
Main food sources of vitamin E.
Abstract
Vitamin E (VE) is the main antioxidant of the cell membrane. Research has extensively explored the use of VE in preventing or treating diseases associated with oxidative stress in humans, with a particular emphasis on cardiovascular diseases (CVD). Studies suggest a range of effects beyond its well-established antioxidant action, including anti-inflammatory, immunomodulatory, lipid-lowering, anticoagulant, antidiabetic, and neuroprotective properties. Regarding the effects of VE on the prevention or treatment of CVD and cardiovascular outcomes, the studies showed conflicting results. The benefits of VE were suggested as: (1) the inverse association between increased intake of VE and the risk of stroke, (2) reduced CVD mortality rate, (3) increased glutathione and reduced C-reactive protein, malondialdehyde, LDL, and blood pressure, (4) lower risk of CVD and metabolic syndrome with higher intake of VE, and (5) lower systolic blood pressure. However, a positive association between VE supplementation and diastolic blood pressure was observed. Other adverse effects of VE supplementation have been suggested, such as an increased risk of hemorrhagic stroke and a small but significant increase in the risk of hospitalization in patients with heart failure. Therefore, it is not possible to recommend VE supplementation for the prevention and treatment of CVD.
Keywords
- vitamin E
- antioxidant
- oxidative stress
- atherosclerosis
- cardiovascular diseases
1. Introduction
Vitamin E, the primary fat-soluble vitamin in plasma, exists in four isoforms (alpha, beta, gamma, and delta-tocopherol), with alpha-tocopherol standing out as the most active and extensively studied biological form. This positioning within the lipid portion of cell membranes enables vitamin E to safeguard unsaturated phospholipids from lipid oxidation. Its protective mechanism involves the ability to convert free radicals into non-harmful metabolites by donating hydrogen [1].
The antioxidant properties of vitamin E have led to extensive research in various areas, including inflammation [1], immunomodulation [2], lipid profile [3], anticoagulant [4], antidiabetic [5], neuroprotective [6], and cardiovascular diseases [7], a leading global cause of death [8]. Atherosclerosis, an inflammatory disease caused by damage to the intimal layer resulting in chronic arterial lumen obstruction, forms the foundation for several cardiovascular diseases [9]. The oxidative process contributes to the progression of the inflammatory response. Reactive oxygen species [10] have also been linked to additional processes related to atherosclerosis, including increased vasoconstriction, angiogenesis, and apoptosis of endothelial cells.
In scientific literature, studies assessing the effects of vitamin E on the prevention or treatment of cardiovascular diseases and cardiovascular outcomes in humans have been carried out and the results suggest that this vitamin is associated with a lower stroke risk, could reduce the incidence of cardiovascular events and may improve cardiometabolic health in patients with diabetes [7, 11, 12, 13, 14, 15, 16, 17, 18, 19]. However, vitamin E was associated with significant increase in the risk of heart failure hospitalization [20]. In this chapter, the physiological aspects, food sources, nutritional deficiency and the effects of vitamin E on human health were addressed, with an emphasis on cardiovascular diseases.
1.1 Chemical composition, food sources, and nutritional deficiency
In recent years, important metabolic aspects of vitamin E have been identified, as well as antioxidant, anticholesterolemic, anti-inflammatory, anticancer, neuroprotective, and cardioprotective properties [21, 22].
Vitamin E exists in eight lipophilic natural forms, including α-, β-, γ-, and δ-tocopherol (αT, βT, γT, δT) and α-, β-, γ-, and δ-tocotrienol (αTE, βTE, γTE, δTE). Different isoforms of tocopherols and tocotrienols differ in the 5 or 7 position of the chromanol ring with an H or CH3 group. All tocopherols and tocotrienols are potent antioxidants with lipoperoxyl radical-scavenging activities (Figure 1) [1].
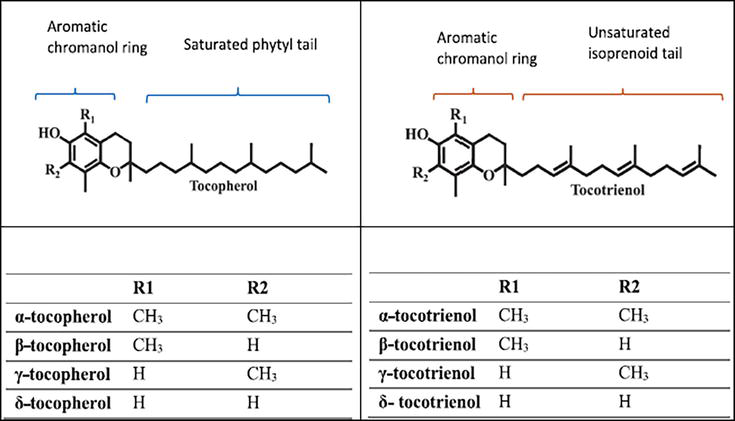
Figure 1.
Chemical structure of vitamin E. Adapted from: Zainal et al., 2022 [
Tocopherols and tocotrienols are present in various vegetable oils (palm oil, rice bran oil, and annatto) and grains (wheat, oats, barley, rice, and rye) [1]. Palm oil contains a healthy balance of saturated and unsaturated fats, including monounsaturated oleic acid (40%), polyunsaturated linoleic acid (10%), saturated palmitic acid (44%), as well as stearic acid (6%) [23]. There is no indication that palm oil consumption has any particular impact on health compared to other fats rich in saturated fatty acids [24, 25]. Edible oils are the main sources of tocotrienols, such as palm oil, rice bran oil, grape seed oil, and cranberry seed oil. Food sources of tocotrienols are barley, wheat, and annatto [26, 27].
Table 1 below shows the amount of vitamin E (in milligrams) per 100 grams or 100 mL of food, in descending order.
| Food (100 g /100 mL) | Amount of vitamin E (mg) |
|---|---|
| Hazelnut oil | 47.2 |
| Sunflower oil | 41.08 |
| Almond oil | 39.2 |
| Roasted sunflower seeds | 38.33 |
| Roasted sesame seeds | 36.33 |
| Safflower oil | 34.1 |
| Almond | 23.75 |
| Hazelnut | 23 |
| Canola oil | 17.46 |
| Peanut oil | 15.69 |
| Corn oil | 14.3 |
| Olive oil | 11.42 |
| Soybean oil | 8.18 |
| Brazil nuts | 7.14 |
| Peanut / Groundnuts | 6.94 |
| Palm oil | 3.81 |
| Egg yolk | 2.58 |
| Avocado | 2.07 |
| Walnuts | 1.8 |
| Sesame oil | 1.4 |
| Cashew nuts | 0.92 |
| Linseed oil | 0.71 |
| Coconut oil | 0.09 |
Table 1.
Source: Food Composition Table. Adapted from: Departamento de Informática em Saúde. Escola Paulista de Medicina. Universidade Federal de São Paulo. [Internet]. http://tabnut.dis.epm.br/alimento [28].
For more detail, Siger & Górnaś [27] checked the tocopherol (T) and tocotrienol (T3) profiles in four hundred and eighteen vegetable oil samples, of which fifteen species were dominated by tocotrienols, while sixty-seven by tocopherols. A relationship was observed between the taxonomic origin of the plant and the presence of the characteristic tocochromanol profile in the oils obtained from these plants [27].
