Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
To purchase hard copies of this book, please contact the representative in India:
CBS Publishers & Distributors Pvt. Ltd.
www.cbspd.com
|
customercare@cbspd.com
Childhood sleep apnea is characterized as airway obstruction because of upper airway impairment due to reduced oxygen levels or awakening from sleep in children. In children, only 1–5% of children suffer from sleep apnea, which equals to about 20 million−100 million children, globally. However, childhood sleep apnea tends to be underdiagnosed with about 90% of children not being properly diagnosed with sleep apnea. Sleep apnea is a major concern due to the harmful clinical manifestations associated with the condition, such as abnormal breathing during sleep, frequent awakenings or restlessness, frequent nightmares, nocturnal enuresis, difficulty getting up in the morning, excessive daytime sleepiness (EDS), ADHD-like symptoms, daytime mouth breathing, and abnormal sleep patterns. There are also certain risk factors that can increase the risk of childhood sleep apnea. These risk factors are tonsillar hypertrophy, adenoid hypertrophy, obesity, craniofacial anomalies, and neuromuscular disorders. Childhood risk factors are important to consider because they can increase risk and severity. To aid an efforts to relieve, prevent, and diagnose childhood sleep apnea, there needs to be more efforts to promote, to educate, and to implement diagnostic testing for sleep apnea as a standard of care in pediatric patients.
Department of Epidemiology and Biostatistics, Jackson State University, Jackson, MS, USA
*Address all correspondence to: eakjones@yahoo.com
1. Introduction
Childhood sleep apnea is characterized as airway obstruction because of upper airway impairment due to reduced oxygen levels or awakening from sleep in children. Childhood sleep apnea is less commonly diagnosed and can severely affect functioning, growth, behavior, and development. Knowledge of childhood sleep apnea is very important because it allows adults to understand the source of certain behaviors, promote awareness, and to ensure the proper diagnosis of children with sleep apnea. This chapter introduces several concepts including, prevalence of sleep apnea, risk factors, clinical manifestations, diagnosis, screening, and recommendations.
“Globally, around 1 billion people suffer from sleep apnea” [1]. “In children, only 1–5% of children suffer from sleep apnea, which equals to about 20 million–100 million children, globally” [2]. While the prevalence of sleep apnea is lower in children than adults, childhood sleep apnea is usually not diagnosed as frequently as in adults. “About 90% of children are underdiagnosed for sleep apnea” [3]. Childhood sleep apnea is usually underdiagnosed because of the difficulty detecting the condition in children.
2.1 Prevalence of sleep apnea in children by sex
“The prevalence of childhood sleep apnea is equal in boys and girls, which equivocates to a prevalence of 10 million–50 million for both boys and girls” [4]. “Both boys and girls, who have asthma or are obese have an increased risk of childhood sleep apnea” [5]. While childhood asthma and obesity have been shown to increase the risk of childhood sleep apnea, the role that asthma and obesity play in sleep apnea severity is unknown in both boys and girls. “Other risk factors that are associated with childhood sleep apnea in both boys and girls are down syndrome, facial birth defects, birth defects in the skull, cerebral palsy, sickle cell disease, neuromuscular disease, low birth weight, and family history of sleep apnea” [6].
2.2 Prevalence of sleep apnea in children by age and race
Table 1 indicates that the prevalence of sleep apnea for children between the ages 0–4 years is 0.66%, the prevalence of sleep apnea for children between the ages of 5–9 years is 1.37%, the prevalence of sleep apnea for children between the ages of 10–14 years is 1.56%, and the prevalence of sleep apnea for children between the ages of 15–19 years is 1.14% [7]. Table 1 shows that children between the ages of 10–14 years have a higher prevalence of sleep apnea. Typically, children between the ages of 10–14 are experiencing puberty. At times, puberty has been shown to increase the risk of sleep apnea because growth spurts can cause sleep disorder breathing.
Table 1 also indicates that the prevalence of sleep apnea in Black children is 47.1%, the prevalence of sleep apnea in Hispanic children in 12.5%, and the prevalence of sleep apnea in White children is 40.4%. “Table 1 shows Black children have a higher prevalence of sleep apnea” [8]. “Studies have shown that Black children have a higher odds of developing sleep apnea and often have a 20% increase in the severity of sleep apnea” [8].
