 Open access peer-reviewed chapter
Open access peer-reviewed chapter
Abstract
This chapter discusses the current landscape of Atopic Dermatitis treatment pathways and management of disease progression. Data leveraged for these types of analyses can come from disease-based communities, otherwise known as patient registries. Disease-based communities can work with participating healthcare institutions and enroll qualified patients to aid understanding of the population and sub-cohorts’ characteristics, as well as therapy protocols and regimens, time to and on therapy, discontinuation trends and reasons, and healthcare outcomes. Since the data collection includes Electronic Healthcare Records (EHRs) with the ability to append patient reported outcome questionnaires, as well as any other data sources relevant to the condition being studied, the resulting datasets provide in-depth insights on the patient population and their treatment pathways. Treating physicians are the Principal Investigators, managing and monitoring the patients’ progression and treatment. The reader is able, as a result, to learn the current preferred treatment pathways in treating Atopic Dermatitis, management of disease progression, as well as understand the underlying patient characteristics and historical medical information that drive the selection of therapies.
Keywords
- atopic dermatitis
- AD treatments
- disease-based communities
- patient registries
- patient data processing
1. Introduction
Natural history studies and studies initiated to fulfill regulatory authority post-marketing requirements and post-marketing commitments are designed to mitigate medical and clinical knowledge gaps. However, both types of studies can be costly, slow to enroll, and inefficient in their design, as they usually are focused on a single subpopulation and may be obsolete, if or when they are completed. In contrast, using real-world data (RWD) to develop the body of evidence for disease natural history and to provide additional safety and effectiveness information needed by post-regulatory decision makers can expedite access to enhanced insights, and benefit new therapies for a broad range of patients [1]. Thus, innovative methods to acquire RWD that rapidly inform clinicians, patients, regulatory agencies, and payers are needed.
Autoimmune diseases are a broad family of immune-mediated and inflammatory diseases, which are chronic and multi-systemic. Despite being life-long in nature, in many cases, disease progression can be slowed or prevented. Unfortunately, in some instances, treatment is ineffective, and the disease is ultimately irreversible, debilitating and potentially, even life ending. According to the National Institutes of Health, over 23 million Americans have an autoimmune disease [2]. More than 1 million adults are estimated to have rheumatoid arthritis (RA); 7.5 million have psoriasis (PsO); 204,000 have systemic lupus erythematosus (SLE); 53,000–248,000 are diagnosed with Sjogren’s Syndrome (SS); between 330,000 to 1.6 million are estimated to have ankylosing spondylitis (AS); and from 330,000 to 660,000 have psoriatic arthritis (PsA) [3, 4, 5, 6, 7, 8, 9].
Immune-mediated inflammatory skin conditions (IMISCs) are a subset of autoimmune diseases, and include atopic dermatitis (AD), PsO, hidradenitis suppurativa (HS), vitiligo, alopecia areata (AA), chronic spontaneous urticaria (CSU), and dermatomyositis. These are chronic, inflammatory disorders affecting the skin and appendages. They constitute a substantial financial burden on the U.S. health care system [10] and are among the greatest contributors to the burden of skin disease worldwide [11].
The etiologies of IMISCs are still being elucidated and are thought to be related to a combination of factors, including genetic susceptibility, social and environmental exposures, immune abnormalities, and skin barrier aberrations. IMISCs can affect individuals of all ages and typically wax and wane over time, with asymptomatic periods that may span days to decades. For example, AD often presents early in childhood with intense itching and recurrent eczematous skin lesions. Originally regarded as a childhood disorder mediated by a T-helper-2 dominated inflammatory response. AD is now recognized as a lifelong disposition with variable clinical manifestations [12]. Defects of the epidermal barrier, immune dysregulation, and environmental factors are thought to affect disease expression over time [13].
Selection of therapies for IMISCs is based upon various characteristics, including patient preferences, location and type of involvement, and risk factors for more severe disease. The pharmacologic options for management of IMISCs have expanded greatly over the past 15 years, based on growing knowledge of the immune pathways involved, with further expansion expected over the next decade. Prior to 2003, when the first biologic agents were FDA approved for the treatment of psoriasis, medical therapies had consisted of topical emollients and corticosteroids, phototherapy, and non-specific immunosuppressive treatments such as methotrexate and cyclosporine. Since that time, treatment patterns have shifted toward more targeted therapies [12, 13].
This chapter is focused primarily on atopic dermatitis (AD) and presents the current market condition, treatment pathways, and changing treatment environment. In the United States, the reported prevalence of AD in adults is 5% and that for children ranges from 10 to 20% [14, 15]. Symptoms of AD include pruritis, xerosis, lichenification, and sleep disturbance. In infants and young children, skin findings typically occur on the scalp, face, and extensor surfaces of the extremities. Older children and adults typically have involvement of the flexor surfaces, neck, wrists and ankles [16].