Tocotrienol is generally highly lipophilic and to be absorbed by enterocytes requires lipolysis into micelles [29]. The presence of food has been shown to increase the absorption of tocotrienols by at least 1.5 times in fed human compared to those in a fasted state [30]. Alpha-tocotrienol recorded the highest absolute bioavailability, followed by γ- and δ-tocotrienol. In humans α-tocotrienol was the most abundant vitamin detected in plasma and lipoproteins following consumption of a single dose of tocotrienol-rich vitamin E from palm oil (70% tocotrienols, 30% tocopherol) [31].
Tocotrienols exhibit excellent biological activities. Tocopherols and tocotrienols differ by the presence of saturated and unsaturated isoprenoid side chains, respectively. To allow for greater fluidity and uniform distribution in the phospholipid bilayer. In addition, α-tocopherol is preferentially retained by body tissues via the α-tocopherol transfer protein (α-TTP), but tocotrienols are rapidly degraded into short-chain carboxychromanols to be more efficient in eliminating peroxyl radicals due to more effective interaction in membrane environments. However, clinical evidence on the effects of palm oil use on diseases such as cancer and cardiovascular diseases is insufficient [6].
The human body is unable to produce vitamin E, and its deficiency manifests obvious symptoms. Insufficiency of Vitamin E can be caused by factors such as a lack of fat absorption or protein malnutrition, among others [32].
1.2 Regulation of metabolism and excretion of vitamin E
In the intestine, tocopherols and tocotrienols from the diet appear to be absorbed in a similar way along with dietary fat and are secreted in chylomicron particles along with triacylglycerol, phospholipids, and cholesterol. Vitamin E bound to chylomicrons is transported via the lymphatic system to muscles, bone marrow, adipose tissue, skin, and brain. In these tissues, the vitamin E forms are taken up by a process mediated by lipoprotein receptors that is not well understood [33].
In the liver, αT is preferentially bound to the α-tocopherol transfer protein (α-TTP). Together with the ATP-binding cassette transporter ABCA1 (also known as the cholesterol efflux regulatory protein, an important regulator of cellular cholesterol and phospholipid homeostasis), α-TTP incorporates αT into lipoproteins that trans-transport to other tissues via the circulation. In contrast to the high affinity of αT (100%), α-TTP has a much lower affinity compared to 50, 10–30 or 1% affinity for βT, γT, and δT, respectively. Large portions of non-αT forms are catabolized in the liver via ω-hydroxylation initiated by cytochrome P450 (CYP4F2) and oxidation followed by β-oxidation of the phytyl chain to generate -hydroxychromanol (130-OH), various carboxychromanols and the terminal metabolite 30-carboxychromanol (30-COOH) or (20-carbox-ethyl)-6-hydroxychromans (CEHCs). Conjugation such as sulfation and glucuronidation of the phenolic on chromanol can occur in parallel with β-oxidation when there is a high intake of vitamin E forms [33].
In addition, protein control, absorption, and excretion of vitamin E may also play a role in its bioavailability. Cytochrome P450-mediated hydroxylation and oxidation of the side chain are responsible for initiating vitamin E catabolism. The activity of tocopherol-ω-hydroxylase is associated with CYP4F2, but not with other isoforms, including CYP3A. CYP4F2, a microsomal ω-hydroxylase, was initially described to metabolize leukotriene B4 via ω-hydroxylation [17]. ω-hydroxylase helps explain some aspects related to the bioavailability of vitamin E. For example, αT supplementation depletes plasma and tissue γT. This observation is probably partly explained by the preference of α-TTP affinity for αT, as increased αT can compete with γT in TTP binding and therefore leaves more γT for catabolism by hydroxylases. Meanwhile, increased αT intake can stimulate γT catabolism due to its effector activity towards CYP4F2 [2].
Lithocholic acid is oxidized at the C-3 position by human cytochrome P450 3A (CYP3A) to form 3-ketocholic acid, and this metabolite is cytotoxic in human intestinal and liver cells. α-Tocotrienol, γ-tocotrienol, δ-tocotrienol and a vitamin E mixture rich in tocotrienol, but not α-tocopherol, differentially inhibited the 3-oxidation of lithocholic acid catalyzed by liver and intestinal microsomes and recombinant CYP3A4 and CYP3A5 [2].
Tocotrienols can be found in the plasma 4 hours after use and have a reduced half-life in circulation, while those of α- and γ-Tocopherols were 57 and 13 h. However, tocotrienols are more effective despite lower bioavailability and absorption, and their deposition takes place in adipose tissue and the heart, in the metabolism in the liver, or the crossing of the blood-brain barrier. Tocotrienols have strong therapeutic properties but require accessibility to target organs [33].
The excretion of vitamin E and its metabolites also influences the tissue retention of these compounds. Short-chain carboxychromanols and their sulfated derivatives or glucuronidated homologs are excreted in the urine, while unconjugated carboxychromanols are found mainly in the feces. Bardowell et al. [34] estimated that up to 80% of the total metabolites were excreted in the feces, and unmetabolized tocopherols and tocotrienols are also eliminated by biliary excretion. Interestingly, fecal excretion of γT and δT is markedly increased in response to their supplementation, which probably prevents excessive accumulation of these tocopherols [34].
1.3 Antioxidant function
Vitamin E is one of the most important essential vitamins for supporting the regulation of oxidative stress in humans. All forms of vitamin E are potent antioxidants, as they eliminate peroxyl lipid radicals by donating hydrogen from the phenolic group on the chromanol ring. On the other hand, tocotrienols have been suggested to be better than αT at scavenging peroxyl radicals due to a more even distribution of tocotrienols in the phospholipid bilayer and more effective interaction with peroxyl radicals than tocopherols in membrane environments [35].
Inflammation, physical and mental stress, cigarette smoke, air pollutants, and chemical additives such as dyes and acidulants, among others, increase the generation of free radicals in the body [36]. Free radicals (FR) are considered destructive because they alter cell membranes, enzymes, and DNA. Free radicals and the intensity of chronic inflammation promote aging and various chronic diseases such as neurodegenerative and cardiovascular diseases [35].
Oxidative stress also increases under unbalanced levels of free radicals and antioxidants. It has been suggested that natural antioxidants may be beneficial to human health [37]. Among these, vitamin E stands out because it is a natural compound and has strong antioxidant activity, inhibiting lipid peroxidation and the generation of reactive oxygen species (ROS) [38].
The chromanol ring of tocotrienols plays a fundamental role in reducing methylation, highlighting the ease with which this molecule can be incorporated into cell membranes, and because of this tocotrienols are 40–60 times more effective than α-tocopherol in inhibiting the generation of pro-inflammatory cytokines. Among tocotrienols, γ tocotrienols and δ tocotrienols are supposedly more efficient at eliminating peroxyl radicals [39]. Tocotrienols are part of the vitamin E family. The potential of tocotrienols as a nutraceutical ingredient is largely underestimated due to low oral bioavailability, which is a common problem associated with fat-soluble bioactive compounds.