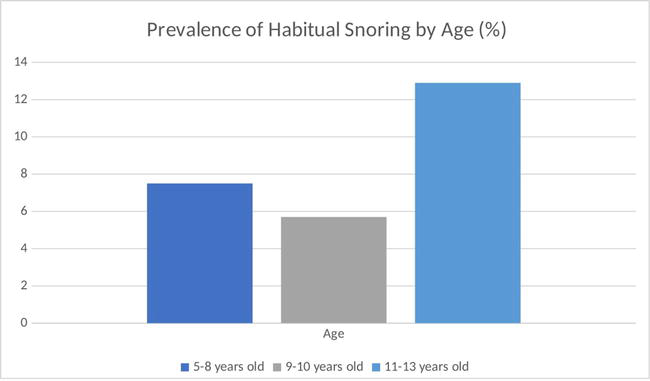
Snoring is a severe sound that obstructs air through the nose and pharynx. “Generally, snoring is quite common in children” [9]. Since snoring is seen as common, it is not seen as a concern. “However, habitual snoring can be a sign of sleep apnea. “Habitual snoring is defined as snoring 3 or more nights per week” [10, 11].
“Globally, 60,000,000 million–240,000,000 million children snore, accounting for a prevalence of 3–12%” [12]. In children, “African Americans have a higher prevalence of snoring” [13]. Figure 1 also indicates the prevalence of habitual snoring by age. Children between the ages of 11–13 have a higher prevalence of habitual snoring.
“These risk factors are tonsillar hypertrophy, adenoid hypertrophy, obesity, craniofacial anomalies, and neuromuscular disorders” [14, 15]. Childhood risk factors are important to consider because they can increase risk and severity.
5.1 Tonsillar hypertrophy
Tonsillar hypertrophy is a condition characterized by swollen or enlarged tonsils. Tonsillar hypertrophy is commonly diagnosed in children. Tonsillar hypertrophy increases the risk of childhood sleep apnea because the condition causes the narrowing of the upper airways, which can lead to airway obstruction.
5.2 Adenoid hypertrophy
Adenoid hypertrophy is characterized by enlarged or swollen adenoids. When adenoid hypertrophy and reduced muscle tones are both present simultaneously in children, the conditions significantly increase the risk of childhood sleep apnea. Both conditions simultaneously cause severe airway obstruction.
5.3 Obesity
Obesity is characterized as a body mass index of 30 or higher. Body mass index is the measure of body fat by height and weight. Obesity is a very common risk factor in children diagnosed with sleep apnea. Fat build-up in the upper respiratory track reduce airway flow, which leads to decrease muscle activity. The reduction of muscle activity results in hypoxia and apneic episodes, which causes sleep apnea.
5.4 Craniofacial anomalies
Craniofacial anomalies are characterized by facial and head deformities in children. “Generally, certain craniofacial anomalies put children more at risk of sleep apnea including, maxillary hypoplasia, mandibular hypoplasia, poor motor tone, crowded oropharynx, and macroglossia” [16]. These conditions tend to cause air narrowing and obstruction.
5.5 Neuromuscular disorders
Neuromuscular disorders are characterized as peripheral nervous system diseases. “Specifically, polymyositis, dermatomyositis, and inclusion body myositis are neuromuscular conditions that cause sleep apnea in children” [17]. These conditions result in sleep apnea due to a loss of muscle tone, respiratory muscles weakness, and movement impairment.
6.1 Prevalence of tonsillar hypertrophy by age, sex, and race
1–5% of children with sleep apnea have tonsillar hypertrophy. Usually, children between the ages of 2–8 years old have a higher prevalence of tonsillar hypertrophy. The prevalence of tonsillar hypertrophy is also associated with sex in children. Boys diagnosed with tonsillar hypertrophy have a higher prevalence of sleep apnea compared to girls. The prevalence of tonsillar hypertrophy in boys is 55.4% compared to 44.6% in girls. However, there is no known association between tonsillar hypertrophy in childhood sleep apnea cases and race.
6.2 Prevalence of adenoid hypertrophy by age, sex, and race
1–5% of children with sleep apnea have adenoid hypertrophy. Usually, children ages 2–8 years old have a higher prevalence of adenoid hypertrophy. However, sex and race do not play a role in the relationship between adenoid hypertrophy and childhood sleep apnea.