Risk factors for the development of AD include filaggrin gene mutations and family history of atopic or allergic disease [17]. Flares of AD are triggered by irritants, such as soaps, and allergens, such as food allergies. Comorbid diseases that are associated with AD include asthma, attention-deficit hyperactivity disorders (ADHD) and autism spectrum disorder (ASD) [18].
There are several challenges associated with drug discovery in autoimmune diseases, including the limited understanding of the biology and natural-history of each specific disease, as well as the appropriate targets for disease-modifying therapies. This is further complicated by a lack of early diagnosis. It has been shown that early intervention in autoimmune disease generally leads to better outcomes and that aggressive treatments can often halt disease progression. The concept of treat-to-target to track progress toward a predefined outcome and adjust dosing, accordingly, has also been a growing influence on autoimmune disease treatment for more than a decade, yet in some cases is not recommended.
Many of the same categories of medicinal treatment are used across the autoimmune diseases, including dermatological conditions, another indicator of a possible common etiology. Treatments frequently assessed in studies include:
NSAIDs, non-steroidal anti-inflammatory drugs (e.g., acetaminophen and meloxicam)
Corticosteroids (CCS, e.g., prednisone and methylprednisolone)
Disease Modifying Anti-Rheumatic Drugs (DMARD)
Immunosuppressants and conventional synthetics (csDMARD): Azathioprine, Cyclosporine, Cyclophosphamide, Hydroxychloroquine (anti-malarial), Leflunomide, Methotrexate, Mycophenolate mofetil, Sulfasalazine, Calcineurin inhibitors
Biologic inhibitors (bDMARD): IL-17, IL-23, B-Cell, CTLA4, TNF, BLyS/BAFF
Targeted Small Molecules (tsDMARD): Janus kinase inhibitors, PDE-4 inhibitors
Other IMISC therapies: topical emollients, phototherapy
Due to the prevalence of autoimmune diseases, there is an increasing need to develop multiple pathways that unlock the potential of real-world data (RWD) and real-world evidence (RWE) to improve patient outcomes and inform clinical trial design, especially in underserved patient populations. The current approach to healthcare is informed mostly by clinical trials with sample sizes in the hundreds or few thousands, which limits generalizability to broader patient populations and can be impractical due to costs and feasibility. In 2020, FDA issued a draft guidance identifying that there are a number of underserved patient groups (e.g., ethnic minorities, women, elderly, those at the extremes of weight range, individuals with organ dysfunction, those with malignancies or certain infections such as HIV, and children) who are routinely excluded from trials without sufficient clinical or scientific justification [19]. The exclusionary nature of our current healthcare system limits the generalizability of the study results to the wider population. Furthermore, in 2022, FDA released another draft guidance, encouraging sponsors of drug trials to outline a Diversity Plan as part of their submissions. In particular, when data suggest a difference in performance of the product based on factors related to race or ethnicity, the Diversity Plan should specify a roadmap for informing safety and effectiveness for each relevant population [20].
The rapid integration of Electronic Health Records (EHRs) has made longitudinal clinical data available for research, making real-world data (RWD) and the real-world evidence (RWE) derived from them an increasingly important tool in modern healthcare systems [21]. By aggregating real-world health and disease information from tens of thousands to hundreds of thousands or more diverse patients via EHR systems, the scale and scope of studies of a wide range of diseases, both common and rare, are improved by adding statistical power to detect associations between various complex factors and a wide variety of outcomes. The increasing utilization of RWD is further enhanced by the growing sophistication of epidemiologic and statistical methods that can facilitate principled learning. These include the development and refinement of causal inference methods, which permit the control of large numbers of covariates, and extend naturally to complex, longitudinal data, which allow (under certain assumptions) for the estimation of the effects of different care pathways for chronic disease [22, 23, 24, 25, 26, 27, 28, 29, 30, 31]. Recent guidance issued by the FDA regarding the utilization of RWE to facilitate drug development underscores the importance of these data sources [32].
As a result of the importance of understanding the autoimmune diseases, this chapter leverages RWD in the form of disease-based communities, otherwise known as patient registries, and presents the current market landscape for AD and available treatment options.
2. A disease-based community’s (patient registry) overview
In a disease-based community, otherwise known as a patient registry, patient level data is collected for the purpose of starting an observational research study. The objective of the community is to present a comprehensive review of outcomes for patients with specific diseases. The registry includes patients being managed for select diseases in usual clinical practice in the United States to address important clinical questions, regarding the management of these diseases by collecting and analyzing data from patients at a variety of academic medical centers and community medical practices. Practice patterns often vary by practice type, location, and the population treated, so the ability to study patients based on the specifics of their clinic type is useful. The study is designed to develop a robust database of real-world data regarding the natural history and health outcomes related to the management of diseases of diverse etiologies. Some examples of disease registries are shown in Figure 1. In the example below, the dermatology community includes a subset of patients with AD [33].
