2021;160:1075-1084
45.Haggitt RC, Glotzbach RE, Soffer EE, Wruble LD. Prognostic factors in colorectal carcinomas arising in adenomas: Implications for lesions removed by endoscopic polypectomy. Gastroenterology. 1985;89:328-336
46.Kikuchi R, Takano M, Takagi K, Fujimoto N, Nozaki R, Fujiyoshi T, et al. Management of early invasive colorectal cancer. Risk of recurrence and clinical guidelines. Diseases of the Colon and Rectum. 1995;38:1286-1295
47.Kitajima K, Fujimori T, Fujii S, Takeda J, Ohkura Y, Kawamata H, et al. Correlations between lymph node metastasis and depth of submucosal invasion in submucosal invasive colorectal carcinoma: A Japanese collaborative study. Journal of Gastroenterology. 2004;39:534-543
48.Nivatvongs S, Rojanasakul A, Reiman HM, Dozois RR, Wolff BG, Pemberton JH, et al. The risk of lymph node metastasis in colorectal polyps with invasive adenocarcinoma. Diseases of the Colon and Rectum. 1991;34:323-328
49.Beaton C, Twine CP, Williams GL, Radcliffe AG. Systematic review and meta-analysis of histopathological factors influencing the risk of lymph node metastasis in early colorectal cancer. Colorectal Disease. 2013;15:788-797
50.Toh EW, Brown P, Morris E, Botterill I, Quirke P. Area of submucosal invasion and width of invasion predicts lymph node metastasis in pT1 colorectal cancers. Diseases of the Colon and Rectum. 2015;58:393-400
51.Berg KB, Telford JJ, Gentile L, Schaeffer DF. Re-examining the 1-mm margin and submucosal depth of invasion:A review of 216 malignant colorectal polyps. Virchows Archiv. 2020;476:863-870
52.Hassan C, Zullo A, Risio M, Rossini FP, Morini S. Histologic risk factors and clinical outcome in colorectal malignant polyp: A pooled-data analysis. Diseases of the Colon and Rectum. 2005;48:1588-1596
53.Ueno H, Mochizuki H, Hashiguchi Y, Shimazaki H, Aida S, Hase K, et al. Risk factors for an adverse outcome in early invasive colorectal carcinoma. Gastroenterology. 2004;127:385-394
54.Cooper HS, Deppisch LM, Gourley WK, Kahn EI, Lev R, Manley PN, et al. Endoscopically removed malignant colorectal polyps:Clinicopathologic correlations. Gastroenterology. 1995;108:1657-1665
55.Boenicke L, Fein M, Sailer M, Isbert C, Germer CT, Thalheimer A. The concurrence of histologically positive resection margins and sessile morphology is an important risk factor for lymph node metastasis after complete endoscopic removal of malignant colorectal polyps. International Journal of Colorectal Disease. 2010;25:433-438
56.Brown IS, Bettington ML, Bettington A, Miller G, Rosty C. Adverse histological features in malignant colorectal polyps: A contemporary series of 239 cases. Journal of Clinical Pathology. 2016;69:292-299
57.Kuo E, Wang K, Liu X. A focused review on advances in risk stratification of malignant polyps. Gastroenterology Research. 2020;13:163-183
58.Egashira Y, Yoshida T, Hirata I, Hamamoto N, Akutagawa H, Takeshita A, et al. Analysis of pathological risk factors for lymph node metastasis of submucosal invasive colon cancer. Modern Pathology. 2004;17:503-511
59.Xu F, Xu J, Lou Z, Di M, Wang F, Hu H, et al. Micropapillary component in colorectal carcinoma is associated with lymph node metastasis in T1 and T2 stages and decreased survival time in TNM stages I and II. The American Journal of Surgical Pathology. 2009;33:1287-1292
60.Williams JG, Pullan RD, Hill J, Horgan PG, Salmo E, Buchanan GN, et al. Association of Coloproctology of Great Britain and Ireland. Management of the malignant colorectal polyp: ACPGBI position statement. Colorectal Disease. 2013;15:1-38