6.3 Prevalence of obesity by age, sex, and race
“13–59% of children with sleep apnea are obese” [18]. Typically, boys, who are obese have a higher prevalence of sleep apnea compared to girls, who are obese. In terms of age, obese adolescents have a higher prevalence of sleep apnea than obese children of other ages. However, the relationship between race and obesity in childhood sleep apnea cases vary.
6.4 Prevalence of craniofacial anomalies by age, sex, and race
“Around 16% of children with craniofacial anomalies have sleep apnea” [16]. “However, children with craniofacial anomalies are 30 times more likely to be diagnosed with sleep apnea compared to children without craniofacial anomalies” [16]. Currently, there is no known association between age, sex, and race in children with craniofacial anomalies and sleep apnea diagnosis.
6.5 Prevalence of neuromuscular disorders by age, sex, and race
“40% of children with neuromuscular disorders have childhood sleep apnea” [18]. “Generally, children between the ages of 10–12 years old with neuromuscular disorders have a higher prevalence of sleep apnea” [18]. However, the relationship between sex and race in children diagnosed with neuromuscular disorders and sleep apnea vary.
A genetic risk factor is the probability of having a genetic mutation or disorder associated with a disease. Genetic risk factors in children such as, down syndrome, prader-willi syndrome (PWS), smith-magensis syndrome, and angelman syndrome (AS) often significantly increase the risk of obstructive sleep apnea compared to children without these conditions. Sleep apnea in children with down syndrome, PWS, smith-magensis syndrome, or AS can result in very harmful health outcomes both physically, mentally, and developmentally.
7.1 Down syndrome
Children with down syndrome have an increased risk of sleep apnea. Down syndrome is a genetic disease associated with an extra chromosome 21. Individuals with down syndrome have certain physical features associated with their genetic condition, such as enlarged adenoids, tongue, tonsils, flat face, short neck, and poor muscle tone. These physical features are the reason for their increased risk of sleep apnea compared to other children.
7.2 Prader-Willi syndrome
Commonly, children with prader-willi syndrome (PWS) have an increased risk of sleep apnea. PWS is a genetic condition that results in numerous physical, mental, and behavioral challenges. The most common symptom associated with PWS is experiencing constant hunger. Due to constant hunger being the most common symptom of the condition, children with PWS are usually obese. Being obese increases the risk of childhood sleep apnea.
7.3 Smith-Magenis syndrome
Children with smith-magenis syndrome have higher rates of sleep apnea than children without the condition. Smith-Magenis syndrome is a developmental disorder associated with emotional challenges, behavioral challenges, and difficulty with learning processes. Individuals with Smith-Magenis syndrome also have certain phenotypic facial features that increase their risk of childhood sleep apnea.
7.4 Angelman syndrome
Children diagnosed with AS also have an increased risk of sleep apnea. AS is a genetic disease associated with developmental challenges, problems with balance and speech, and seizures. Individuals with AS often have a happy disposition and are easily excitable. Generally, children with AS have difficulty falling asleep, remaining asleep, and have various other sleep related conditions.
8.1 Prevalence of sleep apnea in children with down syndrome by age, sex, and race
“The prevalence of sleep apnea in children with down syndrome is 53–76% compared to children without down syndrome, who have disease prevalence of 1–5%” [19]. Prevalence of sleep apnea is also higher in younger children with down syndrome compared to older children with down syndrome. However, the prevalence of sleep apnea does not differ by sex or by race and ethnicity in children with down syndrome.
8.2 Prevalence of sleep apnea in children with prader-willi syndrome by age, sex, and race
“The prevalence of sleep apnea in children with PWS is 57%” [20]. Prevalence of sleep apnea is also higher in older children (>2 years) with PWS compared to younger children with the condition [20]. However, the prevalence of sleep apnea does not differ by sex or by race and ethnicity in children with PWS.
8.3 Prevalence of sleep apnea in children with angelman syndrome by age, sex, and race
“The prevalence of sleep apnea in children with AS is 20–80%” [21]. Prevalence of sleep apnea is higher for children between 2 and 6 years and diminishes as a child progresses through late childhood [21]. However, the prevalence of sleep apnea does not differ by sex or by race and ethnicity in children with AS.
Clinical manifestations vary for all children. Clinical manifestations for childhood sleep apnea include abnormal breathing during sleep, frequent awakenings or restlessness, frequent nightmares, nocturnal enuresis, difficulty getting up in the morning, excessive daytime sleepiness (EDS), daytime mouth breathing, abnormal sleep patterns, non-rapid eye movement (NREM) parasomnias, ADHD-like syndrome, and cognitive and neuropsychological conditions. Clinical manifestations present in children tend to make day to day activities difficult for parents and children.