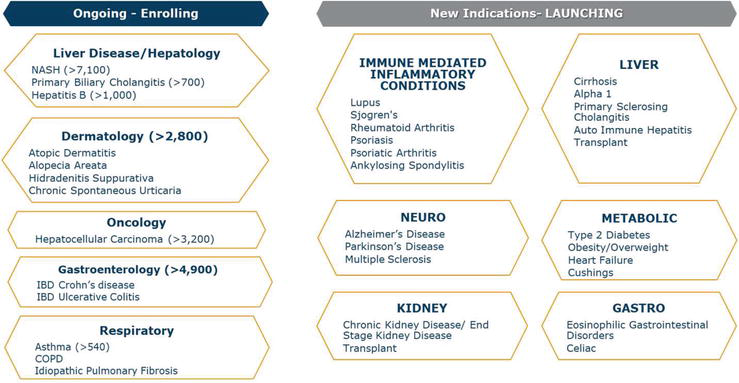
Figure 1.
Examples of currently available and upcoming disease-based communities.
The dermatology disease-based community enrolls patients from dermatology and allergy clinics that manage various dermatologic diseases, including AD, AA, HS, and CSU. Patients with AD are the primary focus of this chapter. The patients participating in a dermatology registry provide consent for their Electronic Health Records (EHRs) to be shared for research purposes. The data includes EHR for up to the prior 3 years retrospectively from the date of patient consent as well as prospective records. Prospective medical record collection continues for up to 15 years or until a study completion/exit criterion is met. The submitted records (structured and unstructured data) include but are not limited to inpatient and outpatient notes, pharmacy records, laboratory data, radiographic and procedure reports, histology reports, and all prior clinical details specific to screening methods, diagnostic evaluation, and treatment regimens for the studied conditions, along with associated comorbid conditions and complications [33].
The medical records include, but are not limited to [33]:
clinic notes/encounters and telephone contact notes/reports
laboratory, radiographic, imaging, or other reports
medication lists/pharmacy reports
hospitalization records
procedures
Records include all prior clinical details specific to screening methods, diagnostic evaluation, and treatment regimens of the respective dermatologic disease, including reasons for premature discontinuation of any therapies and treatment response [33].
Patients can also consent to participate in Patient Reported Outcomes (PRO) surveys and health-related questionnaires. Patients may also be invited to optionally provide periodic biospecimens. Patients can be enrolled at a regularly scheduled clinic visit or consented remotely as is permissible by each site’s IRB [33].
Utilizing this approach for data collection provides an efficient solution to collect information about critical populations from real-world practice, often underrepresented in clinical trials and disadvantaged in the US healthcare system. The concept is to avoid influencing practice patterns, instead capturing the standard of care at the given sites. The data also informs natural history studies and may provide a post-marketing safety and effectiveness surveillance platform that is otherwise impracticable from consented cohorts. It may also provide a platform from which to identify deficiencies in care, determine best practices, and evaluate patient and health outcomes in special subpopulations with the potential to improve the overall quality of care for patients with autoimmune diseases [33].
For the purpose of the chapter, the following AD diagnosis codes are leveraged: L20-L20.9; H01.131-139 atopic dermatitis/eczema, various.
3. Patient reported outcomes for atopic dermatitis
A patient-reported outcome (PRO) has been defined as
Self-reported patient health measures collect information directly from patients/caregivers to measure physical, mental, and social health in their disease state and during treatment. These measures can be used to help clinicians better understand how various treatments affect what patients are able to do and the symptoms they experience beyond what is typically derived from traditional clinical measures. The information can also be used to help patients make informed decisions about their healthcare and treatment options. Both the PROMIS initiative (Patient-Reported Outcome Measurement Information System) from the NIH and PCORI (Patient Centered-Outcomes Research Institute) have highlighted the need to implement patient centered measures into health care delivery. As a result, many healthcare organizations are implementing patient reported outcomes instruments as part of the standard patient intake for clinical visits and management [35].
In evaluating Atopic Dermatitis, outcomes data are sometimes collected at clinical visits to measure response, or lack of response to treatment, and can sometimes be reflected in routine clinical documentation. Types of information collected can include data about itch, location, itch frequency and severity and sleep disturbance. Other disease-specific PROs that are not part of routine clinical care may be collected through additional questionnaires at the start of the study and at regular follow up intervals. These may also include data on quality of life, neuropsychiatric (depression and anxiety) measures, how the condition may or may not impair work function, etc., as these are not only important to understanding the condition but can also sometimes affect treatment outcomes. There are many PROs available for AD, including the examples below [35].
Data on diagnosis can be collected through the U.K. Working Party Criteria (UKWPC) [36, 37], while data related to itch is captured through the Patient Oriented Eczema Measure (POEM) [38], which has been previously used in treatment trials for Atopic Dermatitis and other inflammatory skin disease states. The Patient-Oriented-SCORing Atopic Dermatitis (PO-SCORAD) [39] captures data related to severity. The Atopic Dermatitis Control Tool, (ADCT) [40] data related to itch, sleep, and quality of life. Itch, pain, and sleep can also be assessed by numeric rating scales. Quality of life, work impairment, and anxiety and depression can be assessed using the Dermatology Life Quality Index (DLQI) [41], Work Productivity and Impairment Questionnaire (WAPI) [42], or the PROMIS “PIQ” Short Forms, respectively [42].