Fu et al. [39] showed that nanoencapsulation technology offers innovative solutions to improve the delivery mechanisms of these compounds and found that both nanovesicles (NV-T3) and solid lipid nanoparticles (NP-T3) showed increased accumulation in the kidneys and liver (5-fold) compared to the control group, while selectivity for α-tocotrienol was evident for NP-T3. In the brain and liver of rats that received NP-T3, α-tocotrienol emerged as the dominant congener (>80%). Acute oral administration of nanoencapsulated tocotrienols showed no signs of toxicity. The study concluded greater bioavailability and selective accumulation of tocotrienol congeners in tissues when delivered via nanoencapsulation.
1.4 Anti-inflammatory function
Inflammation is characterized by the production of a plethora of reactive oxygen and nitrogen species and pro-inflammatory mediators, including lipid mediators, notably prostaglandins and leukotrienes, and cytokines such as TNF-α and interleukin-6 (IL-6) which, in turn, aggravate inflammation and lead to excessive damage to host tissues. Prostaglandins and leukotrienes play important roles in mediating the inflammation response. For example, prostaglandin E2 (PGE2), which is produced from the oxidation of AA catalyzed by COX-1 and COX-2, causes pain and fever, besides activating the formation of cytokines. Leukotriene B4 (LTB4), another lipid mediator derived from AA through the reaction catalyzed by 5-lipoxygenase (5-LOX) in neutrophils, is one of the most potent chemotactic agents. Due to the central roles of PGE2 and LTB4 in inflammation, COXs, and 5-LOX have been recognized as key targets for drug therapy against chronic diseases [6].
Tocotrienols exhibit superior anti-inflammatory efficacy compared to tocopherols and a lack of adverse effects [6]. γTocopherol, δTocopherol, and γTocotrienol strongly inhibited A23187-stimulated LTB4 and LTC4-like human neutrophils isolated from peripheral blood, while αT was much less effective. Jiang et al. [40] showed that different forms of vitamin E partially inhibited COX-2-mediated PGD2 and PGE2 formation in lipopolysaccharide (LPS)-stimulated RAW264.7 macrophages and IL-1β-activated lung epithelial cells, respectively, with a potency ratio of δT AND γTE 4 γT ⪢ αT. Although γT, δT, and γTE had no effect on endotoxin- or cytokine-stimulated COX-2 up-regulation, they suppressed COX-2 activity in cellular environments. On the other hand, none of these forms of vitamin E appeared to inhibit purified COX-2 activity. These results support the notion that forms of vitamin E are weak at inhibiting COX-2 tors, such as salicylic acid and paracetamol, both of which inhibit PGE2 in intact cells, but show weak inhibition of purified COXs (Figure 2) [40, 42, 43, 44].
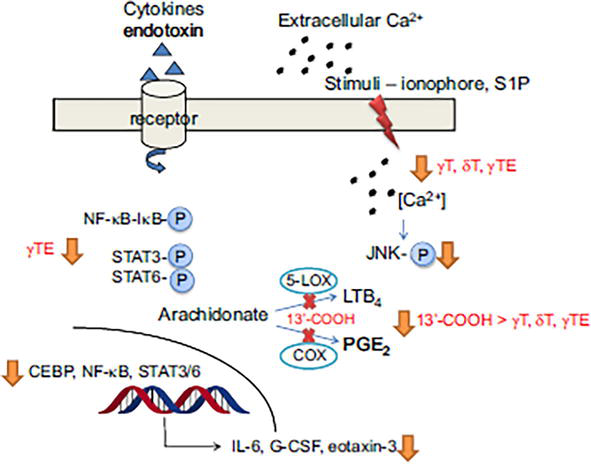
Figure 2.
Anti-inflammatory activities of vitamin E. In epithelial cells, macrophages, and neutrophils, γT, δT, and γTE modestly inhibit PGE2 and LTB4 without inhibiting COX and 5-LOXactivity. 130-COOH spotently inhibit COX-1/COX-2 and 5-LOX enzyme activity (redcrosses). In neutrophils, vitamin forms suppress ionophore-orS1P (sphingosine1-phos-phate)-stimulated calcium influx and its downstream signaling. In macrophages and lung epithelial cells, γTE inhibits activation of NF-κB and STAT6/3 as well as their regulated genes, including cytokines and chemokines. Adapted from: Jiang, Q, 2014 [
Over the last 20 years, research into vitamin E has focused mainly on αT and its antioxidant effects, and much more recently (in the last 10 years), the focus of vitamin E research has been on investigating different tocopherols and tocotrienols, their metabolism, and their non-antioxidant activities. But αT supplementation has failed to provide consistent benefits for the prevention of chronic diseases, including cancer and cardiovascular diseases, in many large clinical intervention studies [45, 46, 47, 48].
One explanation is that αT may be beneficial for individuals deficient in αT and/or other micronutrients, which may be caused by low dietary intake of this vitamin E or αT depletion due to pathologies, smoking, alcoholism, and malabsorption. In these subclinical conditions, αT supplementation is likely to be beneficial [48].
γ-tocopherol (γT) is the second most abundant form of vitamin E in blood and tissues, while α-tocopherol (αT) is the predominant vitamin E in tissues. Research has revealed that γT has unique antioxidant and anti-inflammatory activities relevant to disease prevention compared to αT. Although both compounds are potent lipophilic antioxidants, γT, but not αT, can capture reactive nitrogen species forming 5-nitro-γT, and appears to show superior protection of function in mitochondria. γT inhibits ionophore-stimulated leukotrienes by blocking the translocation of 5-lipoxygenase (5-LOX) in leukocytes, decreases prostaglandins catalyzed by cyclooxygenase-2 (COX-2) in macrophages and blocks the growth of cancer cells, but not healthy cells. For these activities, γT is stronger than αT. In addition, γT is more extensively metabolized than αT via side-chain oxidation initiated by cytochrome P-450 (CYP4F2), which leads to the formation of metabolites including 13′-carboxychromanol (13′-COOH) and carboxyethylhydroxychroman (γ-CEHC). 13’-COOH and γ-CEHC are the predominant metabolites found in feces and urine, respectively. Interestingly, γ-CEHC has natriuretic activity and 13′-COOH inhibits COX-1/−2 and 5-LOX activity. Consistent with these mechanistic findings of γT and metabolites, studies show that γT supplementation attenuates inflammation and disease symptoms in animal models with induced inflammation, asthma, and cancer. In addition, γT supplementation decreased inflammation markers in patients with kidney disease and mild asthma. These observations support that γT may be useful against diseases associated with inflammation [41, 49, 50].
Findings have provided mechanistic insights into the role of γT in the prevention and management of diseases observed in animal and human studies, as seen in a recent review, in which Jiang et al. [51] that γT is shown to be superior to αT in detoxifying nitrogen dioxide (NO2), peroxynitrite (ONOO-), and copper-zinc superoxide dismutase (SOD)/H2O2/NO2-, via the formation of 5-NγT. Consistently, 5-NγT was elevated in zymosan-induced-peritonitis in rats and during FeCl3 patch-induced occlusive thrombus formation in rats. Supplementation of pharmaceutical doses of γT (∼1200 mg) temporarily increases this vitamin E in the plasma to up to 30–40 μM.
Below is a Table 2 of the bioactivities of γT and metabolites, adapted from the above-mentioned review.
| Activities in cells or animal models Mechanisms | ||
|---|---|---|
| Activity of γT; Comparing γT and αT |
|
|
| 13′ -COOH |
|
|
| γ-CEHC |
|
|
Table 2.