9.1 Abnormal breathing during sleep
“Abnormal breathing during sleep is characterized by the ceasing of breathing during sleep” [22]. Breathing cessation is usually the result of airway blockage from enlarged tonsils or adenoids in the upper airway. Abnormal breathing can be observed in children by noticing brief pauses during sleep.
9.2 Frequent awakenings or restlessness
Frequent awakenings or restlessness is characterized by disruptions from sleep or awakening or inability to sleep. Frequent awakenings are a result of lacking oxygen, which result in the initiation of the survival reflex. The survival reflex is used to allow the child to return to normal breathing by waking-up.
9.3 Frequent nightmares
Frequent nightmares are characterized by unpleasant dreams during sleep. Children, who suffer from sleep apnea experience abnormal or fragmented sleep patterns that can cause high alert in the brain. By the brain being in high alert, it can result in mental distress that can be expressed as nightmares in children.
9.4 Nocturnal enuresis
Nocturnal enuresis is bedwetting that occurs at night. Enuresis is a secondary condition that occurs due to exhaustion from the inability to sleep due to childhood sleep apnea. “Children, who experience exhaustion or extreme fatigue may not be able to control their bladder as well as children, who are not suffering from sleep apnea” [23].
9.5 Difficulty getting up in the morning
Children with sleep apnea may have trouble getting up in the morning due to irritability from the lack of a normal sleep pattern caused by childhood sleep apnea. The irritability that a child may experience during awakening can last throughout the day, which can result in issues in the classroom.
9.6 Excessive daytime sleepiness
EDS is characterized as the inability to remain awake or alert during the daytime. EDS in children can result in failing grades, emotional disturbances, and inattentiveness. Obese children with sleep apnea are more likely to suffer from EDS than non-obese children with EDS at any given severity level of sleep apnea.
9.7 ADHD-like symptoms
ADHD-like symptoms are characterized as disruptive behavior in children and is a mimicry condition to ADHD. ADHA-like symptoms are associated with childhood sleep apnea. ADHD-like symptoms make it difficult for children to function and concentrate properly during the day.
9.8 Daytime mouth breathing
Children with sleep apnea tend to suffer from adenoid hypertrophy and tonsillar hypertrophy. These conditions usually cause daytime mouth breathing. Daytime mouth breathing is characterized as a child breathing through their mouth instead of their nose during the daytime hours. Daytime mouth breathing can cause harm to a child’s mental and oral health. Mentally, daytime breathing can result in issues with problem solving and concentration. In terms of oral health, long-term daytime mouth breathing can cause gum disease, caries, crowded teeth, and cracked lips.
9.9 Sleep patterns
Sleep patterns are characterized as the typical sleep cycle that individuals undergo each night. “A typical sleep pattern has 4 to 6 cycles each night. These cycles last 80–100 minutes and involve two phases of sleep” [24]. “Children with moderate sleep apnea have an abnormal sleep pattern that results in children waking up 120–239 minutes per 8 hours of sleep” [25]. “Children with severe sleep apnea may wake-up 30 or more times per hour” [25].
9.10 Non-rapid eye movement parasomnias
NREM parasomnias is characterized as “sleep walking and confusional arousals during the first half of the night” [26]. Children with sleep apnea may experience NREM parasomnias. NREM parasomnias are caused by cortical arousals and/or sleep inertia caused by abnormalities in arousal mechanisms due to sleep apnea.
9.11 Deficits of IQ and executive function
Children diagnosed with sleep apnea also suffer from cognitive and neuropsychological effects. Children with sleep apnea may have lower IQs and poor executive functioning. Developing children with untreated sleep apnea can have their cognitive function altered permanently.
Clinical symptoms of sleep apnea do not manifest in the same manner in children as adults. For children, clinical manifestations tend to affect behavior, which can result in hyperactivity and inability to concentrate. While the clinical manifestation of symptoms differs for adults and children, symptoms of sleep apnea fluctuate for all children. Due to fluctuation of clinical symptoms in children, diagnosis criteria, clinical criteria, and the assessment of severity play a major role in understanding the extent of sleep apnea in children.