The Children’s Dermatology Life Quality Index (CDLQI) [43] and the Infants Dermatitis Quality of Life Index (IDQOL) [44] are validated tools that assess disease activity in infants, children, and adolescents. The PROMIS Pediatric Scales assess anxious and depressive symptoms in children, as well as those related to sleep and itch [44].
In addition to patient reported outcome measures, Clinician Reported Outcomes (ClinROs) are an important data point in all disease areas. In AD, ClinROs are particularly important, given the scarcity of detail in clinician notes. Two of the most widely used ClinROsin AD include the Eczema Area and Severity Index (EASI) and the validated Investigator Global Assessment for Atopic Dermatitis (vIGA-AD) [45]. The EASI evaluates the severity of disease using an area score in each body region. The vIGA looks at overall severity of AD at the time of the exam. At times, clinicians also estimate a body surface area (BSA), the percent of skin affected by AD at the time of the exam [45].
4. Patient data processing overview
The patient registry provides a small-footprint data acquisition engine to process the EHR source (structured and unstructured data) of patients and export it from sites. The process typically is executed within the site firewall but can also be performed under secure protocols at managing organization or even at a mutually agreed Trusted Third Party (TTP) [33].
The data is standardized, pre-processed, and packaged behind the site firewall before being securely transmitted to the technical platform. The preprocessing and standardization steps allow for “at source” validation of the data elements extracted from the upstream system. Patient data from the sites is transmitted at frequent fixed intervals (weekly/monthly) and each site has a deterministic update schedule so that missing data receipts can be flagged [33].
This approach provides an EHR-agnostic strategy and utilizes a standard extract/report format most frequently available for the site’s EHR system, such as the Fast Healthcare Interoperability Resources (FHIR) standard. Such standard data extract formats will reduce ongoing support required by the sites technical team [33].
5. Methodology overview
Descriptive summaries are the basis of reporting used to support any insights derived in this chapter.
Numeric measures, including shifts from baseline, if possible, are summarized with the available number of patients (n), median, minimum, and maximum values. The mean, standard deviation, standard error, quartiles, inter quartile range, and number of missing observations may optionally be reported. Applicable figures include histograms, box plots, scatter plots, mean ± standard deviations, and mean ± standard errors.
Categorical descriptive measures are summarized with counts and percentages. The denominator in fixed category variables will be the number of patients with an observed result. The denominator for medication or defined event summaries represents all patients who could have had an observation. Defined events may also include the total number of events or the events per period. Cumulative event rates may be calculated using Kaplan-Meier methods.
6. Atopic dermatitis current market landscape overview
Through a series of quarterly reported summary statistics and insights, a snapshot of the AD patient registry is published every 3 months over the course of the registry. Patients included in the study started enrolling in January 2019 and have data from up to 3 years prior to that date, so the AD dataset captures several years of longitudinal data, including any events available post diagnosis. The below write up summarizes key insights from the currently available AD data.
In the Dermatology disease-based community cohort, there are currently 3559 participants enrolled in the US and Canada, of whom 2774 are included in the atopic dermatitis cohort. Of those, 2755 (99%) are included in this chapter market assessment. There are 53 active sites and 7 closed sites. The participants in this report represent 50 sites in the US and Canada; 25 of these sites are community and 25 are academic. A well-balanced sample of sites is important in ensuring unbiased insights.
One goal of registry studies is to be more representative of diverse populations than randomized clinical trials are able to be. Demographic summary statistics present the sex and racial/ethnic breakdown of the cohort. For example, there are 1514 female participants (55%) and 1241 male participants (45%). 1495 participants represent adults in the sample. There are 1428 White (52%), 346 (13%) African American, 15 (0.5%) American Indian or Alaskan Native, 18 (1%) Native Hawaiian or Other Pacific Islander, and 244 (9%) Asian participants. There are 19% Hispanics of any race in the cohort. The sex and racial/ethnic breakdown present similar ratios as noted in other registry studies [14, 15]. Systematic reviews of randomized clinical trials have shown a lag in terms of transparency of race and ethnicity reporting in dermatology studies; this has started to shift [46].
In addition, therapies taken at any time are reported by age group and organized by systemic therapy, topical therapy, and phototherapy. The recently approved JAK inhibitor and monoclonal antibody therapies, for instance, are tracked over time; there is great interest in observing the uptake of these therapies in the registry to understand the changing trends in treatments. Over time, sequencing of therapies will also be followed and reported. In addition, trends in topical therapy use are documented. Some therapies, like corticosteroids, are reported in multiple sections, as their route of administration includes both a systemic and topical option.