Bioactivities of γT and metabolites.
Adapted from: Q. Jiang, Metabolism of natural forms of vitamin E and biological actions of vitamin E metabolites, Free Radic Biol Med 179 (2022) 375–387 [51].
1.5 Immunomodulatory function
In the adaptive immune system, Th17 cells have pro-inflammatory properties, while Treg cells have negative immunoregulatory effects. The Th17/Treg balance plays an important role in the treatment of autoimmune diseases [52]. Th17 differentiation is regulated by the cytokine IL-6 via the JAK/STAT3 signaling pathway. In the IL-6/JAK/STAT3 signaling pathway, IL-6 binds to the membrane receptors IL-6Rα and gp130 (IL-6Rβ) to regulate JAK activation. JAK induces STAT3 that combines with another STAT3 protein to form a phosphorylated dimer. Finally, the dimer enters the nucleus and activates transcription factors involved in Th17 differentiation [53].
The role of γ-Tocotrienol in the differentiation and function of T helper 17 (Th17)/regulatory (Treg) cells is not fully understood. However,
In addition, γ-Tocotrienol can inhibit nuclear factor kappa B (NF-κB) signaling via positively regulating A20 protein expression [17]. And γ-Tocotrienol inhibits lipopolysaccharide-induced IL-6, tumor necrosis factor alpha, granulocyte-macrophage colony-stimulating factor, and other pro-inflammatory cytokines [55].
1.6 Hypolipidemic effect
Tocotrienols have shown hypolipidemic, as well as atherogenic and nephroprotective effects since hyperlipidemia is intrinsically connected to oxidative stress leading to cardiovascular dysfunction, atherosclerosis, and progressive chronic renal dysfunction [3, 56, 57].
Tocotrienols can inhibit the action of hepatic hydroxy-methylglutaryl coenzyme A (HMG-CoA) reductase, the enzyme responsible for cholesterol biosynthesis, which has been attributed to their lipid-lowering properties that reduce cholesterol production. This activity has been demonstrated in experimental and clinical studies by several researchers [3, 58].
In experimental studies, atherosclerotic animals supplemented with tocotrienols observed a reduction in serum levels of vascular cell adhesion protein-1 (VCAM-1), IL-6, and matrix metalloproteinase-12 (MMP-12) and LDL cholesterol [59, 60].
1.7 Anti-coagulant function
T3 can act as an anticoagulant, thereby delaying the progression of atherosclerosis and reducing total plasma triglycerides (TG) and apolipoprotein-A1 (Apo-A1) [4]. Oxidative stress, as described in [61], induces inflammation and endothelial damage. T3 exerts beneficial effects on serum LDL, CRP, ApoB, and glycation end products. Simultaneously, it increases HDL levels, collectively reducing the risk of developing atherosclerosis.
1.8 Tocotrienols as an anti-diabetic agent
Diabetes is a chronic disease that impairs the body’s ability to produce or use insulin properly [55]. After most food is converted into glucose and absorbed, insulin is released in response to an increase in blood glucose [62].
Clinical and experimental investigations have shown that T3 supplementation can help reduce the risk of diabetes and mitigate associated conditions such as brain health care, nerve pain relief, preventive eye care, and kidney well-being. Due to this, it is considered an antihyperglycemic agent [5, 63].
1.9 Vitamin E as a neuroprotector
Tocotrienols have been investigated as nutraceuticals, particularly in the context of metabolic diseases and degenerative conditions [6]. In recent years, clinical studies on the neuroprotective effect of tocotrienols have gained significant results. Supplementation for up to 12 months, as reported in [source], has been shown to reduce white matter lesion volume and alleviate pain in diabetic patients with peripheral neuropathy [64, 65]. These clinical benefits have been attributed mainly to the antioxidant and anti-inflammatory mechanisms of tocotrienols [64, 65].
Alcoholism affects around 2 billion people worldwide. Withdrawal causes a neuroinflammatory response which increases anxiety. Villas Boas et al. [66] conducted a study with male Wistar rats divided into four groups and subjected to a forced and chronic rehabilitation procedure, involving a liquid diet containing 6 and 8% ethanol for 15 days, followed by an abrupt interruption of treatment. The results showed that α-tocopherol showed anxiolytic action and anti-inflammatory activity, attenuating the anxious behavior of abstinent animals and reducing neuroinflammation in amygdaloid nuclei (AN) and medial hypothalamic nucleus (mHN); and the intensity of the anxiolytic and anti-inflammatory effect of α-tocopherol is dose-dependent. [66].
Toxicological evaluation is critical and has been tested for safety in experimental tests. One of the known side effects of tocopherols is the modification of vitamin K’s function in blood coagulation. However,
According to Fu et al. [53], T3 supplementation at 400 mg/day for 14 days did not affect hematotoxicity or hepatotoxicity in individuals with metabolic diseases. In addition, the Institute of Medicine suggests taking 200–1000 mg of vitamin E per day which can only be obtained through supplementation.
The recommended dietary intake of vitamin E (α-Toc) is around 15 mg per day. In addition, the Food and Drug Administration (FDA) has recommended tocotrienol intake of 13 to 20 mg per day from food. Tocotrienol supplementation has proven to be safe and acceptable in >30 clinical trials with varying dosages of tocotrienol in various formulations and study demographics [68].
More clinical trials investigating the potential use of tocopherols, tocotrienols, and combinations must be carried out to ensure effective treatments from this important vitamin.
Advertisement
2. Vitamin E in cardiovascular diseases
Cardiovascular diseases (CVD) represent a major cause of death worldwide [8].
When serum LDL concentrations rise, this lipoprotein is deposited in the arteries, resulting in oxidation and the formation of oxidized LDL (LDL-ox), which attacks endothelial cells that start expressing various molecules (intercellular adhesion molecule, E-selectin, vascular adhesion molecule, and interleukin-8) that act to recruit and bring neutrophils into the tunica media of the vessels. LDL-ox itself is chemotactic for monocytes. This process increases the inflammatory response, promoting the migration of monocytes to the tunica intima and their differentiation into macrophages that phagocytize LDL-ox, transforming it into foam cells. These cells are components of atherosclerotic plaques which, in more advanced stages, develop into fibrous plaques that impair blood flow, resulting in necrosis [9].
LDL-ox phagocytosis is characterized by the increased production of digestive proteases by macrophages and an increase in reactive oxygen species [9]. Oxidative stress is one of the most important factors involved in atherosclerosis and its complications [69]. The oxidative process favors the progression of the inflammatory response, making the damage more complex and triggering clinical manifestations such as
Controlling dyslipidemia and inflammation and protecting the vascular endothelium should be part of the treatment of atherosclerosis. Lifestyle changes are the main determinants of CVD prevention, including diet, which can influence atherogenesis directly or through changes in classic risk factors (blood pressure, blood glucose, and serum lipids) [70].