10.1 Diagnosis criteria
Diagnosis criteria for childhood sleep apnea are factors used in medical practice to direct the care of young patients through the assessment of symptoms, signs, and tests. Generally, diagnosis criteria are very important aspects of medical practice and patient care because it ensures that patients receive the best possible care. In children, the diagnosis criteria for sleep apnea are vital in preventing, understanding, and identifying declines in oxygen levels, or increases in carbon dioxide levels.
According to the American Academy of Family Physicians (AAFP), “the golden standard for the diagnosis criteria of sleep apnea in children is measured using the apnea-hypopnea index (AHI)” [27]. The AHI is the average rate of breathing disturbances or apneas or shallow or unusually slow breathing patterns or hypopneas. The AAFP has set the golden standard for the diagnosis criteria of childhood sleep apnea as an “AHI of greater than 1 or an average of 0.1–0.5 events per hour or a minimum oxygen saturation level of less than 92%” [27].
10.1.1 Clinical criteria
Clinical criteria are guidelines that are used to assess a patient’s condition to establish the patient’s medical needs. In children with sleep apnea, clinical criteria are used to assess a child’s condition to lead to a diagnosis. The clinical criteria of childhood sleep apnea are “snoring, labored, paradoxical, or obstructed breathing during sleep, sleepiness, hyperactivity, behavioral problems, or learning problems” [28].
10.1.2 Polysomnography
Polysomnography (PSG) is a test that is used to diagnose sleep apnea in adults and children. PSG diagnoses sleep disorders by measuring AHI or respiratory disturbance index (RDI). Typically, the most recommended environment for the use of PSG in children is to use an overnight PSG in a sleep laboratory. Figure 2 depicts PSG in a child with severe obstructive sleep apnea.
Figure 2.
PSG in a child with severe obstructive sleep apnea [21].
10.2 Assessment of severity
The assessment of severity is used to describe the intensity of sleep apnea cases in children. There are three grades of severity- mild obstructive sleep apnea, moderate obstructive sleep apnea, and severe obstructive sleep apnea. “Mild sleep apnea is defined as an AHI of greater than 1 to less than 5” [29]. “Moderate sleep apnea is defined as an AHI of greater than or equal to 5 or less than 10” [29]. “Severe sleep apnea is defined as an AHI of greater than or equal to 10” [29].
10.3 Preliminary classification using respiratory disturbance index/apnea-hypopnea index
Both RDI and AHI can be used as a diagnosis and assessment tool for obstructive sleep apnea in children. While both RDI and AHI are similar, RDI also includes respiratory effort-related arousal (RERAs) as a standard for diagnosing and assessing severity of sleep apnea. RERAs is a disorder caused by airflow reduction in the upper airways and leads to increases in respiratory effort that settles by the appearance of arousal.
11. Screening
Screening is the application of tools used to detect potential disease occurrence in patients, who are without symptoms. Medically, symptoms are considered the subjective experience of patients, who are dealing with a health concern. The screening process for childhood sleep apnea involves the use of the pediatric sleep questionnaire (PSQ) to identify potential risk. Followed by using Nocturnal Polysomnogram (PSG) or the Nocturnal Pulse Oximetry to physically confirm cases of childhood sleep apnea. Generally, Nocturnal Polysomnogram is conducted in a sleep laboratory, while Nocturnal Pulse Oximetry is conducted at home.
11.1 Pediatric sleep questionnaire
“The Pediatric Sleep Questionnaire (PSQ) is a 22-item survey that accesses for apneas, snoring, sleepiness, and other childhood sleep apnea symptoms” [30]. PSQ is scored using 0 and 1 s with 0 s meaning that the symptom is absent and 1 s meaning that the symptom is present. “A final score of greater than or equal to 0.33 is used to indicate a risk of childhood sleep apnea” [30].
11.2 Nocturnal polysomnogram
Nocturnal PSGs conducted in sleep laboratories are considered the gold standard for detecting childhood sleep apnea. A nocturnal PSG can identify both obstructive events and assess severity. However, the process of scheduling nocturnal PSGs for pediatric patients is rather complex. Nocturnal PSGs for children are generally ordered based on several factors, including the decision of the healthcare provider, age, comorbidities, the preference of the parent or guardian, tolerance of sensors, and the availability and accessibility of PSG testing.