In this cohort, which is enriched by patients with moderate-to-severe disease, both systemic and topical therapies are widely prescribed. For the systemic therapies, antihistamines—often available over the counter—are often used, with hydroxyzine being the most frequently dosed treatment. Hydroxyzine is the only first-generation antihistamine that is recommended for AD. Monoclonal antibodies such as dupilumab are also used in this patient population [47]. Adults have a higher share of dupilumab use when compared to pediatric patients, which is likely due to the earlier approval date for adults. More recently, several other systemic biologic therapies have gained approval in the United States and other parts of the world. These therapies include tralokinumab, which is another monoclonal antibody, and upadacitinib, abrocitinib, and baricitinib, which are janus-kinase inhibitors (JAK-inhibitors). With regard to topical therapies, crisaborole (a phosphodiase-4 inhibitor) and ruxolitinib (another JAK-inhibitor) are creams that are approved for mild to moderate patients with AD. In addition, other topical therapies include calcineurin inhibitors and topical antibiotics. Finally, the vast majority of patients take either systemic or topical corticosteroids. Please note that the share of drug utilization often varies by the patient segment and the corresponding disease severity. As additional patient data is collected, more in-depth trends will be reported, including as noted above sequencing of treatments.
Most often prescribed concomitant therapies include treatments for health issues related to the respiratory system, alimentary track and metabolism, nervous system, and cardiovascular system. AD patients also often experience other types of allergic diagnoses from allergies to grass, weed and tree pollen, dust mice, food such as milk, nuts, and gluten to allergies to pets. While there are several different types of allergies, many of them are only experienced by a small percent of patients. As noted in other articles, the findings confirm previously found insights that comorbid diseases that are associated with AD include asthma and depression, but not noted in this analysis, attention-deficit hyperactivity disorders (ADHD) and autism spectrum disorder (ASD) have also been found to be associated [18].
Another important statistic shows the ClinRO responses at the time of the quarterly report (Figure 2). It is important to note the distribution of vIGA-AD severity score, which includes patients with clear or almost clear skin alongside patients with more severe categories of AD. Interestingly, this measure does not account for the type of therapy the patient was taking at the time of the clinician assessment. For example, a patient on dupilumab, who previously had severe AD, but is now well-controlled on therapy, might be reported to have a clear vIGA-AD score. In analyses, factors like this can be accounted for and worked into other reports. The summary results are intended to be idea-generating, and to encourage thoughts for analyses and publications on the registry data.
As shown in Figure 2, based on the validated Investigator Global Assessment for Atopic Dermatitis (vIGA-ADTM) at study enrollment, 216 (8%) were rated as clear, 381 (14%) as almost clear, 738 (27%) as mild, 1046 (38%) as moderate and 364 (13%) as severe.
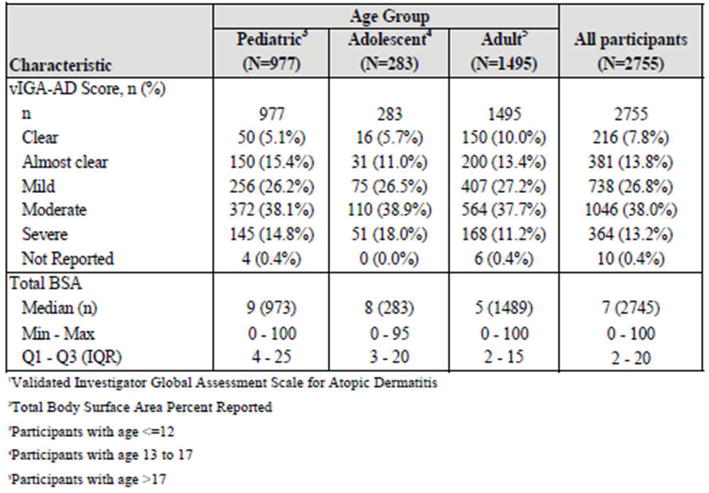
Figure 2.
vIGA-AD1 and total BSA2 status at enrollment by participant type.
It is important to note that while initially open to all patients being managed for AD, the AD patient enrollment is currently limited to patients who met the following targeted criteria: those with a vIGA score of moderate or severe at the time of enrollment, those who are currently on a biologic therapy or one of the following systemic treatments (methotrexate, cyclosporine, mycophenolate mofetil, novel biologics/JAK inhibitors and oral steroids) and those with a history of moderate or severe chronic AD, as supported by documentation in the available retrospective medical records. The reason for these targeted criteria is to enhance the population of patients who are eligible to receive treatment with the newer systemic therapies entering the market. Information on their performance in the real world is critical.
There is also great interest in seeing many of the summary statistics broken out by age group. Not only are different age groups affected by AD in unique ways, but therapies are also approved for different age groups at different times. So, for example, a new therapy might be available for adults prior to its label extending to adolescent or pediatric patients.
Finally, there is also interest in seeing summary statistics broken out by the site setting. In a well-balanced registry, patients will come from both community and academic sites. For this reporting period includes 1495 adult participants; 506 (31%) of the adult participants are enrolled at academic study sites and 989 (66%) are enrolled at community sites. This summary report includes 1260 pediatric patients; 635 (50%) of the pediatric participants are enrolled at academic study sites and 625 (50%) are enrolled at community sites.