Considering the role of LDL-ox in the atherosclerotic process, the use of antioxidants such as vitamin E (VE) has aroused the interest of researchers. This interest is due to the anti-atherogenic mechanisms that have been attributed to VE (Table 3).
| Remove peroxyl radicals, interrupting the chain of lipidic peroxidation; |
| Protect the polyunsaturated fatty acids from damage by free radicals; |
| Protect circulating lipoproteins; |
| Act in the proper functioning of the cell membranes; |
| Increase the resistance of LDL to oxidation; |
| Reduce platelet adhesion and aggregation; |
| Inhibit vitamin K-dependent coagulation factors; |
| Stimulate endothelin production; |
| Attenuate the inhibition of nitric oxide production mediated by LDL-ox; |
| Inhibit the secretion of interleukin-1 by monocytes by inhibiting protein kinase C; |
| Influence the vasodilator function of the arteries. |
Table 3.
VE antiatherogenic mechanisms.
Adapted from M. Batlouni, Hipótese oxidativa da aterosclerose e emprego dos antioxidantes na doença arterial coronária, Arq Bras Cardiol 68 (1) (1997) 55–63 [10].
In an attempt to answer the question: “
| Authors/year | Objective | Total/Type of the study | Characteristics of the studies | Quality of the studies | Results | Limitations |
|---|---|---|---|---|---|---|
| Cheng et al. [11] |
|
|
|
|
|
|
| Machado et al. [15] |
|
|
|
|
|
|
| Han et al. [13] |
|
|
|
|
|
|
| Khan et al. [20] |
|
|
|
|
|
|
| Shah et al. [16] |
|
|
|
|
|
|
| Hamedi-Kalajahi et al. [17] |
|
|
|
|
|
|
| Li et al. [12] |
|
|
|
|
|
|
| O’Connor et al. [18] |
|
|
|
|
|
|
| An et al. [14] |
|
|
|
|
|
|
| Dludla et al. [19] |
|
|
|
|
|
|
| Zhang et al. [7] |
|
|
|
|
|
Table 4.
Characteristics of the studies and main findings on the effect of vitamin E on cardiovascular health.
BP, lipid profile, glycemia, all-cause mortality, cardiovascular mortality, AMI, stroke, CAD, arrhythmia and DM2.
PUFA of the n-3 series, PUFA of the n-6 series, PUFA of the n-9 series, hesperidin, L-arginine, L-citrulline, VB9, VC, VD, VE, Mg, Zn, α-lipoic acid, coQ10, lycopene, Se, Mg, Zn, anthocyanin, quercetin, resveratrol, isoflavones, flavonoids, melatonin, catechin, curcumin, flavanol and genistein.
Cancer (breast, lung, esophagus, stomach, pancreas, kidney, bladder, cervical, glioma, thyroid, colorectal, endometrium, ovary, non-Hodking lymphoma), total cancer and cancer mortality.
CVD, Parkinson’s disease, depression, age-related cataracts, metabolic syndrome, fractures, stroke, anxiety, glaucoma, obesity and all-cause mortality.
VE (vitamin E), AVC (cerebrovascular accident, stroke), MA (meta-analysis), VA (vitamin A), CSOS (cross-sectional observational studies), RCTs (randomized controlled trials), CRF (coronary risk factor), Mg (magnesium), Zn (zinc), vitamin C (vitamin C), CAC (coronary artery calcification), FFQ (food frequency questionnaire), CVD (cardiovascular disease), SR (systematic review), VB6 (vitamin B6), VB9 (vitamin B9), VB12 (vitamin B12), VD (vitamin D), HF (heart failure), PUFA (polyunsaturated fatty acid), CoQ10 (coenzyme Q10), ↓ (reduction), SAH (systemic arterial hypertension), BP (blood pressure), AMI (acute myocardial infarction), CAD (coronary artery disease), LDL (low-density lipoprotein), DM2 (type 2 diabetes mellitus), CKD (chronic kidney disease), apo (apolipoprotein), HD (hemodialysis), BW (body weight), BMI (body mass index), WC (waist circumference), MDA (malondialdehyde), IL-6 (interleukin-6), HbA1C (glycated hemoglobin), ALT (alanine aminotransferase), AST (aspartate aminotransferase), TNF-α (tumor necrosis factor alpha), SBP (systolic blood pressure), DBP (diastolic blood pressure), VB3 (vitamin B3), Se (selenium), GSH (glutathione), CRP (C-reactive protein), RR (relative risk), CI (confidence interval), OR (odds ratio), MD (mean differences), SMD (standardized mean difference), ARD (absolute risk difference) and HR (hazard ratio).
The literature surveyed shows conflicting results (benefits, adverse effects, and no effect) regarding the effects of VE on the prevention or treatment of CVD and cardiovascular outcomes. In 5 studies, the benefits of VE were suggested as: (1) the inverse association between increased intake of VE (diet, supplement, or combination) and the risk of stroke [11], (2) reduced CVD mortality rate with VE supplementation [13], and (3) lower systolic blood pressure with VE supplementation [12]. A recent SR showed that VE may improve cardiometabolic healthy by increasing glutathione levels, reducing C-reactive protein, malondialdehyde and LDL levels and controlling blood pressure [19]. A recent umbrella review suggests a lower risk of CVD and metabolic syndrome with higher intake of VE (diet, supplementation or combination) [7].
It is worth noting that, in the MA by Li et al. [12], a positive association between VE supplementation and DBP was found by unknown mechanisms. Other adverse effects of VE supplementation have been suggested, such as an increased risk of hemorrhagic stroke [18] and a small but significant increase in the risk of hospitalization in patients with heart failure (HF) [20]. When offered in high doses, VE starts to act as a pro-oxidant, generating oxidative stress that worsens HF [71], which could explain the increased risk of hospitalization in HF patients.
In the SR by Shah et al. [16], Asian studies showed a significant positive association between serum delta-tocopherol [72] and gamma-tocopherol [73] and increased risk for AMI and increased mortality from hemorrhagic stroke (in women), respectively. In these studies, the authors showed no effect of serum alpha-tocopherol and gamma-tocopherol for AMI [72] and reduced mortality from hemorrhagic stroke [73] for alpha-tocopherol. Another interesting finding is that in the study by Nagao et al. [73], serum gamma-tocopherol was associated with lower stroke mortality in men. These results suggest the influence of VE isoform and gender on cardiovascular outcomes.
There was no effect of VE on CVD prevention and cardiovascular mortality [16, 18], anthropometry and cardiometabolic indices (except blood pressure) [12], CVD and DM2 [14] and serum concentrations of apo A-1 and apo B-100 [17]. Although it did not influence apo A-1 and apo B-100 concentrations, VE was associated with a reduction in LDL-ox concentrations in dialysis patients [74] and diabetics [75], contributing to a reduction in the atherogenic process. In their SR, Machado et al. [15] found that the relationship between VE and coronary artery calcification (CAC), a risk factor for atherosclerosis, coronary events, and cardiovascular mortality, is controversial, with reports of no association [76, 77] or a positive association between VE intake and CAC [78, 79].
Two SRs evaluated the effect of antioxidant supplements alone or in combination on the prevention of CVD [13, 18] and cancer [18]. The use of combined antioxidants was found to have little or no advantage over antioxidants alone. A small reduction in cancer incidence with combined antioxidants was observed in healthy adults without micronutrient deficiencies [18].