The technical process of nocturnal PSG testing involves the use of sensors to track brain waves, oxygen levels, breathing, heart rate, and physical movement, such as eye and leg movement. Typically, nocturnal PSGs are performed in sleep laboratories within hospitals or sleep centers. The set-up time for PSGs can be timely and the detection of nocturnal seizures can also extend the time further.
11.3 Nocturnal pulse oximetry
A nocturnal pulse oximetry is a device that is used to detect oxygen levels in the blood as a means for indicating the presence of childhood sleep apnea. Typically, nocturnal pulse oximetry is used at home during the night and is easy to use. The device has an apparatus that connects to one finger, which makes it easy to set-up and easy to manage for parents of young patients.
12. Summary and recommendations
Childhood sleep apnea is a very serious condition in children. While childhood sleep apnea may not be as common as adult sleep apnea, the effects of the disease is still very harmful and is often underdiagnosed in children. The effects of childhood sleep apnea tend to affect the day-to-day activities of children. Certain populations of children are also more at risk of sleep apnea due to genetic factors, and certain conditions, such as obesity, neuromuscular disorders, and craniofacial anomalies. To aid an efforts to relieve, prevent, and diagnose childhood sleep apnea, there needs to be more efforts to promote the commonality of the disease in children, to educate parents on identifying the symptoms, to explore new treatment options [31], andto promote the implementation of diagnostic testing for sleep apnea as a standard of care in pediatric patients.
References
1.Lyons MM, Bhatt NY, Pack AI, Magalang UJ. Global burden of sleep-disordered breathing and its implications. Respirology. 2020;25(7):690-702. DOI: 10.1111/resp.13838
2.Cleveland Clinic Medical. Is it sleep apnea? [Internet]. Available from: https://my.clevelandclinic.org/health/diseases/14312-obstructive-sleep-apnea-in-children
3.Science X. Up to 15 percent of children have sleep apnea, yet 90 percent go undiagnosed [Internet]. Medical Xpress; 2019. Available from: https://medicalxpress.com/news/2019-02-percent-children-apnea-undiagnosed.html#:~:text=Up%20to%2015%20percent%20of%20children%20have%20some%20form%20of,to%20psychological%20or%20emotional%20issues
4.Togeiro S, Santos C, Tufik S, Smith A, Moreira G. 0814 obstructive sleep apnea in asthmatic children: highly prevalent though no identifiable risk factors. Sleep. 2023;46(Supplment_1):00049-9. DOI: 10.1093/sleep/zsad077.0814
5.American Lung Association. The link between asthma and weight [Internet]. Available from: https://www.lung.org/blog/the-link-between-asthma-weight
6.Pediatric obstructive sleep apnea [Internet]. Mayo Foundation for Medical Education and Research; 2023. Available from: https://www.mayoclinic.org/diseases-conditions/pediatric-sleep-apnea/symptoms-causes/syc-20376196
7.Lumeng JC, Chervin RD. Epidemiology of pediatric obstructive sleep apnea. Sleep and Breathing in Children. 2008;5(2):429-450.DOI: 10.3109/9781420060836-23
8.Dudley KA, Patel SR. Disparities and genetic risk factors in obstructive sleep apnea. Sleep Medicine. 2016;18:96-102. DOI: 10.1016/j.sleep.2015.01.015
9.Tan Y, How C, Chan Y, Teoh O. Approach to the snoring child. Singapore Medical Journal. 2020;61(4):170-175. DOI: 10.11622/smedj.2020054
10.Isaiah A, Ernst T, Cloak CC, Clark DB, Chang L. Association between habitual snoring and cognitive performance among a large sample of preadolescent children. JAMA Otolaryngology–Head & Neck Surgery. 2021;147(5):426. DOI: 10.1001/jamaoto.2020.5712
11.Pediatric sleep-disordered breathing [Internet]. 2022. Available from: https://www.enthealth.org/conditions/pediatric-sleep-disordered-breathing/