7. Conclusions
This chapter introduced the concept of disease-based communities, otherwise known as patient registries and presented the AD market assessment based on to date available data to date. Patient registries are an important collection model of medical records that allow for receiving in-depth insights related to the patient diagnoses and treatment pathways as well as overall patient journey. The data provides a variety of data elements, such as clinic notes, laboratory, radiographic, imaging reports, prescribed medication lists, and diagnostic procedures and results. The level of granularity of the data is not always found in the healthcare claims, remittance, pharmacy adjudicated information, and primary market research datasets. The information can aid the understanding of patient outcomes, disease progression, and best pathways for treatment application, and fill in missing gaps from the other data sources. The deeper understanding of the AD diagnostic and treatment patterns, as a result, can help deploy strategies to optimize the care process, ultimately improving patient quality of life and final outcomes.
The overall disease-based community insights present that most patients’ diagnoses with AD are treated with at least a topical drug application, but often also systemic therapies such as antihistamines, monoclonal antibodies, and JAK-inhibitors. In addition, a small percent of patients has other allergies and are treated for a variety of comorbid conditions such as respiratory and cardiovascular diseases. Female patients represent a slightly higher percentage of AD patients in this registry, while from race/ethnic breakdown, ‘White’ patients represent half of the studied sample.
As noted earlier, due to still relatively small sample size in the patient registry, the level of insights presented in this chapter is limited. Future research will include reporting trends in combinations of therapies, reasons for discontinuing therapies, response to treatment over time, subsets of the population that respond to various therapies, PROs, and ClinROs over time and in relation to therapy starts.
Furthermore, with the larger sample, ability for inferential analysis vs. just descriptive statistics reporting will be available to provide additional insights into the data elements, impacting the diagnoses, disease progressions, and types of treatment prescribed. Survival analytics and adherence analytics represent examples of analytics that could be applied to the larger dataset. Other examples of analytics include predictive analytics, next best action analytics, and other marketing and management sciences analyses.
Acknowledgments
Authors would like to thank Keith Knapp, PhD, Target RWE, Durham, NC, USA for his contribution to this book chapter.
Nomenclature
Alopecia Areata | |
Atopic Dermatitis | |
Atopic Dermatitis Control Tool | |
Attention-Deficit Hyperactivity Disorders | |
Autism Spectrum Disorder | |
Ankylosing Spondylitis | |
Body Area Surface | |
Children’s Dermatology Life Quality Index | |
Clinician Reported Outcomes | |
Chronic Spontaneous Urticaria | |
Dermatology Life Quality Index | |
Electronic Healthcare Records | |
U. S. Food and Drug Administration | |
Fast Healthcare Interoperability Resources | |
Hidradenitis Suppurativa | |
Infants Dermatitis Quality of Life Index | |
Immune-Mediated Inflammatory Skin Conditions | |
Patient Oriented Eczema Measure | |
Patient-Oriented-SCORing Atopic Dermatitis | |
Patient Reported Outcomes | |
“PIQ” Short Forms | |
Psoriasis | |
Rheumatoid Arthritis | |
Real-World Data | |
Real-World Evidence | |
Systemic Lupus Erythematosus | |
Sjogren’s Syndrome | |
Trusted Third Party | |
U.K. Working Party Criteria | |
Validated Investigator Global Assessment | |
Work Productivity and Impairment Questionnaire |
References
- 1.
Abuabara K, Silverberg JI, Simpson EL, Paller AS, Eichenfield LF, Bissonnette R, et al. International observational atopic dermatitis cohort to follow natural history and treatment course: TARGET-DERM AD study design and rationale. BMJ Open. 2020; 10 (11):e039928. DOI: 10.1136/bmjopen-2020-039928. PMID: 33247014; PMCID: PMC7703415 - 2.
NIH Autoimmune Diseases Coordinating Committee: Autoimmune Diseases Research Plan, 2005. Available from: https://www.niaid.nih.gov/sites/default/files/adccfinal.pdf [Accessed: October 3, 2022] - 3.
Hunter TM, Boytsov NN, Zhang X, et al. Prevalence of rheumatoid arthritis in the United States adult population in healthcare claims databases, 2004-2014. Rheumatology International. 2017; 37 :1551-1557 - 4.
Rachakonda TD, Schupp CW, Armstrong AW. Psoriasis prevalence among adults in the United States. Journal of the American Academy of Dermatology. 2014; 70 (3):512-516 - 5.
Armstrong AW, Mehta MD, Schupp CW, Gondo GC, Bell SJ, Griffiths CEM. Psoriasis prevalence in adults in the United States. JAMA Dermatology. 2021; 157 (8):940-946 - 6.
Izmirly PM, Parton H, Wang L, McCune WJ, Lim SS, Drenkard C, et al. Prevalence of systemic lupus erythematosus in the United States: Estimates from a meta-analysis of the centers for disease control and prevention national lupus registries. Arthritis & Rhematology. 2021; 73 (6):991-996 - 7.