Several factors may explain the discrepancy between the studies. In the MA by Khan et al. [20], the quality of the evidence and studies was considered low. In the MA of Li et al. [12], 47.1% of the studies were considered inconsistent. In the umbrella review by Zhang et al. [7], most of the evidence was low (47.1%) or very low (44.1%). In addition, the VE isoform tested was not identified in most studies. Only 2 studies [7, 17] identified the isoform (alpha) of the supplement. Asian results suggest the influence of the VE isoform on cardiovascular outcomes [72, 73]. The characteristics of the participants should also be considered. For example, in the SR of O’Connor et al. [18], where VE supplementation was associated with an increased risk of hemorrhagic stroke, in 55.5% of studies, women were the majority, aged between 55 and 66 years and the frequency of smokers ranged from 2–100%. Smoking is one of the independent risk factors for stroke [80]. All studies had limitations, such as the small number of studies, sample size, language of the articles, follow-up period, and supplement dose. Thus, caution is needed in interpreting the results.
The amount of VE intake associated with a given effect was not clearly specified by the studies, except for Cheng et al. [11] who suggested a dietary VE intake between 15 to 39.45 mg/day for stroke prevention. Bell & Grochoski [81] suggested that healthy individuals should not use VE supplements in amounts greater than 1000 mg/day and complement it, stating that daily VE intake of up to 800 IU appears to be safe and beneficial. Daily VE intake between 400 and 800 IU appears to reduce the risk for several diseases, including CVDs, in healthy individuals [81].
It is worth noting that VE can promote the degradation of drugs used in the treatment of cancer, CVD, SAH, or DM [7]. In addition, it has been suggested that VE doses above 300 mg/day may interfere with the action of tamoxifen, cyclosporine, aspirin, or warfarin [82]. The drug-VE interaction should be considered when interpreting the results.
Advertisement
3. Conclusion
Therefore, recommending VE supplementation for CVD prevention and treatment is not feasible due to the lack of consensus on dosage, duration, patient profiles benefiting from supplementation, efficacy of combined antioxidant supplements, and potential adverse effects. Further studies, characterized by good methodological rigor and evidence quality, are necessary to provide clarity on these uncertainties. Hence, prioritizing a diet abundant in fruits, vegetables, whole grains, seeds, oilseeds, and moderate amounts of vegetable oils is recommended for obtaining antioxidant nutrients. This emphasis on dietary sources is preferred over relying on antioxidant supplements, whether isolated or combined.
References
- 1.
Jiang Q. Natural forms of vitamin E: Metabolism, antioxidant, and anti-inflammatory activities and their role in disease prevention and therapy. Free Radical Biology & Medicine. 2014; 72 :76-90 - 2.
Wong SY, Teo JSM, Chai SF, Yeap SL, Lau AJ. Vitamin E analogues differentially inhibit human cytochrome P450 3A (CYP3A)-mediated oxidative metabolism of lithocholic acid: Impact of δ-tocotrienol on lithocholic acid cytotoxicity. Toxicology. 2019; 423 :62-74 - 3.
Cheng HS, Ton SH, Tan JBL, Kadir KA. The ameliorative effects of a tocotrienol-rich fraction on the AGE-RAGE axis and hypertension in high-fat-diet-fed rats with metabolic syndrome. Nutrients. 2017; 9 :984 - 4.
Prasad KN, Edwards-Prasad J. Vitamin E and cancer prevention: Recent advances and future potentials. Journal of the American College of Nutrition. 1992; 11 (5):487-500 - 5.
Shahidi F, de Costa AC. Tocopherols and tocotrienols in common and emerging dietary sources: Occurrence, applications, and health benefits. International Journal of Molecular Sciences. 2016; 17 (10):1745 - 6.
Zainal Z, Khaza'ai H, Radhakrishnan AK, Chang SK. Therapeutic potential of palm oil vitamin E-derived tocotrienols in inflammation and chronic diseases: Evidence from preclinical and clinical studies. Food Research International. 2022; 156 :111175 - 7.
Zhang T et al. Vitamin E intake and multiple health outcomes: An umbrella review. Frontiers in Public Health. 2023; 11 :1035674 - 8.
Organização Pan-Americana da Saúde, Doenças Cardiovasculares [Internet]. 2023. Available from: https://www.paho.org/pt/topicos/doencas-cardiovasculares [Accessed: November, 2023]. - 9.
Corrêa-Camacho CR, Dias-Melicio LA, Soares AMVC. Aterosclerose, uma resposta inflamatória. Arq Ciênc Saúde. 2007; 14 (1):41-48 - 10.
Batlouni M. Hipótese oxidativa da aterosclerose e emprego dos antioxidantes na doença arterial coronária. Arquivos Brasileiros de Cardiologia. 1997; 68 (1):55-63 - 11.
Cheng P et al. Vitamin E intake and risk of stroke: A meta-analysis. The British Journal of Nutrition. 2018; 120 :1181-1188 - 12.
Li F, Xu B, Soltanieh S, Zanghelini F, Abu-Zaid A, Sun J. The effects of tocotrienols intake on obesity, blood pressure, inflammation, liver and glucose biomarkers: A meta-analysis of randomized controlled trials. Critical Reviews in Food Science and Nutrition. 2021; 62 (26):7154-7167 - 13.
Han J, Zhao C, Cai J, Liang Y. Comparative efficacy of vitamin supplements on prevention of major cardiovascular disease: Systematic review with network meta-analysis. Complementary Therapies in Clinical Practice. 2020; 39 :101142 - 14.
An P et al. Micronutrient supplementation to reduce cardiovascular risk. JACC. 2022; 80 (24):2269-2285 - 15.
Machado AD, Andrade GRG, Levy J, Ferreira SS, Marchioni DM. Association between vitamins and minerals with antioxidant effects and coronary artery calcification in adults and older adults: A systematic review. Current Pharmaceutical Design. 2019; 25 :2474-2479 - 16.
Shah S et al. A systematic review of effects of vitamin E on the cardiovascular system. Cureus. 2021; 13 (6):e15616 - 17.
Hamedi-Kalajahi F et al. A systematic review and meta-analysis on the impact of oral vitamin E supplementation on apolipoproteins A1 and B100. Clinical Nutrition. 2021; 46 :106-114 - 18.
O’Connor EA et al. Vitamin and mineral supplements for the primary prevention of cardiovascular disease and cancer. Update evidence report and systematic review for the US preventive services task force. JAMA. 2022; 327 (23):2334-2347 - 19.
Dludla PV et al. Dietary supplements potentially target plasma glutathione levels to improve cardiometabolic health in patients with diabetes mellitus: A systematic review of randomized clinical trials. Nutrients. 2023; 15 (4):944 - 20.
Khan MS et al. Dietary interventions and nutritional supplements for heart failure: A systematic appraisal and evidence map. European Journal of Heart Failure. 2021; 23 :1468-1476 - 21.
Torquato P et al. Analytical strategies to assess the functional metabolome of vitamin E. Journal of Pharmaceutical and Biomedical Analysis. 2016; 124 :399-412 - 22.
Phang SCW, Ahmad B, Kadir KA, Palanisamy UDM. Effects of tocotrienol-rich fraction supplementation in patients with type 2 diabetes: A systematic review and meta-analysis of randomized controlled trials. Advances in Nutrition. 2023; 14 :1159-1169 - 23.