61.Watanabe T, Muro K, Ajioka Y, Hashiguchi Y, Ito Y, Saito Y, et al. Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2016 for the treatment of colorectal cancer. International Journal of Clinical Oncology. 2018;23:1-34
62.Aarons CB, Shanmugan S, Bleier JI. Management of malignant colon polyps:Current status and controversies. World Journal of Gastroenterology. 2014;20:16178-16183
63.Bartel MJ, Brahmbhatt BS, Wallace MB. Management of colorectal T1 carcinoma treated by endoscopic resection from the Western perspective. Digestive Endoscopy. 2016;28:330-341
64.Ciocalteu A, Gheonea DI, Saftoiu A, Streba L, Dragoescu NA, Tenea-Cojan TS. Current strategies for malignant pedunculated colorectal polyps. World Journal of Gastrointestinal Oncology. 2018;10:465-475
65.Fujiya M, Tanaka K, Dokoshi T, Tominaga M, Ueno N, Inaba Y, et al. Efficacy and adverse events of EMR and endoscopic submucosal dissection for the treatment of colon neoplasms: A meta-analysis of studies comparing EMR and endoscopic submucosal dissection. Gastrointestinal Endoscopy. 2015;81:583-595
66.Chandan S, Khan SR, Kumar A, Mohan BP, Ramai D, Kassab LL, et al. Efficacy and histologic accuracy of underwater versus conventional endoscopic mucosal resection for large (>20 mm) colorectal polyps: A comparative review and meta-analysis. Gastrointestinal Endoscopy. 2021;97(3):471-482
67.Yang D, Othman M, Draganov PV. Endoscopic mucosal resection vs endoscopic submucosal dissection for Barrett’s Esophagus and colorectal neoplasia. Clinical Gastroenterology and Hepatology. 2019;17:1019-1028
68.Hayashi N, Tanaka S, Hewett DG, Kaltenbach TR, Sano Y, Ponchon T, et al. Endoscopic prediction of deep submucosal invasive carcinoma: Validation of the narrow-band imaging international colorectal endoscopic (NICE) classification. Gastrointestinal Endoscopy. 2013;78:625-632
69.Rastogi A, Keighley J, Singh V, Callahan P, Bansal A, Wani S, et al. High accuracy of narrow band imaging without magnification for the real-time characterization of polyp histology and its comparison with high-definition white light colonoscopy: A prospective study. The American Journal of Gastroenterology. 2009;104:2422-2430
70.Backes Y, Elias SG, Groen JN, Schwartz MP, et al. Dutch T1 CRC working group. Histologic factors associated with need for surgery in patients with pedunculated T1 colorectal carcinomas. Gastroenterology. 2018;154:1647-1659
71.Saraivaa S, Rosaa I, Fonsecab R, Pereira AD. Colorectal malignant polyps: A modern approach. Annals of Gastroenterology. 2022;35(1):17-27
72.Vosko S, Bourke MJ. Gross morphology predicts the presence and pattern of invasive cancer in laterally spreading tumors: Don’t overlook the overview! Gastrointestinal Endoscopy. 2020;92:1095-1097
73.Ferlitsch M, Moss A, Hassan C, Bhandari P, Dumonceau JM, Paspatis G, et al. Colorectal polypectomy and endoscopic mucosal resection (EMR): European Society of Gastrointestinal Endoscopy (ESGE) clinical guideline. Endoscopy. 2017;49:270-297
74.Winawer SJ, Zauber AG, Fletcher RH, Stillman JS, O’Brien MJ, Levin B, et al. Guidelines for colonoscopy surveillance after polypectomy: A consensus update by the US multi-society task force on colorectal Cancer and the American Cancer Society. Gastroenterology. 2006;130:1872-1885
Written By
Umid Kumar Shrestha
Submitted: 06 September 2023Reviewed: 07 September 2023Published: 04 December 2023
 Open access peer-reviewed chapter
Open access peer-reviewed chapter