Maciel G, Crowson CS, Matteson EL, Cornec D. Prevalence of primary Sjögren’s syndrome in a US population-based cohort. Arthritis Care and Research (Hoboken). 2017; 69 (10):1612-1616 - 8.
Taurog JD, Chhabra A, Colbert RA. Ankylosing spondylitis and axial Spondyloarthritis. The New England Journal of Medicine. 2016; 374 (26):2563-2574 - 9.
Saalfeld W, Mixon AM, Zelie J, Lydon EJ. Differentiating psoriatic arthritis from osteoarthritis and rheumatoid arthritis: A narrative review and guide for advanced practice providers. Rheumatology and Therapy. 2021; 8 (4):1493-1517 - 10.
Lim HW, Collins SAB, Resneck JS Jr, Bolognia JL, Hodge JA, Rohrer TA, et al. The burden of skin disease in the United States. Journal of the American Academy of Dermatology. 2017; 76 (5):958-972.e2 - 11.
Hay RJ, Johns NE, Williams HC, Bolliger IW, Dellavalle RP, Margolis DJ, et al. The global burden of skin disease in 2010: An analysis of the prevalence and impact of skin conditions. The Journal of Investigative Dermatology. 2014; 134 (6):1527-1534 - 12.
Weidinger S, Novak N. Atopic dermatitis. Lancet. 2016; 387 (10023):1109-1122 - 13.
Leung DY, Guttman-Yassky E. Deciphering the complexities of atopic dermatitis: Shifting paradigms in treatment approaches. The Journal of Allergy and Clinical Immunology. 2014; 134 (4):769-779 - 14.
Barbarot S, Auziere S, Gadkari A, Girolomoni G, Puig L, Simpson EL, et al. Epidemiology of atopic dermatitis in adults: Results from an international survey. Allergy. 2018; 73 (6):1284-1293. DOI: 10.1111/all.13401 - 15.
Eichenfield et al. Atopic Dermatitis: Epidemiology and Pathogenesis Update. Seminars in cutaneous medicine and surgery. Elsevier Science; 2012; 31 :S3-S5 - 16.
McAleer MA, O’Regan GM, et al. Atopic dermatitis. In: Bolognia JL et al., editors. Dermatology. 4th ed. Vol. 208. China: Elsevier; 2018. p. 27 - 17.
Simpson et al. Update on epidemiology, diagnosis, and disease course of atopic dermatitis. Seminars in Cutaneous Medicine and Surgery. 2016; 35 :S84-S88. DOI: 10.12788/j.sder.2016.041 - 18.
Leung DYM et al. New insights into atopic dermatitis. Journal of Clinical Investigation. 2004; 113 (5):651-657 - 19.
U.S. Department of Health and Human Services, Food and Drug Administration et al. Enhancing the Diversity of Clinical Trial Populations—Eligibility Criteria, Enrollment Practices, and Trials Designs. Guidance for Industry. Rockville, MD: Food and Drug Administration; 2020. Available from: https://www.fda.gov/media/127212/download . [Accessed: October 3, 2022] - 20.
U.S. Department of Health and Human Services, Food and Drug Administration et al. FDA Takes Important Steps to Increase Racial and Ethnic Diversity in Clinical Trials. Guidance for Industry. Rockville, MD: Food and Drug Administration; 2022. Available from: https://www.fda.gov/news-events/press-announcements/fda-takes-important-steps-increase-racial-and-ethnic-diversity-clinical-trials . [Accessed: December 11, 2022] - 21.
NEJM CATALYST. Healthcare Big Data and the Promise of Value-Based Care. NEJM CATALYST: NEJM; 2018. Available from: https://catalyst.nejm.org/doi/full/10.1056/CAT.18.0290 . [Accessed: January 28, 2023] - 22.
Robins JM, Hernan MA, Brumback B. Marginal structural models and causal inference in epidemiology. Epidemiology. 2000; 11 :550-560 - 23.
An der Laan MJ, Robins JM. Unified Methods for Censored and Longitudinal Data and Causality. New York: Springer Verlag; 2002 - 24.
Schneeweiss S. Learning from big health care data. The New England Journal of Medicine. 2014; 370 :2161-2163 - 25.
Cepeda MS, Boston R, Farrar JT, Strom BL. Comparison of logistic regression versus propensity score when the number of events is low and there are multiple confounders. American Journal of Epidemiology. 2003; 158 :280-287 - 26.
Seeger JD, Walker AM, Williams PL, Saperia GM, Sacks FM. A propensity score-matched cohort study of the effect of statins, mainly fluvastatin, on the occurrence of acute myocardial infarction. The American Journal of Cardiology. 2003; 92 :1447-1451 - 27.
Seeger JD, Kurth T, Walker AM. Use of propensity score technique to account for exposure-related covariates: An example and lesson. Medical Care. 2007; 45 :S143-S148 - 28.