Absalome MA et al. Biochemical properties, nutritional values, health benefits and sustainability of palm oil. Biochimie. 2020; 178 :81-95 - 24.
Marangoni F et al. Palm oil and human health. Meeting report of NFI: Nutrition Foundation of Italy symposium. International Journal of Food Sciences and Nutrition. 2017; 68 :643-655 - 25.
Sen CK, Rink C, Khanna S. Palm oil-derived natural vitamin E alphatocotrienol in brain health and disease. Journal of the American College of Nutrition. 2010; 29 :314s-323s - 26.
Shahidi F, Pinaffi-Langley ACC, Fuentes J, Speisky H, de Camargo AC. Vitamin E as an essential micronutrient for human health: Common, novel, and unexplored dietary sources. Free Radical Biology & Medicine. 2021; 176 :312-321 - 27.
Siger A, Górnas P. Free tocopherols and tocotrienols in 82 plant species' oil: Chemotaxonomic relation as demonstrated by PCA and HCA. Food Research International. 2023; 164 :112386 - 28.
Universidade Federal de São Paulo. Tabela Composição Alimentos – UNIFESP. São Paulo: Departamento de Informática em Saúde. Escola Paulista de Medicina. Universidade Federal de São Paulo. [Internet]. UNICAMP. 2011. Available from: http://tabnut.dis.epm.br/alimento - 29.
Torres LCR, Sartori AGO, Silva APS, Alencar SM. Bioaccessibility and uptake/epithelial transport of vitamin E: Discoveries and challenges of in vitro andex vivo assays. Food Research International. 2022;162 :112143 - 30.
Yap WN et al. Gamma-and delta-tocotrienols inhibit skin melanin synthesis by suppressing constitutive and UV-induced tyrosinase activation. Pigment Cell & Melanoma Research. 2001; 23 :688-692 - 31.
Fairus S, Nor RM, Cheng HM, Sundram K. Alpha-tocotrienol is the most abundant tocotrienol isomer circulated in plasma and lipoproteins after postprandial tocotrienol-rich vitamin E supplementation. Nutrition Journal. 2012; 11 :5 - 32.
Rizvi S, Raza ST, Ahmed F, Ahmed A, Abbas S, Mahdi F. The role of vitamin e in human health and some diseases. Sultan Qaboos University Medical Journal. 2014; 14 (2):e157-e165 - 33.
Waniek S et al. Vitamin E (α-and γ-tocopherol) levels in the community: Distribution, clinical and biochemical correlates, and association with dietary patterns. Nutrients. 2018; 10 (1):3 - 34.
Bardowell SA, Ding X, Parker RS. Disruption of P450-mediated vitamin E hydroxylase activities alters vitamin E status in tocopherol supplemented mice and reveals extra-hepatic vitamin E metabolism. Journal of Lipid Research. 2012; 53 (12):2667-2676 - 35.
Soysal P, Arik F, Smith L, Jackson SE, Isik AT. Inflammation, frailty and cardiovascular disease. Advances in Experimental Medicine and Biology. 2020; 1216 :55-64 - 36.
Phaniendra A, Jestadi DB, Periyasam L. Free radicals: Properties, sources, their implication in various diseases. Indian Journal of Clinical Biochemistry. 2015; 30 (1):11-26 - 37.
Jideani AJO, Silungwe H, Takalani T, Omolola AO, Udeh HO, Anyasi TA. Antioxidant-rich natural fruit and vegetable products and human health. International Journal of Food Properties. 2021; 24 :41-67 - 38.
Khorami SAH, Mutalib MSA, Khazai’ai H. Comparative effect of vitamin E compounds on HSP70 expression in response to acute redox imbalance in Chang liver cells Research Square. April 21st, 2020. DOI: q0.21203/rs.3.rs-22336/vl - 39.
Trela-Makowej A, Kruk J, Zadlo A, Szymanska R. Antioxidant activity of vitamin E homologues in model systems, [Internet]. 2021. DOI: 10.21203/rs.3.rs-199353/v1 - 40.
Jiang Z, Yin X, Jiang Q. Natural forms of vitamin E and 130-carboxychromanol, a long-chain vitamin E metabolite, inhibit leukotriene generation from stimulated neutrophils by blocking calcium influx and suppressing 5-lipoxygenase activity, respectively. Journal of Immunology. 2011; 186 :1173-1179 - 41.
Jiang Q. Natural forms of vitamin E: Metabolism, antioxidant, and anti-inflammatory activities and their role in disease prevention and therapy. Review article. Free Radical Biology & Medicine. 2014; 72 :76-90 - 42.
Boutaud O, Aronoff DM, Richardson JH, Marnett LJ, Oates JA. Determinants of the cellular specificity of acetaminophen as an inhibitor of prostaglandin H(2)synthases. Proceedings of the National Academy of Sciences of the United States of America. 2002; 99 :7130-7135 - 43.
Jiang Q, Elson-Schwab I, Courtemanche C, Ames BN. Gamma-tocopherol and its major metabolite, in contrast to alpha-tocopherol, inhibit cyclooxygenase activity in macrophages and epithelial cells. Proceedings of the National Academy of Sciences of the United States of America. 2000; 97 (21):11494-11499 - 44.
Jiang Q, Yin X, Lill MA, Danielson ML, Freiser H, Huang J. Long-chain carboxychromanols, metabolites of vitamin E, are potent inhibitors of cyclooxygenases. Proceedings of the National Academy of Sciences of the United States of America. 2008; 105 :20464-20469 - 45.
Papaioannou D, Cooper KL, Carroll C, Hind D, Squires H, Tappenden P, et al. Antioxidants in the chemoprevention of colorectal cancer and colorectal adenomas in the general population: A systematic review and meta-analysis. Colorectal Disease. 2011; 13 (10):1085-1099 - 46.
Moya-Camarena SY, Jiang Q. The role of vitamin E forms in cancer prevention and therapy—Studies in human intervention trials and animal models. In: Sarkar FH, editor. Nutraceuticals and Cancer. New York: Springer; 2012. pp. 323-354. (Chap.15) - 47.
Dolara P, Bigagli E. Collins A, antioxidant vitamins and mineral supplementation, life span expansion and cancer incidence: Acritical commentary. European Journal of Nutrition. 2013; 51 :769-781 - 48.
Myung SK et al. Efficacy of vitamin and antioxidant supplements in prevention of cardiovascular disease: Systematic review and meta-analysis of randomised controlled trials. BMJ. 2013; 346 (f10). DOI: 10.1136/bmj.f10 - 49.
Dovizio M, Alberti S, Guillem-Llobat P, Patrignani P. Role of platelets in inflammation and cancer: Novel therapeutic strategies. Basic & Clinical Pharmacology & Toxicology. 2014; 114 (1):118-127 - 50.
Debbabi M et al. Protective effects of alpha-tocopherol, gamma-tocopherol and oleic acid, three compounds of olive oils, and no effect of trolox, on 7-ketocholesterol-induced mitochondrial and peroxisomal dysfunction in microglial BV-2 cells. International Journal of Molecular Sciences. 2016; 17 (12):1973 - 51.
Jiang Q. Metabolism of natural forms of vitamin E and biological actions of vitamin E metabolites. Free Radical Biology & Medicine. 2022; 179 :375-387 - 52.