12.Children with sleep apnea [Internet]. 2022. Available from: https://www.pinnacledentalgroupmi.com/obstructive-sleep-apnea-in-children-dont-ignore-a-childs-snoring/
13.Song S. Snoring at night may affect kids’ daytime behavior [Internet]. Time; 2012. Available from: https://healthland.time.com/2012/08/13/how-a-childs-nighttime-snoring-may-affect-daytime-behavior/
14.Baidas L, Al-Jobair A, Al-Kawari H, AlShehri A, Al-Madani S, Al-Balbeesi H. Prevalence of sleep-disordered breathing and associations with orofacial symptoms among Saudi primary school children. BMC Oral Health. 2019;19(1):43. DOI: 10.1186/s12903-019-0735-381
15.Xu Z, Wu Y, Tai J, Feng G, Ge W, Zheng L, et al. Risk factors of obstructive sleep apnea syndrome in children. Journal of Otolaryngology - Head & Neck Surgery. 2020;49(1):11. DOI: 10.1186/ s40463-020-0404
16.Lam DJ, Jensen CC, Mueller BA, Starr JR, Cunningham ML, Weaver EM. Pediatric sleep apnea and craniofacial anomalies: a population-based case-control study. The Laryngoscope. 2010;120(10):2098-2105. DOI: 10.1002/lary.21093
17.Lacomis D. Neuromuscular disorders in critically ill patients: review and Update. Journal of Clinical Neuromuscular Disease. 2011;12(4):197-218. DOI: 10.1097/cnd.0b013e3181b5e14d
18.Kinimi L. Clinical Profile of Children with Suspected Sleep Apnea [Internet]. 2022. Available from: https://journals.lww.com/jpp/_layouts/15/oaks.journals/ PageNotFound.aspx
19.Sleep & down syndrome [Internet]. 2023. Available from: https://ndss.org/resources/sleep-down syndrome#:~:text=Children%20syndrome%20are,Facial%20structure%20differences
20.Hedstrom S. Sleep apnea in people with PWS [Internet]. 2017. Available from: https://www.fpwr.org/blog/sleep-apnea-in-people-with pws#:~:text=Approximately%2057%25%20of%20PWS%20patients,suffer%20from%20 obstructive%20sleep%20apnea
21.Lo, Bue A, Salvaggio A, Insalaco G. Obstructive sleep apnea in developmental age. A narrative review. European Journal of Pediatrics. 2020;179(3):357-365. DOI: 10.1007/s00431-019-03557-8
22.Tobin M. Breathing abnormalities during sleep. Archives of Internal Medicine. 1983;143(6):1221-1228. DOI: 10.1001/archinte.143.6.1221
23.Claire McCarthy M. A tired child? what you should know [Internet]. 2020 Available from: https://www.health.harvard.edu/blog/a-tired-child-heres-what-to-think-about-2018041713672
24.Stages of sleep: What happens in a sleep cycle [Internet]. 2023 Available from: https://www.sleepfoundation.org/stages-of-sleep
25.Professional CC medical. Sleep apnea: What it is, causes, symptoms & treatment [Internet]. 2022. Available from: https://my.clevelandclinic.org/health/diseases/8718-sleep-apnea
26.Parasomnias in children [Internet]. 2012. Available from: https://bestpractice.bmj.com/topics/en-us/117 7
27.Understanding the apnea-hypopnea index (AHI) [Internet]. 2023. Available from: https://www.sleepfoundation.org/sleep-apnea/ahi#:~:text=Mild%3A%20Children%20with%20an%20AHI,diagnosed%20with%20severe%20sleep%20apnea
28.Gipson K, Lu M, Kinane B. Sleep-disordered breathing. Surgery for Sleep-Disordered Breathing; 1(1):1-2. doi: 10.1007/3-540-27608-4_1
29.Savini S, Ciorba A, Bianchini C, Stomeo F, Corazzi V, Vicini C, et al. Assessment of obstructive sleep apnoea (OSA) in children: an update. Acta Otorhinolaryngologica Italica. 2019;39(5):289-297. DOI: 10.14639/0392-100x-n0262
30.Umano GR, Rondinelli G, Luciano M, Pennarella A, Aiello F, di Santo M, et al. Pediatric sleep questionnaire predicts moderate-to-severe obstructive sleep apnea in children and adolescents with obesity. Children. 2022;9(9):1303. DOI: 10.3390/children9091303
31.Gozal D, Tan H-L, Kheirandish-Gozal L. Treatment of obstructive sleep apnea in children: Handling the unknown with precision. Journal of Clinical Medicine. 2020;9(3):888. DOI: 10.3390/jcm9030888
Written By
Elizabeth Jones
Submitted: 17 July 2023Reviewed: 17 July 2023Published: 18 September 2023
 Open access peer-reviewed chapter
Open access peer-reviewed chapter