Brookhart MA, Reams D, Dluzniewski PJ, Kshirsagar A, Walsh L, Bradbury BD. Estimating the effect of preventable treatment discontinuation on health outcomes. Epidemiology. 2018; 29 :134-141 - 29.
Hernan MA, Lanoy E, Costagliola D, Robins JM. Comparison of dynamic treatment regimes via inverse probability weighting. Basic & Clinical Pharmacology & Toxicology. 2006; 98 :237-242 - 30.
Cain LE, Saag MS, Petersen M, et al. Using observational data to emulate a randomized trial of dynamic treatment-switching strategies: An application to antiretroviral therapy. International Journal of Epidemiology. 2016; 45 :2038-2049 - 31.
U.S. Department of Health and Human Services Food and Drug Administration Center for Drug Evaluation and Research (CDER). Real-world data: Assessing electronic health records and medical claims data to support regulatory decision-making for drug and biological products. Guidance for Industry. 2021 - 32.
Mishra P, Florian J, Peter J, Vainorius M, Fried MW, Nelson DR, et al. Public–private partnership: Targeting real-world data for hepatitis C direct-acting antivirals. Gastroenterology. 2017; 153 :626-631 - 33.
Target RWE. Partners for the Real World. Durham, NC: Target RWE; 2022. Available from: https://www.targetrwe.com/ . [Accessed: December 10, 2022] - 34.
U.S. Food and Drug Administration. Patient-reported outcome measures: Use in medical product development to support labeling claims. Guidance for Industry. Rockville, MD: Food and Drug Administration. 2009; 74 (35):65132-65133. Available from:https://www.fda.gov/regulatory-information/search-fda-guidance-documents/patient-reported-outcome-measures-use-medical-product-development-support-labeling-claims . [Accessed: December 9, 2022] - 35.
Target RWE. Patient Reported Outcomes—Site Starter Packet. Internal Company Marketing and Training Resources; 2022 [Accessed: December 10, 2022] - 36.
Williams HC, Burney PG, Hay RJ, et al. The UK working party’s diagnostic criteria for atopic dermatitis. I. Derivation of a minimum set of discriminators for atopic dermatitis. The British Journal of Dermatology. 1994; 131 :383-396 - 37.
Williams HC, Burney PG, Pembroke AC, et al. The UK working party’s diagnostic criteria for atopic dermatitis. III. Independent hospital validation. The British Journal of Dermatology. 1994; 131 :406-416 - 38.
Spuls PI, Gerbens LAA, Simpson E, et al. Patient-oriented eczema measure (POEM), a core instrument to measure symptoms in clinical trials: A harmonising outcome measures for eczema (home) statement. The British Journal of Dermatology. 2017; 176 :979-984 - 39.
Stalder J-F, Barbarot S, Wollenberg A, et al. Patient-oriented SCORAD (PO-SCORAD): A new self-assessment scale in atopic dermatitis validated in Europe. Allergy. 2011; 66 :1114-1121 - 40.
Simpson E, Eckert L, Gadkari A, Mallya UG, Yang M, Nelson L, et al. Validation of the atopic dermatitis control tool (ADCT©) using a longitudinal survey of biologic-treated patients with atopic dermatitis. BMC Dermatology. 2019; 19 (1):15. DOI: 10.1186/s12895-019-0095-3 - 41.
Basra MKA, Fenech R, Gatt RM, et al. The dermatology life quality index 1994-2007: A comprehensive review of validation data and clinical results. The British Journal of Dermatology. 2008; 159 :997-1035 - 42.
Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibility of a work productivity and activity impairment instrument. PharmacoEconomics. 1993; 4 :353-365 - 43.
Lewis-Jones MS, Finlay AY. The children’s dermatology life quality index (CDLQI): Initial validation and practical use. The British Journal of Dermatology. 1995; 132 :942-949 - 44.
Hanifin JM, Thurston M, Omoto M, et al. The eczema area and severity index (EASI): Assessment of reliability in atopic dermatitis. EASI Evaluator Group. Experimental Dermatology. 2001; 10 (1):11-18. DOI: 10.1034/j.1600-0625.2001.100102.x - 45.
Eli Lilly and Company. Validated Investigator Global Assessment. Used with the Permission of Eli Lilly and Company under a Creative Commons Attribution-No Derivatives 4.0 international license. 2017 - 46.
Chen V, Akhtar S, Zheng C, Kumaresan V, Nouri K. Assessment of changes in diversity in dermatology clinical trials between 2010-2015 and 2015-2020: A systematic review. JAMA Dermatology. 2022; 158 (3):288-292. DOI: 10.1001/jamadermatol.2021.5596 - 47.
Nowicki R, Trzeciak M, Wilkowska A, Sokołowska-Wojdyło M, Ługowska-Umer H, Barańska-Rybak W, et al. Atopic dermatitis: Current treatment guidelines. Statement of the experts of the dermatological section, polish Society of Allergology, and the allergology section, polish Society of Dermatology. Advances in Dermatology and Allergology. 2015; 32 (4):239-249. DOI: 10.5114/pdia.2015.53319