Menn GL, Jablo'nska A, Chen Z. The effects of post-translational modifications on Th17/Treg cell differentiation. Biochimica et Biophysica Acta - Molecular Cell Research. 2022; 6 :119223 - 53.
Fu JY, Meganathan P, Gunasegaran N, Tan DMY. Effect of nano-delivery systems on the bioavailability and tissue biodistribution of vitamin E tocotrienols. Food Research International. 2023; 171 :113048 - 54.
Zhao H et al. γ-Tocotrienol inhibits T helper 17 cell differentiation via the IL-6/JAK/STAT3 signaling pathway. Molecular Immunology. 2022; 151 :126-133 - 55.
Kim Y, Gromovsky AD, Brown JM, Chung S. Gamma-tocotrienol attenuates the aberrant lipid mediator production in NLRP inflammasome-stimulated macrophages. The Journal of Nutritional Biochemistry. 2018; 58 :169-177 - 56.
Grimm MOW, Mett J, Hartmann T. The impact of vitamin E and other fat-soluble vitamins on Alzheimer s disease. International Journal of Molecular Sciences. 2016; 17 (11):1785 - 57.
Ismail M et al. Safety and neuroprotective efficacy of palm oil and tocotrienol-rich fraction from palm oil: A systematic review. Nutrients. 2020; 12 (2):521 - 58.
Malavolta M et al. Pleiotropic effects of tocotrienols and quercetin on cellular senescence: Introducing the perspective of senolytic effects of phytochemicals. Current Drug Targets. 2016; 17 :447-459 - 59.
Rahman TA, Hassim NF, Zulkafli N, Muid S, Kornain NK, Nawawi H. Atheroprotective effects of pure tocotrienol supplementation in the treatment of rabbits with experimentally induced early and established atherosclerosis. Food & Nutrition Research. 2016; 60 :31525 - 60.
Das S et al. Cardioprotection with palm tocotrienol: Antioxidant activity of tocotrienol is linked with its ability to stabilize proteasomes. American Journal of Physiology. Heart and Circulatory Physiology. 2012; 302 (11):H2447 - 61.
Kosmas CE et al. High-density lipoprotein (HDL) functionality and its relevance to atherosclerotic cardiovascular disease. Drugs Context. 2018; 7 :212525 - 62.
American Diabetes Association. Standards of medical care in diabetes. Diabetes Care. 2009; 32 (suppl 1):S13-S61 - 63.
Skyler JS et al. Differentiation of diabetes by pathophysiology. Natural History, and Prognosis, Diabetes. 2017; 66 (2):241-255 - 64.
Birringer M, Lorkowski S. Vitamin E: Regulatory role of metabolites. IUBMB Life. 2019; 71 (4):479-486 - 65.
Wells SR, Jennings MH, Rome C, Hadjivassiliou V, Papas KA, Alexander JS. α-, γ- and δ-tocopherols reduce inflammatory angiogenesis in human microvascular endothelial cells. The Journal of Nutritional Biochemistry. 2010; 21 (7):589-597 - 66.
Villas Boas GR, Paes MM, Cunha MS, Ponsoni LF, da Silveira APS, Oesterreich SA. Evaluation of the effect of alpha-tocopherol on anxiety and the neuroinflammatory process during alcohol withdrawal in a model of forced and chronic self-administration of liquid diet containing ethanol: Behavioral and neurochemical evidence. Alcohol. 2022; 104 :31-44 - 67.
Yang C, Jiang Q. Vitamin E δ-tocotrienol inhibits TNF-α-stimulated NF-κB activation by up-regulation of anti-inflammatory A20 via modulation of sphingolipid including elevation of intracellular dihydroceramides. The Journal of Nutritional Biochemistry. 2019; 64 :101-109 - 68.
Dhodapkar MM, Ramachandran XSR, Wallach JD. Characterization and corroboration of safety signals identified from the US Food and Drug Administration adverse event reporting system, 2008-19: Cross sectional study. BMJ. 2022; 379 :e071752 - 69.
Violi F, Nocella C, Lofredo L, Carnevale R, Pignatelli P. Interventional study with vitamin E in cardiovascular disease and meta-analysis. Free Radical Biology & Medicine. 2022; 178 :26-41 - 70.
Hu FB, Willett WC. Optimal diets for prevention of coronary heart disease. JAMA. 2002; 288 (20):2569-2578 - 71.
Bowry VW, Ingold KU, Stocker R. Vitamin E in human low-density lipoprotein. When and how this antioxidant becomes a pro-oxidant. The Biochemical Journal. 1992; 288 (Pt 2):341-344 - 72.
Naidoo N et al. Plasma vitamin E and coenzyme Q10 are not associated with a lower risk of acute myocardial infarction in Singapore Chinese adults. The Journal of Nutrition. 2012; 142 :1046-1052 - 73.
Nagao M, Moriyama Y, Yamagishi K, Iso H, Tamakoshi A. Relation of serum α- and γ-tocopherol levels to cardiovascular disease-related mortality among Japanese men and women. Journal of Epidemiology. 2012; 22 :402-410 - 74.
Diepeveen S et al. Effects of atorvastatin and vitamin E on lipoproteins and oxidative stress in dialysis patients: A randomised-controlled trial. Journal of Internal Medicine. 2005; 257 (5):438-445 - 75.
Keihan GS, Gharib MH, Momeni A, Hemati Z, Sedighin R. A comparison between the effect of cuminum and vitamin E on the level of leptin, paraoxonase 1, HbA1c and oxidized LDL in diabetic patients. International Journal of Molecular and Cellular Medicine. 2016; 5 (4):229-235 - 76.
Arad Y, Spadaro LA, Roth M, Newstein D, Guerci AD. Treatment of asymptomatic adults with elevated coronary calcium scores with atorvastatin, vitamin C, and vitamin E: The St. Francis heart study randomized clinical trial. Journal of the American College of Cardiology. 2005; 46 (1):166-172 - 77.
de Oliveira Otto MC et al. Dietary micronutrient intakes are associated with markers of inflammation but not with markers of subclinical atherosclerosis. The Journal of Nutrition. 2011; 141 (8):1508-1515 - 78.
Hatzigeorgiou C, Taylor AJ, Feuerstein IM, Bautista L, O’Malley PG. Antioxidant vitamin intake and subclinical coronary atherosclerosis. Preventive Cardiology. 2006; 9 (2):75-81 - 79.
Falcone EL et al. Micronutrient concentrations and subclinical atherosclerosis in adults with HIV. The American Journal of Clinical Nutrition. 2010; 91 (5):1213-1219 - 80.
de Souza DP, Waters C. Perfil epidemiológico dos pacientes com acidente vascular cerebral: pesquisa bibliográfica. Brazilian Journal of Health Review. 2023; 6 (1):1466-1478 - 81.
Bell SJ, Grochoski GT. How safe is vitamin E supplementation? Critical Reviews in Food Science and Nutrition. 2008; 48 :760-774 - 82.
Miller ER, Pastor-Barriuso R, Dalal D, Riemersma RA, Appel LJ, Guallar E. Metaanalysis: High-dosage vitamin E supplementation may increase all-cause mortality. Annals of Internal Medicine. 2005; 142 (1):37-46